Download presentation
Presentation is loading. Please wait.

1
Stenting Patients Needing Non-Cardiac Surgery
Davide Capodanno, MD University of Catania Cardiology Department Ferrarotto Hospital - Catania Director: Prof. C. Tamburino

2
Yes Step 1 No Yes Step 2 No Yes Step 3 No Yes Step 4 No or unknown
Perioperative surveillance and postoperative risk stratification and risk factor management Need for emergency noncardiac surgery? Yes Step 1 Operating room No Active cardiac conditions? Yes Evaluate and treat per ACC/AHA guidelines Step 2 Consider operating room No Low risk surgery Yes Step 3 Proceed with planned surgery No Functional capacity greater than or equal to 4 MET, without symptoms Yes Step 4 Proceed with planned surgery No or unknown Step5 Fleisher et al. ACC/AHA 2007

3
3 or more clinical risk factors Vascular surgery
Step 5 3 or more clinical risk factors Vascular surgery Intermediate risk surgery 1-2 clinical risk factors No clinical risk factors Proceed with planned surgery Consider testing if it will change management Proceed with planned surgery with HR control or consider non-invasive testing if it will change management Fleisher et al. ACC/AHA 2007 Perioperative Guidelines. JACC 2007;50:e

4
Prophylactic revascularization before non-cardiac surgery
Proponents of ‘prophylactic’ coronary revascularization in selected patients argue that it improves both perioperative as well as long-term outcome

5
But the debate is open Opponents of this approach point out that:
morbidity and mortality of PCI and CABG in high-risk elderly vascular patients are substantial and outweigh any benefit; recovery from such major morbidity substantially delays and even prevents the surgery for which the intervention was undertaken; it does not differentiate between young and old age and between patients with symptomatic CAD and those with CAD discovered by cardiac stress testing only; only survivors of coronary revascularization are included in the various reports

6
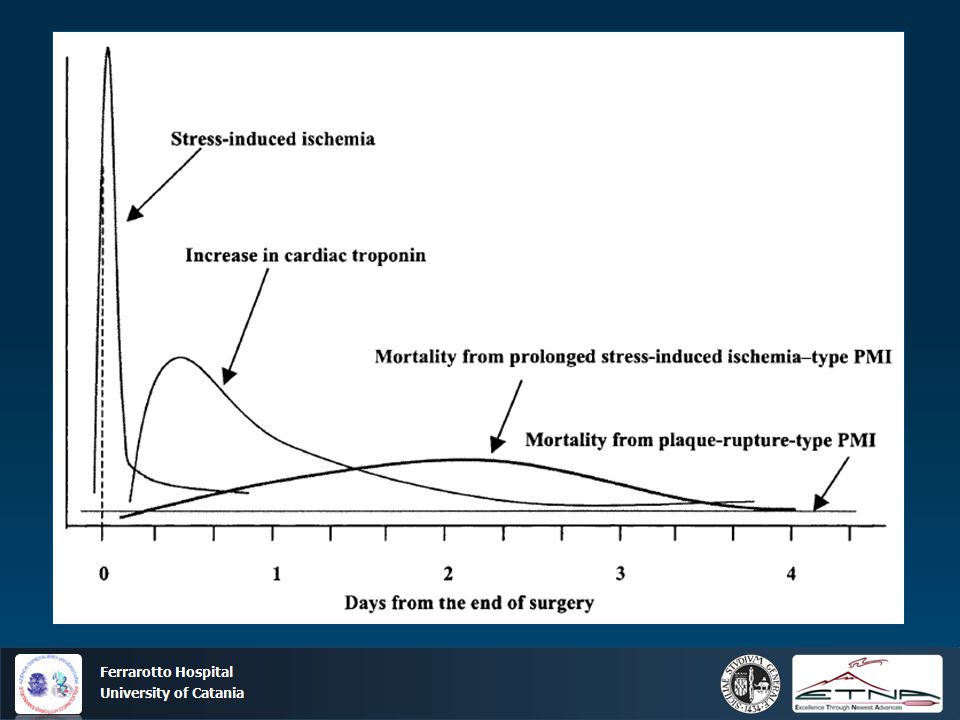
What do we know about perioperative myocardial ischemia (PMI)?
Perioperative myocardial ischemia peaks during the early postoperative period. Intraoperative ischemia is less common. PMI is preceded almost exclusively by ST depression-type ischemia. MI is mostly silent (50%) and most often is a non-Q wave rather than Q-wave infarction Mortality is <10% to 15%, similar to in-hospital mortality of nonsurgical non-Q infarction in contrast to earlier concerns, anesthesia per se, either general or regional, if administered without complications, is not a risk factor for the high-risk cardiac patient undergoing noncardiac surgery. Rather, it is postoperative stress (including emergence from anesthesia), which precipitates ischemia, infarction, and cardiac mortality.
 and most often is a non-Q wave rather than Q-wave infarction. Mortality is <10% to 15%, similar to in-hospital mortality of nonsurgical non-Q infarction. in contrast to earlier concerns, anesthesia per se, either general or regional, if administered without complications, is not a risk factor for the high-risk cardiac patient undergoing noncardiac surgery. Rather, it is postoperative stress (including emergence from anesthesia), which precipitates ischemia, infarction, and cardiac mortality.")
8
Two types of PMIs Preoperative revascularization of severe stenoses may not reduce perioperative ischemic complications

