Download presentation
Presentation is loading. Please wait.

1
Dementia and Primary Progressive Aphasia (PPA) Differential Diagnosis Therapy approaches The Roles of Speech Language Pathologists
 Differential Diagnosis Therapy approaches The Roles of Speech Language Pathologists")
2
What we think about DEMENTIA Garbled speech Impulsive Forgetful Childish

3
Defining Dementia Dementia - a group of symptoms related to memory, and overall cognitive impairment. Most types of dementia continue to worsen and are irreversible. Alzheimer’s Disease- the most common type of dementia. Affects up to 80% of those diagnosed with dementia PPA - a form of dementia that involves a decline in language functions.

4
SIGNS/SYMPTOMS OF DEMENTIA Confusion Getting lost in familiar places Problems with personal affairs (housekeeping, finances, grooming) Personality changes Depression Difficulty following simple directions Significant memory loss Decreasing communication skills Dysphagia Increased muscle tightness/ rigidity. * Progressive loss begins many years before it is diagnosed.

5
How is Dementia diagnosed? A complete medical workup to r/o other causes of cognitive impairment such as drug interaction or multi-infarct dementia ( from several small CVA’s) Diagnosis team may include physician, neuropsychologist, SLP, OT, social worker, and family/friends/caregivers Testing to evaluate cognitive functioning
 Diagnosis team may include physician, neuropsychologist, SLP, OT, social worker, and family/friends/caregivers Testing to evaluate cognitive functioning.")
8
Medical history that can lead to dementia Huntington’s disease Multiple Sclerosis-auto immune demyelinating Infections such as HIV/Aids, Lyme disease Parkinson’s disease (30-40%). (new research – stim. Astrocytes in hippocampus ento rhinal area improved memory) Pick’s disease-Tau protein damage Progressive supranuclear palsy
 Pick’s disease-Tau protein damage Progressive supranuclear palsy.")
9
PPA Diagnosis How is PPA diagnosed? History: assess functionality by interviewing caregivers and family members regarding orientation, memory, executive function Medical history and results of other testing : neurological, psychological 1. Functional communication assessment ( an interview) 2. Cognitive Linguistic Quick Test 3. Aphasia testing 4. Oral / swallowing fx
 2. Cognitive Linguistic Quick Test 3. Aphasia testing 4. Oral / swallowing fx.")
10
Signs and symptoms Focal vs Diffuse Vary, depending upon the portion of the brain affected. Some people with frontotemporal dementia undergo dramatic changes in their personality and become 1.socially inappropriate, 2.impulsive or emotionally blunted, **while others lose the ability to use and understand language.

11
Medications may be prescribed, all have side effects To control behaviors : Antipsychotics (haloperidol,risperidone,olanzapine) Mood stabilizers (fluoxetine,imipramine,citalopram) Stimulants (methylphenidate To slow rate of symptoms: Aricept, Exelon, Razadyne,Namenda
 Mood stabilizers (fluoxetine,imipramine,citalopram) Stimulants (methylphenidate To slow rate of symptoms: Aricept, Exelon, Razadyne,Namenda")
12
Speech Evaluation + Speech and Language Evaluation: Since a decline in language abilities is the primary symptom of PPA A Speech-Language Pathologist evaluates different aspects of language in detail and can make recommendations for strategies to improve communication. Family members should be included in the treatment sessions to educate them about how to facilitate communication and use functional strategies. What works? What doesn't Talk to family

13
Speech Evaluation Cont. The disorder has an impact on : relationships, the ability to continue working, the ability to perform many routine duties, and the ability to communicate even the simplest of needs. Although there are many resources available for individuals with memory loss, there are relatively fewer appropriate resources for individuals with PPA, their relatives and friends. Evaluation with a social worker who is familiar with PPA can address these issues and provide suggestions for dealing with day-to-day frustrations and problems. We may need to make recommendations for social worker to help them

