Download presentation
Presentation is loading. Please wait.

1
rFactor VIIa in Cardiac Surgery
Timothy H. Trotter, MD, FACS Assistant Professor of Surgery

2
IRB Approval OUHSC IRB Protocol #12376 VAMC IRB Protocol #12376

3
Assistance Mary Lane, PhD -- Data analysis
Shannie Frisbie -- Cost information The residents and fellows for providing me with the opportunity to use rFVIIa

4
FDA Approved Uses for rFactor VIIa
“…management of bleeding related to hemophilia in patients with factor inhibitors…” A number of “off label” uses have become popular since it was first used for treatment of traumatic bleeding after a GSW in 1999

5
Clotting Factor Changes in CPB
Davidson, et al. Blood Coagulation & Fibrinolysis 2003; 14: Clotting Factor Changes in CPB Decrease in Factors may be important in CPB Harker -- decrease in Factors not important Based on observations of single deficiency pts The following changes have been observed : Factor II 51% Decrease Factor V 28% Decrease Falls before CPB Less fall with adequate heparinization Factor VII 27% Decrease Ca. 28% fall in the PCV due to dilution Factor X 56% Decrease Factor VIII No Change

6
rFactor VIIa Mechanism of Action
406 amino acid Vitamin K-dependent glycoprotein Generation of thrombin by initial binding to tissue factor and activation of FX on the platelet surface It also participates in conversion FIX-->FIXa Activation of FX in combination with FV converts prothrombin to thrombin leading to the formation of a hemostatic “plug” & subsequently converts fibrinogen to fibrin causing local hemostasis

7
rFactor VIIa Mechanism of Action
Partial activation of thrombin occurs at rFVIIa concentrations of 50nM, but full activation of thrombin or “thrombin burst” occurs at nM This thrombin activity on the platelet leads to a stabilized thrombin plug and tight fibrin structure resistant to lysis

8
rFactor VIIa Mechanism of Action
The “thrombin burst” and stabilized “plug” seems to only occur at sites where tissue factor is exposed at sites of vessel injury This is probably why there is little generalized thrombosis with rFVIIa

9
rFactor VIIa Mechanism of Action
The decrease in fibrinolysis is thought to possibly be due to an increase in thrombin-activatable fibrinolysis inhibitor and an increase in FXIIIa rFVIIa appears to work in a TF-independent fashion directly on FIX/FX on the phospholipid surface of the activated platelet

10
Hemostatic Mechanisms for rFVIIa
Eikelboom, et al. Blood Coagulation & Fibrinolysis 2003, 14: Hemostatic Mechanisms for rFVIIa

11
rFactor VIIa Half Life The mean elimination half life of rFVIIa is hours (only 1.3 hours in children) Prothrombin time is shortened by rFVIIa treatment

12
rFactor VIIa Dosing Dosage Micrograms/Kg Time to Treatment
Excellent or Effective Response % Mean Number of Doses Compassionate Use 60-120 5 days 72 13.6 Dose Finding 70 9 hours 3.6 35 53 3.5 US Home Treatment 90 1.2 hours 92 2.3

13
rFactor VIIa Dosing Most authors will admit that there is little real science for the dosing of rFVIIa and most authorities recommend that the dosing be based on weight, but that the dose be rounded to the nearest vial Continuous infusions do not seem to provide any benefit and the dosing scheme is no more clear than bolus

14
Adverse Effects of rFVIIa
Novo Nordisk data, rFVIIa, 20 March 2001. Adverse Effects of rFVIIa As of March 2001, an estimated 171,790 doses had been sold with 87 reported adverse events: 16 Decreased therapuetic response 7 MI’s (all pt’s had predisposing factors) 4 PE’s 6 Ischemic CVA’s 3 Venous Thromboses 1 DIC 17 died and 8 were felt to be related to the rFVIIa 1:21,474 related to rFVIIa
 4 PE’s. 6 Ischemic CVA’s. 3 Venous Thromboses. 1 DIC. 17 died and 8 were felt to be related to the rFVIIa. 1:21,474 related to rFVIIa.")
15
Adverse Effects of rFVIIa
Levi, et al. Crit Care Med 2005; 33: Adverse Effects of rFVIIa Levi et al reviewed 483 papers related to the pharmacologic use of rFVIIa Used for hemophilia with inhibiting antibodies, Glanzmann Thrombasthenia, congenital FVII deficiency, liver disease, cirrhosis, surgery/trauma, reversal of anticoagulant therapy, and excessive blood loss They found that in patients other than hemophilia patients the estimated incidence of thromboembolism is 1.4%