9
Cardiac Outcomes After Higher-Risk Noncardiac Surgery Stratified by Coronary Status in the CASS Registry (n=1546) * 30-Day Outcome No. of Diseased Vessels Medical Rx Prior CABG P Death 1 4/278 (1%) 4/191 (2%) NS 2 8/170 (5%) 2/314 (0.6%) 0.0005 3 7/134 (5%) 11/459 (2%) 0.15 MI 5/278 (2%) 3/191 (2%) 6/170 (3.5%) 0/314 (0%) 0.002 5/134 (4%) 5/459 (1%) 0.05 * Higher-risk noncardiac surgery indicates vascular, thoracic, major abdominal, and head and neck surgery Eagle KA et al, Circulation 1997
 4/191 (2%) NS. 2. 8/170 (5%) 2/314 (0.6%) /134 (5%) 11/459 (2%) MI. 5/278 (2%) 3/191 (2%) 6/170 (3.5%) 0/314 (0%) /134 (4%) 5/459 (1%) * Higher-risk noncardiac surgery indicates vascular, thoracic, major abdominal, and head and neck surgery. Eagle KA et al, Circulation")
10
Lessons from CASS Registry
Patients who had CABG within the previous 5 years can be sent for surgery, if their clinical condition has remained unchanged since their last examination. Patients undergoing low-risk procedures are unlikely to derive benefit from CABG before low-risk surgery, differently from those with multivessel disease and severe angina undergoing high-risk surgery This analysis represents a unique opportunity to examine surgery-specific risk in patients with well-defined coronary artery disease. We have shown that vascular, thoracic, abdominal, and major head and neck surgery are those specific procedures associated with a higher risk of a myocardial infarction or death in the face of nonrevascularized coronary artery disease. Furthermore, any benefit conferred by coronary revascularization appears to be particularly suited for this higher-risk subcategory of noncardiac procedures

11
Balancing the potential risks versus benefits of CABG before vascular surgery
Short term risk of CABG Perioperative risk of non-cardiac surgery Long-term benefit of CABG

12
Long-Term Survival among Patients Randomized to Undergo Coronary-Artery Revascularization or No Coronary-Artery Revascularization before Elective Major Vascular Surgery CARP trial McFalss et al, NEJM 2004

13
CARP post hoc analysis of patients undergoing vascular surgery after revascularization (n = 222)
")
14
Incidence of perioperative myocardial infarction and death
CARP post hoc analysis of patients undergoing vascular surgery after revascularization (n = 222) Incidence of perioperative myocardial infarction and death Ward et al, Ann Thorac Surg 2006
 Incidence of perioperative myocardial infarction and death. Ward et al, Ann Thorac Surg")
15
Incidence of All-Cause Death or Myocardial Infarction During 1-Year Follow-Up According to the Allocated Strategy in Patients With 3 or More Cardiac Risk Factors With Extensive Stress-Induced Ischemia DECREASE V OMT + Revasc OMT Randomized studies are not sized. Patients undergoing elective noncardiac procedures who are found to have prognostic high-risk coronary anatomy and in whom long-term outcome would likely be improved by coronary bypass grafting should generally undergo coronary revascularization before a noncardiac elective vascular surgical procedure or noncardiac operative procedures of intermediate or high risk p = 0.30 p = 0.48