14
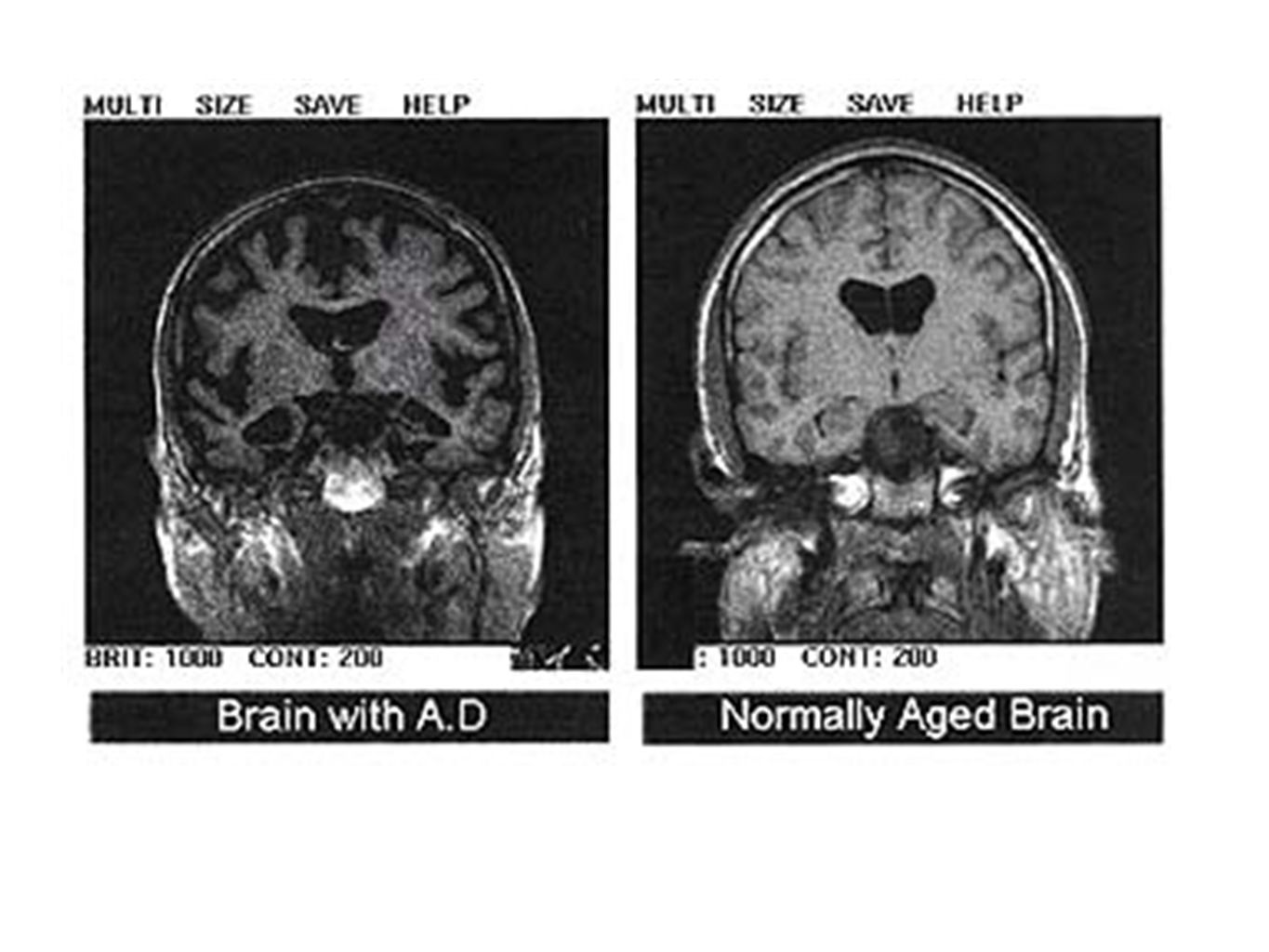
Brain Scan. MRI studies Normal brain PPA Brain

