Download presentation
Presentation is loading. Please wait.

1
Dr Narinder Pal Singh Dr Minati Choudhary
Cardioplegia Dr Narinder Pal Singh Dr Minati Choudhary

2
Cardioplegic Strategies
sufficient reduction of oxygen demands delivery to all cardiac regions provide unimpaired vision

3
Advantages Immediate arrest Hypothermia Provide substrate Maintain pH
Avoid reperfusion damage Avoid edema

4
Cardioplegic solutions
1 Electrolyte composition Intracellular no/ low conc. of sodium and calcium Extracell. Na depletion, loss of memb. Pot. Extracellular higher conc. of sodium, calcium, Mg hyperkalemic depol. of cell memb.

5
Calcium 2 pH 3 Osmolality Calcium paradox
solutions devoid of ca2+ should never be used 2 pH Ischemia-intracellular pH ↓ as lactate accumulates. Buffers should be added. 3 Osmolality Important in limiting myocardial edema Blood- Iso-osmolar Crystalloid- hypo/ iso / hyper (albumin, mannitol, glucose)
")
6
Additives KCl Diastolic arrest THAM/Histidine Buffer Mannitol
Osmolality/Free Radical Scavenger Aspartate/Glutamate Substrate MgCl2 Ca2+ antagonist CPD ↓ free Ca2+ conc Glucose Blood O2 carrying

7
Types of Cardioplegia crystalloid blood (2:1, 4:1, 8:1, blood only)
")
8
Crystalloid Cardioplegia
Does not contain hemoglobin Delivers dissolved oxygen only Can be used only with myocardial hypothermia

9
Intracellular

10
Extra cellular

11
BLOOD CARDIOPLEGIA oxygenated environment.
intermittent reoxy of the heart during arrest. limit hemodilution when large vol of CP used. excellent buffering capacity. osmotic properties. electrolyte composition and pH are physiologic.

12
endogenous antioxidants and free radical scavengers.
Provides substrate less complex than other solutions to prepare. Various forms- warm, cold, hot shot Better ATP replenish Lower periop morbidity & mortality

14
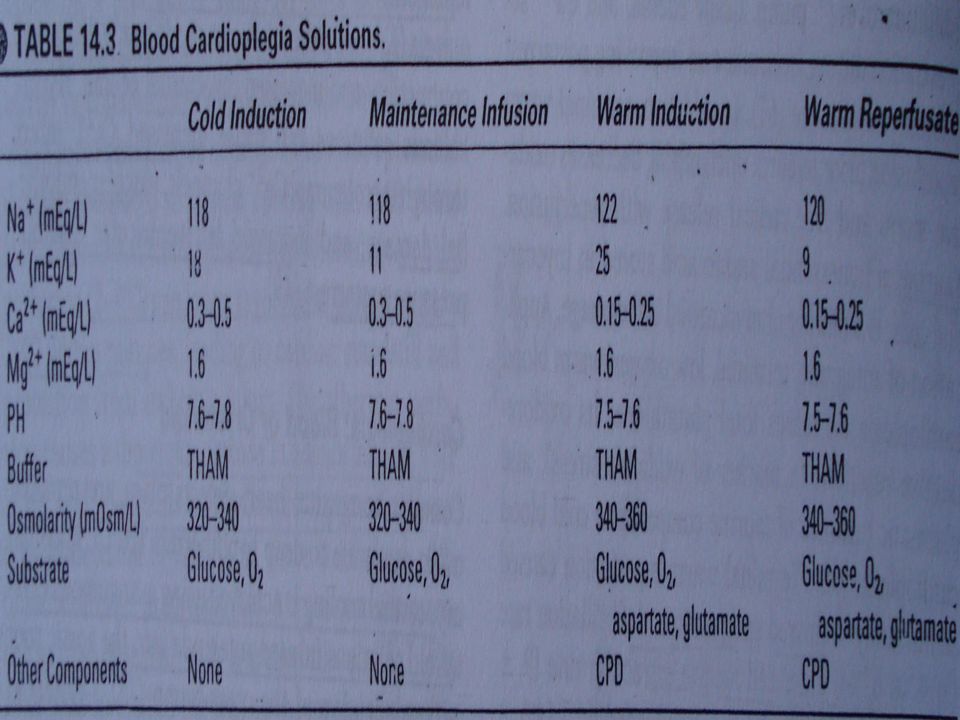
Cold Blood Cardioplegia
Advantages Lowers myocardial oxygen demands Pitfalls Hypothermic inhibition of mitochondrial enzymes Shifts oxyhaemoglobin dissociation curve to left Activates platelets, leukocytes, complement Impaired membrane stabilization

