Download presentation
Presentation is loading. Please wait.

1
2012/09/27 Combine meeting 58 y/o Female DCMP s/p ECMO s/p DFPP s/p LVAD 林柑 5305996

2
Brief History 2006---DCMP 2008---ICD 2010---Heart transplantation waiting list

3
58 yo Female DCMP with arrhythmia status post permanent pacemaker insertion. 2012/07/07 HsinChu H.: unsteady gait and aphasia. Con’s=E4M6Vt Brain CT: left cerebral subcortical infarction admission 2012/07/07-11: Progressive dyspnea, oliguria LVEF=4.6% Pulmonary edema with acute CHF 2012/07/11: Intubation, ECMO NTUH

4
Physical Examination (2012/7/11) Vital Sign: T:36.2 P:64 R:17 BP:108/84 mmHg General appearance: ill Consciousness: E4M6Vt HEENT: grossly normal Eyes: conjunctiva: not pale, sclera: not icteric Pupil Isocoric, light reflex (R/L): +/+, prompt Ears: eardrums not injected. Neck: supple, JVE (-), LAP (-) Chest: symmetric expansion, bil crackles (+), Heart: RHB, no murmur audible Abdomen: soft and flat, no superficial collateral circulations, No tenderness, no rebounding tenderness Bowel sounds: normal active Liver / Spleen: Not palpable Extremities: freely movable, pitting edema (+), cyanosis (-), petechiae (-), rash (-) left femoral ECMO (+)
, LAP (-) Chest: symmetric expansion, bil crackles (+), Heart: RHB, no murmur audible Abdomen: soft and flat, no superficial collateral circulations, No tenderness, no rebounding tenderness Bowel sounds: normal active Liver / Spleen: Not palpable Extremities: freely movable, pitting edema (+), cyanosis (-), petechiae (-), rash (-) left femoral ECMO (+).")
5
2012-7-11 X-ray

6
2012/07/12 EKG

7
2012/07/16 Cardiac Echo LVEF=14.6% global hypokinesia Moderate MR, TR, PR, Pulmonary Hypertension TRPG=50.7

8
CAVH on V-A ECMO AKI due to shock related CAVH on ECMO support Waiting for heart transplantation

9
Lab data 5.4 Donor Crossmatch + Unasyn Tatumcef

10
Cross match Date 4 ℃ T-cell37 ℃ B-cell4 ℃ T-cell37 ℃ B-cell HLA-ABCHLA-DR 2012-7-121:2 Positive 1:16 Positive 1:1 Positive 1:16 Positive 2012-7-19 A2 A24 B38 B46 Bw4 Bw6 Cw1 Cw7 DR17 DR19 DR52 DR53 DQ2 DQ9 2012-7-20 14:33 1:8 Positive 1:32 Positive 1:2 Positive 1:32 Positive 2012-7-20 20:41 Negative1:16 Positive Negative1:32 Positive 減敏感治療