15
Treatment – Compensatory-Adaptive Treatment of Communication Impairments To improve the ability to communicate AAC? Notebook, post it's, enlarged calendar the type of language problems experienced by patients with PPA may vary, the focus of treatment for improving communication ability will also vary. At present, there is no cure for the degenerative diseases that cause PPA. Medical treatments are generally in the realm of managing behavioral symptoms such as depression, anxiety, or agitation, which may occur later in the course of the illness. Find the strongest Lang modalities

16
Clinicians are responsible for facilitating cognitive-communicative function Direct Interventions- spaced retrieval tasks, graphic and written cues in memory books. Indirect Intervention- environmental modifications Caregiver Training- repeat key information, give choices rather than open ended questions, keep information/questions short and simple, use written cues for activities (ie: getting dressed, preparing simple meal), encourage attendance at support groups, seek adult day cares for respite to prevent burn out.
, encourage attendance at support groups, seek adult day cares for respite to prevent burn out..")
17
Caregivers at home and in the SNFs Only 7% of the day in conversation 1.Only to do with ADL 2.Isolating = 3.Less need to communicate 4.Diminishing skills>reduced Stim> What to do as an SLP? Educate the people around the client Follow up on interactions *

18
Speech Therapy Approaches There are 2 basic approaches to treatment for PPA and the dementias that must always include training the caregivers 1.Direct Treatment: focus treatment directly on ways to improve the functional memory, language, pragmatic skills that are impaired 2.Compensatory &. adaptive *It is recommended that both treatment approaches be used with PPA patients. Beginning in early stages of the disease, treatment should be provided to enhance verbal language skills. For example, treatments focused on word-retrieval skills may be helpful. Treatment focused on the use of augmentative/alternative communication strategies also should be provided, even in the early stages of PPA. These are strategies that either enhance verbal communication or replace it. What are some examples?

19
Direct intervention : Calendars Dry erase boards Labels in the living space Visual memory activities Auditory memory activities Vocabulary and sequences associated with pragmatic skills and ADL

20
Set up strategies for the future Small notebook with pictures and words Apps for communication Find out the best modality and use it to assist Pictures Gesturing Tags around the house Consistent routines

21
Family or caregiver involvement The patient (and family members) be trained in augmentative/alternative communication and functional strategies such as: Use of a communication notebook/ smart pad Use of gestures Use of drawing Share. In simple terms results : Speech eval How client uses AAC or other fx adaptive materials However, follow-up treatment with a Speech-Language Pathologist is important in order to further develop the strategy and provide practice in using it. Practicing daily routines needs to be emphasized

22
Areas of cognition to assess and stimulate 1.Orientation - days,seasons, direction, 2.Attention- focus,,memory, distractions, redirectability 3.Sequences- ADL, recreation 4.Categories - by function, place etc 5.Ability to use strategies,communication books or smart pads

23
For nonprogressive cognitive loss due to other neurological impairments Assess functional language and cognition Follow similar procedure as for PPA Stimulate cognitive function along all parameters in the areas of cognition ?