16
When stents meet non-cardiac surgery
The cardiologist’s perspective The surgeon’s perspective Stents in patients needing non-cardiac surgery Prophylactic PCI: who? To stent or not to stent? Which stent, if any? Non-cardiac surgery in patients with stent How to manage antiplatelet therapy?

17
Prophylactic PCI Unstable active CAD (UA/NSTEMI, STEMI)
according to current guidelines: Yes Recurrent ischemia after CABG: Yes Asymptomatic ischemia or CCS I-II: No Stable angina but CCS III: Uncertain, probably not Left main: poor outcome with PCI, consider CABG In summary: PCI is of no value in preventing perioperative cardiac eventsm except in those patients in whom PCI is independently indicated for an acute coronary syndrome Fleisher et al, JACC 2007

18
Balloon angioplasty BARI post hoc analysis

19
Issues with balloon PTCA
Delaying noncardiac surgery for more than 8 weeks increases the chance of restenosis. Performing the surgical procedure too soon after the PCI procedure might also be hazardous. Delaying surgery for at least 2 to 4 weeks after balloon angioplasty to allow for healing of the vessel injury at the balloon treatment site is the optimal approach Daily aspirin antiplatelet therapy should be continued perioperatively. The risk of stopping the aspirin should be weighed against the benefit of reduction in bleeding complications from the planned surgery. Arterial recoil or acute thrombosis at the site of balloon angioplasty is most likely to occur within hours to days after balloon coronary angioplasty.

20
What about stenting? Ka GL et al, JACC 2000

21
No apparent ambiguities from guidelines
It is recommended that patients with previous CABG in the last 5 years be sent for non-cardiac surgery without further delay (class I C) It is recommended that non-cardiac surgery be performed in patients with recent bare metal stent implantation after a minimum 6 weeks and optimally 3 months following the intervention (class I B) It is recommended that non-cardiac surgery be performed in patients with recent drug-eluting stent implantation no sooner than 12 months following the intervention (class I B) Consideration should be given to postponing non-cardiac surgery in patients with recent balloon angioplasty until at least 2 weeks following the intervention (class IIa B) ESC guidelines 2009
 It is recommended that non-cardiac surgery be performed in patients with recent bare metal stent implantation after a minimum 6 weeks and optimally 3 months following the intervention (class I B) It is recommended that non-cardiac surgery be performed in. patients with recent drug-eluting stent implantation no. sooner than 12 months following the intervention (class I B) Consideration should be given to postponing non-cardiac. surgery in patients with recent balloon angioplasty until at. least 2 weeks following the intervention (class IIa B) ESC guidelines")
22
ESC guidelines 2009

23
Unplanned surgery The need for surgery in relation to its timing and the specific pathology (e.g. malignant tumour, vascular aneurysm repair) should be balanced against the excessive risk of stent thrombosis during the first year following DES implantation and a careful ‘case-by-case’ consideration is advisable. Discussion between the surgeon, the anaesthesiologist, and the treating cardiologist about this matter is recommended in order to achieve a reasonable expert consensus
 should be balanced against the excessive risk of stent thrombosis during the first year following DES implantation and a careful ‘case-by-case’ consideration is advisable. Discussion between the surgeon, the anaesthesiologist, and the treating cardiologist about this matter is recommended in order to achieve a reasonable expert consensus.")
24
Conclusions Successful perioperative evaluation and management of high- risk cardiac patients undergoing noncardiac surgery requires careful teamwork and communication between surgeon, anesthesiologist, the patient’s primary caregiver, and the consultant. The use of both noninvasive and invasive preoperative testing should be limited to those circumstances in which the results of such tests will clearly affect patient management For many patients noncardiac surgery represents their first opportunity to receive an appropriate assessment of both short- and long-term cardiac risk.

Similar presentations









>")






>")