11
Desenstitration Order

12
DFPP Protocol 1.2A 4A Separator 2.Volume : 1.5 X 3.30% 10% Extraction 4.Replacement Fluid : Nil

13
DFPP Course Volume /blood flow Duration Extraction (L) Complication 2012-7-262A 3500/100130 min0.26BP drop, wound oozing 2012-7-282A 3500/100134 min0.37BP drop, wound oozing 2012-7-302A 3500/100120 min0.42BP drop, wound oozing 2012-8-012A 2300/10077 min0.31 ?ABP straight line 2012-8-044A 3500/100120 min0.42Wound oozing 2012-8-074A 3500/100125 min0.36Wound oozing 2012-8-104A 3500/120120 min0.48Wound oozing 2012-8-144A 3500/100125 min0.44Wound oozing
 Complication A 3500/ min0.26BP drop, wound oozing A 3500/ min0.37BP drop, wound oozing A 3500/ min0.42BP drop, wound oozing A 2300/10077 min0.31 ABP straight line A 3500/ min0.42Wound oozing A 3500/ min0.36Wound oozing A 3500/ min0.48Wound oozing A 3500/ min0.44Wound oozing")
15
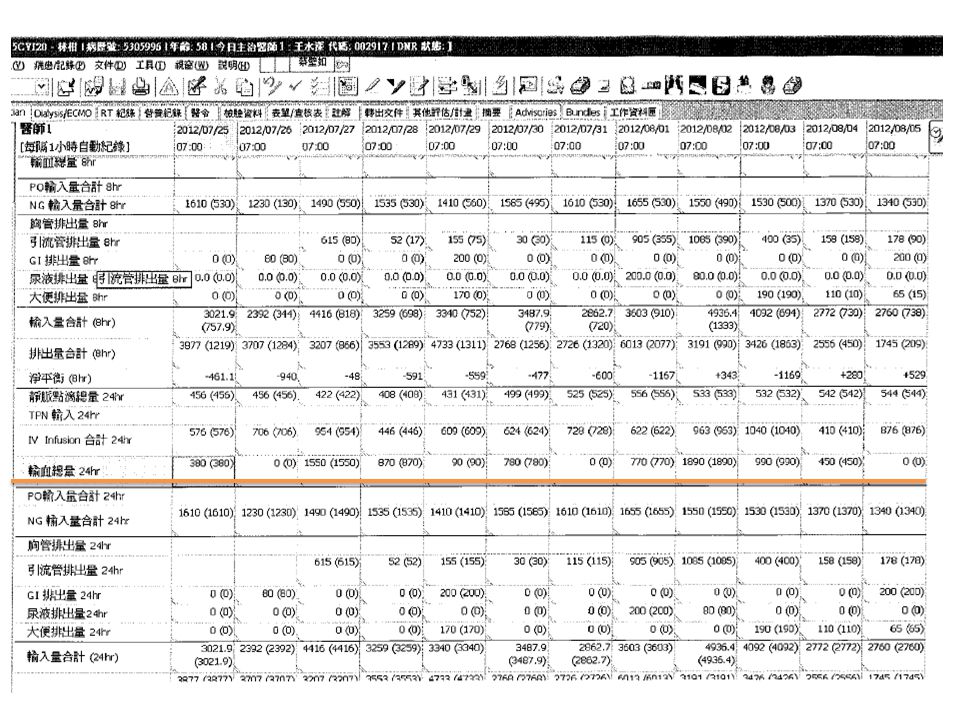
Treatment Course AlbuminFibrinogenTransfusionaPTT/INRHeparin 2012-7-233.5267.4 ﹡ 2012-7-26 129.8/23.7155037.3/1.09 ﹡ 2012-7-28 134.887033.9/1.110 2012-07-2998.931.0/1.220 ﹡ 2012-7-30 3.0112.978031.4/1.130 ﹡ 2012-8-01 72189031.7/1.040 ﹡ 2012-8-4 2.4198.145029.9/0.990 ﹡ 2012-8-7 152.440049.5/1.230 ﹡ 2012-8-10 1.993.681029.3/1.100 ﹡ 2012-8-14 2.4 / 36.773036.4/1.480 2012-8-1656.835.9/1.400

18
Donor Cross match Date 4 ℃ T-cell4 ℃ B-cell37 ℃ T-cell37 ℃ B-cell Anti-HLA class I Ab Anti-HLA class I I Ab Flow PRA Class I Flow PRA Class II 2012-7-12 1:2 Positive 1:16 Positive 1:1 Positive 1:16 Positive Negative 2012-7-19 Positive 2012-7-20 14:33 1:8 Positive 1:32 Positive 1:2 Positive 1:32 Positive 98.9674.47 2012-7-20 20:41 Negative1:16 Positive Negative1:32 Positive 2012-8-6 16:44 1:32 Positive 2012-8-15 99.7471.47 2012-8-29 1:1 Positive 1:8 Positive 1:1 Positive 1:4 Positive

19
問題 Blood flow ? Myocardium depression Fibrinogen consumption – Bleeding – Transfusion 輸血 – 避免輸血 – 前置作業

20
Treatment Course in 5CVI 2012/07/14 ECMO+CAVH, on HTx waiting list, PRA(+) 2012/07/25 Start Desensitization Protocol 7/25 Rituximab 200 mg iv stat with solu-medrol 40 mg st 7/26 DFPP(2A) with IVIG 7/26, 7/28, 7/30 8/1~14 DFPP (4A) with IVIG (QW2,5) 8 courses
 2012/07/25 Start Desensitization Protocol 7/25 Rituximab 200 mg iv stat with solu-medrol 40 mg st 7/26 DFPP(2A) with IVIG 7/26, 7/28, 7/30 8/1~14 DFPP (4A) with IVIG (QW2,5) 8 courses")
21
Treatment Course in 5CVI 2012/07/11-8/30: Waiting for Heart Transplantation (ECMO) ‧ Coagulopathy DFPP + IVIG for desensitization low fibrinogen, bleeding Thrombus formation s/p emergent evacuation *4 PRA(+) VT DC shock (7/29, 8/27,8/28)
 ‧ Coagulopathy DFPP + IVIG for desensitization low fibrinogen, bleeding Thrombus formation s/p emergent evacuation *4 PRA(+) VT DC shock (7/29, 8/27,8/28)")
22
2012/08/30 LVAD implantation OP Method: LVAD THORATEC implantation V cannula: beveled tip against septim through LV apex A cannula: 14mm graft end-to-side anastomosis to AsAo; then wrapped by 20mm Hemashield vascular graft.