24
1. Mild cognitive impairment: deficits in cognitive domains other than memory. Ribeiro F, de Mendonça A, Guerreiro M. Dement Geriatr Cogn Disord. 2006;21(5-6):284-90. Epub 2006 Feb 10. PMID: 16484806 [PubMed - indexed for MEDLINE] Related citations 2. Verbal learning and memory deficits in Mild Cognitive Impairment. Ribeiro F, Guerreiro M, De Mendonça A. J Clin Exp Neuropsychol. 2007 Feb;29(2):187-97. PMID: 17365254 [PubMed - indexed for MEDLINE] Related citations 3. Frontotemporal mild cognitive impairment. de Mendonça A, Ribeiro F, Guerreiro M, Garcia C. J Alzheimers Dis. 2004 Feb;6(1):1-9. PMID: 15004322 [PubMed - indexed for MEDLINE] Related citations 4. Clinical significance of subcortical vascular disease in patients with mild cognitive impairment. de Mendonça A, Ribeiro F, Guerreiro M, Palma T, Garcia C. Eur J Neurol. 2005 Feb;12(2):125-30. PMID: 15679700 [PubMed - indexed for MEDLINE] Related citations 5. Mild cognitive impairment: focus on diagnosis. de Mendonça A, Guerreiro M, Ribeiro F, Mendes T, Garcia C. J Mol Neurosci. 2004;23(1-2):143-8. Review. PMID: 15126699 [PubMed - indexed for MEDLINE] Related citations 6. Memory complaints in healthy young and elderly adults: reliability of memory reporting. Mendes T, Ginó S, Ribeiro F, Guerreiro M, de Sousa G, Ritchie K, de Mendonça A. Aging Ment Health. 2008 Mar;12(2):177-82. PMID: 18389397 [PubMed - indexed for MEDLINE] Related citations
: Epub 2006 Feb 10. PMID: [PubMed - indexed for MEDLINE] Related citations 2. Verbal learning and memory deficits in Mild Cognitive Impairment. Ribeiro F, Guerreiro M, De Mendonça A. J Clin Exp Neuropsychol Feb;29(2): PMID: [PubMed - indexed for MEDLINE] Related citations 3. Frontotemporal mild cognitive impairment. de Mendonça A, Ribeiro F, Guerreiro M, Garcia C. J Alzheimers Dis Feb;6(1):1-9. PMID: [PubMed - indexed for MEDLINE] Related citations 4. Clinical significance of subcortical vascular disease in patients with mild cognitive impairment. de Mendonça A, Ribeiro F, Guerreiro M, Palma T, Garcia C. Eur J Neurol Feb;12(2): PMID: [PubMed - indexed for MEDLINE] Related citations 5. Mild cognitive impairment: focus on diagnosis. de Mendonça A, Guerreiro M, Ribeiro F, Mendes T, Garcia C. J Mol Neurosci. 2004;23(1-2): Review. PMID: [PubMed - indexed for MEDLINE] Related citations 6. Memory complaints in healthy young and elderly adults: reliability of memory reporting. Mendes T, Ginó S, Ribeiro F, Guerreiro M, de Sousa G, Ritchie K, de Mendonça A. Aging Ment Health Mar;12(2): PMID: [PubMed - indexed for MEDLINE] Related citations.")
25
7. J. Mol Neurosci. 2011 Nov;45(3):724-36. doi: 10.1007/s12031-011-9579-2. Epub 2011 Jun 28. Positive effects of language treatment for the logopenic variant of primary progressive aphasia. Beeson PM, King RM, Bonakdarpour B, Henry ML, Cho H, Rapcsak SZ. 8. Constantinidou, F., Thomas, R. D., & Best, P. J. “Principles of Cognitive Rehabilitation: An Integrative Approach”. Boca Raton, FL: CRC Press. ©2004. 9. Constantinidou, F., Thomas, R. D., Scharp, V. L., Laske, K. M., Hammerly, M. D., & Guitonde, S. (2005). “Effects of Categorization Training in Patients With TBI During Postacute Rehabilitation: Preliminary Findings” Journal of Head Trauma Rehabilitation Mar-Apr 2005, 143-157.
. Effects of Categorization Training in Patients With TBI During Postacute Rehabilitation: Preliminary Findings Journal of Head Trauma Rehabilitation Mar-Apr 2005,")
Similar presentations














 Training Intent: Welcome participants & introduce.>")
. TBI results from: Penetrating Closed head injury.>")




 THAT INTERFERES WITH ROUTINE DAILY ACTIVITIES. MENTAL.>")