15
Warm Induction (resuscitation of the heart)
severe left ventricular dysfunction cardiogenic shock preischaemic depletion of energy stores warm induction showed improved aerobic metabolism and LV function

16
Warm Reperfusion (hot-shot)
early myocardial metabolic recovery while maintaining electro-mechanical arrest repletion of energy stores

17
Continuous Warm Cardioplegia
avoidance of direct myocellular injury inflicted by any cold solution or environment increased rate of perioperative stroke and neurological events (randomised trial-1001 patients)
")
18
“The heart takes up oxygen over time rather than by dose, so that blood cardioplegic solutions must be delivered over a time interval, rather than by volume” Buckberg GD J Thorac Cardiovasc Surg 1991;102:

19
Cardioplegic Temperature
cold (9 0C) tepid (29 0C) warm (37 0C) Hayashida et al- compared cold (8°C), tepid (29°C), or warm (37°C) in 72 pts of CABG. tepid CP- most effective in reducing anaerobic lactate acid release during the arrest period. Whether tepid cardioplegia confers better protection over other current methodologies remains to be determined
 tepid (29 0C) warm (37 0C) Hayashida et al- compared cold (8°C), tepid (29°C), or warm (37°C) in 72 pts of CABG. tepid CP- most effective in reducing anaerobic lactate acid release during the arrest period. Whether tepid cardioplegia confers better protection over other current methodologies remains to be determined.")
20
retrograde (coronary sinus) Combined (ante/retro)
Cardioplegic Route antegrade (aorta) retrograde (coronary sinus) Combined (ante/retro)
 retrograde (coronary sinus) Combined (ante/retro)")
21
Antegrade Cardioplegia
Initial flow rate 150ml/min/m2 Initial dose ml/kg (upto 1 litre) Perfusion pressure mm Hg
 Perfusion pressure mm Hg.")
22
Antegrade Cardioplegia
Advantages Produces prompt arrest Pitfalls poor distribution in coronary patients poor distribution in patients with AR risk of ostial injury from direct perfusion interruption of procedure during mitral surgery

23
Retrograde Cardioplegia
Correct catheter placement flow rate = 200mL/min perfusion pressure < 40 mmHg prevent perivascular haemorrhage and oedema

24
Retrograde Cardioplegia
Advantages Distribution of CP to regions supplied by occluded/stenosed vessels Improved subendocardial CP delivery Flushing of air and/or atheromatous debris Pitfalls Shunting of CP into ventricular cavities via Thebesian channels Perfusion defects especially right ventricle and posterior septal regions

25
Combined (ante/retro)
Studies have demonstrated better myocardial protection Various techniques Arrest with antegrade, additional doses given retrogradely with venting of aortic root Alternating technique-retrograde cardioplegia administered frequently+ interrupted antegrade cardioplegia down each completed graft Simultaneous method- retrograde continued while antegrade is given down each graft.

28
inadequate protection postop RV dysfn coronary ostial stenosis
COMPLICATIONS inadequate protection postop RV dysfn coronary ostial stenosis coronary sinus injury aortic root injury

29
CONTROVERSY ‘ideal’ cardioplegic technique different crystalloid cardioplegia crystalloid versus blood cardioplegia Although recent rand trials - improved metabolic and functional myo preserv with blood CP -decreased mortality and morbidity not consistently demonstrated between blood and crystalloid cardioplegia.

30
Therefore, institutional and the individual surgeon's experience remain the most important determinants of myocardial protection strategy at this moment.

31
Thank you

Similar presentations