23
Post-OP Course (2012/8/30) 2012/08/30 14:00 Thoratec blood flow: 6L/min CVP:24 mmHg, BP:45/42(43) mmHg Dopamine :9.4 µg/Kg/min Levophed: 1.63 µg/Kg/min, Isuprel : 0.2 µg/Kg/min 2012/08/30 18:00 BP↓ (48/41mmHg), device alarm: no flow EKG: bradycardia Lab: Hyperkalemia(K6.18) with metabolic cidosis (pH=7.05) s/p correction: BP 169/97, PH 7.546, K 2.90 Start CVVH
 2012/08/30 14:00 Thoratec blood flow: 6L/min CVP:24 mmHg, BP:45/42(43) mmHg Dopamine :9.4 µg/Kg/min Levophed: 1.63 µg/Kg/min, Isuprel : 0.2 µg/Kg/min 2012/08/30 18:00 BP↓ (48/41mmHg), device alarm: no flow EKG: bradycardia Lab: Hyperkalemia(K6.18) with metabolic cidosis (pH=7.05) s/p correction: BP 169/97, PH 7.546, K 2.90 Start CVVH")
24
Post-OP Course (2012/8/30) 2012/08/30-31 0:00 BP drop ↓77/52mmHg VAD alarm(+): poor drainage CVP 27 12 volume challenge! Dop+Isuprel+Levophed+ DC shock*2 CPR-> on ECMO

25
2012/8/30-31 ABG: lactate↑

26
Treatment Course in 5CVI 2012/08/31 Pupil dilatation, E1M1Vt BP:50/30mmHg Discuss with family about poor prognosis 2012/09/02 Remove ECMO and Thoratec, the pt expired at 11:10AM

28
問題 Blood flow ? Myocardium depression Fibrinogen consumption – Bleeding – Transfusion 輸血 – 避免輸血 – 前置作業

29
The decrease of patient blood volume was induced by an oncotic pressure drop due to albumin loss and often resulted in a pressure drop.

30
ECMO + DFPP

31
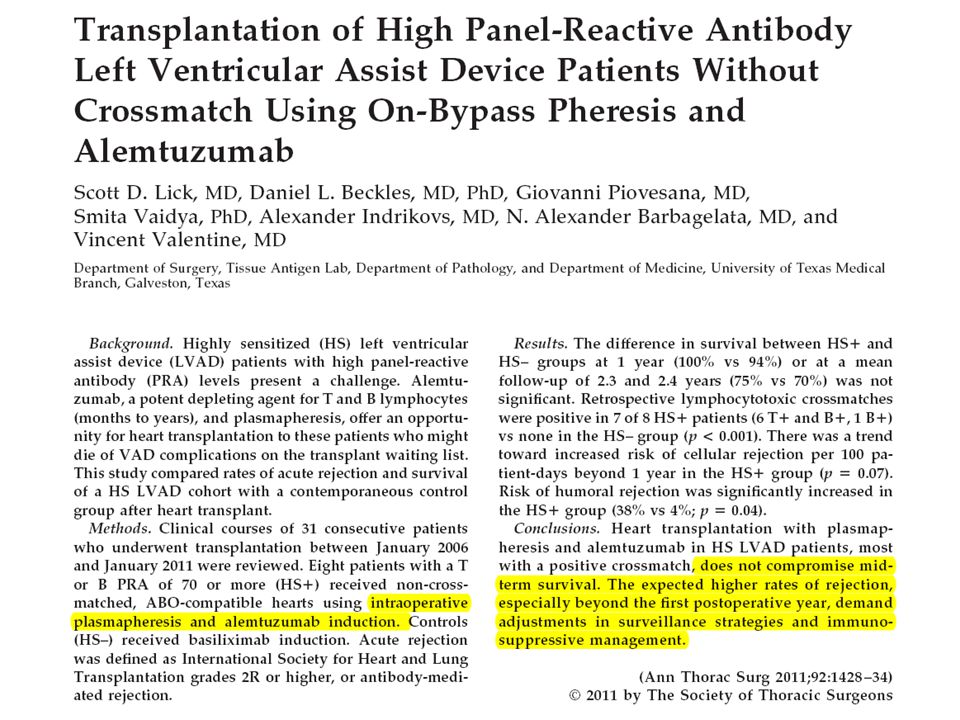
Intraoperative plasmapheresis and Cellcept induction Peri-operative alemtuzumab(Campath-1H) and plasmapheresis for high-PRA positive lymphocyte crossmatch heart transplant: a strategy to shorten left ventricular device support. – Department of surgery, University of Texas Medical Branch, Galveston. – J Heart Lung Transplant. 2008 Sep;27(9): 1036-9. Mortality and morbidity in pre-sensitized pediatric heart transplant recipients with a positive donor crossmatch utilizing peri-operative plasmapheresis and cytolytic therapy. – Department of Pediatrics, Washington University school of Medicine. – J Heart Lung Transplant. 2007 Sep;26(9): 876-82. Pediatric cardiac transplantation in children with high panel reactive antibody. – The Congenital Heart institute of Florida, All children’s Hospital, University of South Florida. – Ann Thorac Surg. 2004 Nov;78(5):1703-9
: Mortality and morbidity in pre-sensitized pediatric heart transplant recipients with a positive donor crossmatch utilizing peri-operative plasmapheresis and cytolytic therapy. – Department of Pediatrics, Washington University school of Medicine. – J Heart Lung Transplant Sep;26(9): Pediatric cardiac transplantation in children with high panel reactive antibody. – The Congenital Heart institute of Florida, All children’s Hospital, University of South Florida. – Ann Thorac Surg Nov;78(5):")
33
Protocol 3-volume exchange in 60-100 min, depending on the patient’s body size. Repaid removal of calcium and heparin sulfate during pheresis. The timing of the institution of CPB and pheresis is determined by the expected arrival of the donor heart.

34
Ann Thorac Surg 2011;92:1428-34

35
NTUH Plasma exchange during CPB

37
EvafluxPore sizeAlbumin sc IgG sc HDL sc IgM sc LDL 2A 0.01 ㎛ 0.620.190.1500 3A 0.02 ㎛ 0.70.350.2200 4A 0.03 ㎛ 0.850.550.500 5A 0.03 ㎛ (?) 0.920.850.830.10.02 移除目標為 IgG: 2A 或 3A (can remove Immunoglobulins while allowing Albumin to be returned) 移除目標為 IgM: 4A 或 5A 移除目標為 LDL: 5A (can remove LDL while allowing Albumin and HDL to be returned)
 移除目標為 IgG: 2A 或 3A (can remove Immunoglobulins while allowing Albumin to be returned) 移除目標為 IgM: 4A 或 5A 移除目標為 LDL: 5A (can remove LDL while allowing Albumin and HDL to be returned)")
38
楊正智 order

39
楊正智 DFPP

40
4/18 plasma exchange in OR

43
LVAD (Thoratec Heartmate VE) Pulsatile, LV assist Only. Fixed rate / Chamber filled (asynchrony) – Initiated with flow 2.2L/min/m 2, LAP 10-15mmHg Bridge to Heart Transplantation.
 – Initiated with flow 2.2L/min/m 2, LAP 10-15mmHg Bridge to Heart Transplantation..")
44
Manual Of Perioperative Care In Adult Cardiac Surgery Ch11 p.479

45
Contraindication Reasonable chance of recovery? – Age, medical condition, RV function, – Comorbidities ( neurologic, pulmonary, renal, hepatic) – Other medical issues ( infection, vascular disease, DM…)
 – Other medical issues ( infection, vascular disease, DM…).")
46
Post-LVAD management Adequate tissue perfusion – Assessed by mixed Venous oxygen saturation Decrease myocardial demand – Vasoactive medication only for RV function or increased SVR to keep MAP>75mmHg – “vasodilatory shock”

47
Complication Mediastinal bleeding, tamponade (60%) – Manifested by inadequate drainage into the device. – Previous coagulopathy, fibrinolysis, plt dysfxn. Mediastinitis and Sepsis (40-50%) – Device related. – Resistant organism. Malignant ventricular arrhythmia – LVAD flow↓ – Foster thrombus formation RV failure (20%) iNO Thromboembolism (20%)
 – Device related. – Resistant organism. Malignant ventricular arrhythmia – LVAD flow↓ – Foster thrombus formation RV failure (20%) iNO Thromboembolism (20%).")
48
Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) trial; N=280. The 1-year survival after LVAD implantation was 56%; in-hospital mortality after LVAD surgery was 27%. – The most important determinants: poor nutrition hematological abnormalities end-organ or right ventricular dysfunction lack of inotropic support Circulation. 2007 Jul 31;116(5):497-505. Epub 2007 Jul 16
: Epub 2007 Jul 16.")
49
Preoperative RV dysfunction correlated well with postoperative worsening RV dysfunction. – deviation of interventricular septum towards the LV, which eliminates the septal contribution to right heart contractility. Neragi-Miandoab et al. Journal of Cardiothoracic Surgery 2012, 7:60a

50
Operative mortality of 46% for a score > 5. 12% for a score to <=5. J Thorac Cardiovasc Surg 2003;125:855-62

51
Back to our patient and Questions Pre-LVAD status: – prolonged ECMO support end organ damage? – profound coagulopathy – PRA(+) Increase peri-operative mortality
 Increase peri-operative mortality.")
Similar presentations









 VAD (Ventricular assist device)>")
: Indications and Management Strategy David Spielvogel, MD Surgical Director, Cardiac Transplant and Mechanical.>")

 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")


>")