16
Surgical Uses of rFVIIa
Raobaikady, et al. BJA 94(5): Surgical Uses of rFVIIa Raobaikady et al looked at the use of rFVIIa in a double-blind, randomized, placebo-controlled study in 48 patients undergoing surgery for major traumatic fracture of the pelvis or the pelvis/acetabulum and found no decrease in the volume of blood loss in patients with normal hemostasis
: Surgical Uses of rFVIIa. Raobaikady et al looked at the use of rFVIIa in a double-blind, randomized, placebo-controlled study in 48 patients undergoing surgery for major traumatic fracture of the pelvis or the pelvis/acetabulum and found no decrease in the volume of blood loss in patients with normal hemostasis.")
17
Cardiac Surgery and rFVIIa
Karkouti, et al. Transfusion 2005; 45:26-34. Cardiac Surgery and rFVIIa Karkouti et al looked at 51 patients with intractable blood loss after cardiac surgery using a propensity score-matched case-control analysis They used about 70micrograms/kg in severe bleeding and 35micrograms/kg in “less severe, controlled bleeding”

18
Characteristics of Karkouti Pts
Karkouti, et al. Transfusion 2005; 45:26-34. Characteristics of Karkouti Pts VARIABLE rFVIIa PATIENTS % GENERAL POP % p VALUE Mean Age 56 62 0.0007 Urgent Surgery 27 8 <0.0001 Redo Surgery 35 CHF 48 21 Active Endocarditis 1 Complex Surgery 73 24 Mean CPB Period (min) 159 100 DHCA 15 3 Difficult Wean from CPB 46 13 LCOS 25 4 Reexploration 60 6 Massive Blood Loss 92 Units Blood, Cryoppt 10 PRBC 14 Platelets FFP
 DHCA Difficult Wean from CPB LCOS Reexploration Massive Blood Loss. 92. Units Blood, Cryoppt. 10. PRBC. 14. Platelets. FFP.")
19
Karkouti, et al. Transfusion 2005; 45:26-34.
Matched Control Pts The matched control patients were essentially no different from the rFVIIa patients except in the volume of blood products that they received

20
Postoperative Course Karkouti Pts
Karkouti, et al. Transfusion 2005; 45:26-34. Postoperative Course Karkouti Pts ADVERSE EVENT GENERAL POP rFVIIa PATIENTS MATCHED CONT PT Recovery Measures Duration Intub (hrs) 14 62 64 ICU LOS (days) 1 6 3.5 (p <0.05) Hosp LOS (days) 7 15.5 10 (p <0.05) Adverse Event CVA 1.4 4 MI 2.2 3 PE/DVT 0.2 Liver Dysfunction N/A 2 Renal Dysfunction 15 6 (p <0.05) Death 0.4 Composite 21
 ICU LOS (days) (p <0.05) Hosp LOS (days) (p <0.05) Adverse Event. CVA MI PE/DVT Liver Dysfunction. N/A. 2. Renal Dysfunction (p <0.05) Death Composite. 21.")
21
Karkouti, et al. Transfusion 2005; 45:26-34.
Karkouti Conclusions The hourly blood loss profile after the administration of rFVIIa is similar to that seen in the control and is significant 1/3 of the patients required a second dose and all of those patients had a surgically correctable cause rFVIIa was found to reduce intractable blood loss, but with an increase in morbidity ICU LOS, Hosp LOS, Renal Dysfunction, ? CVA

22
Cardiac Surgery and rFVIIa
Ravio et al, Ann Thorac Surg 2005; 80:66-71. Cardiac Surgery and rFVIIa Raivio et al reported the use of rFVIIa in 16 postop cardiac surgery patients 10 patients were “emergency” 6 patients required DHCA 4 were redo patients All were complex cardiac or aortic procedures Mean predicted EuroSCORE mortality was 19.8% Hospital mortality was 25% Mean ICU stay was 21 days Mean dose was 65 micrograms/kg

23
Raivio Bleeding Pre/Post rFVIIa
Ravio et al, Ann Thorac Surg 2005; 80:66-71. Raivio Bleeding Pre/Post rFVIIa 6 Hours Before rFVIIa 6 Hours After rFVIIa p Value Bleeding (ml) 2180 350 <0.001 Transfusions (Units) Platelets 12 0.005 FFP 3.0 1.0 0.017 PRBC 4.0 2.0 NS
 < Transfusions (Units) Platelets FFP PRBC NS.")
24
Ravio et al, Ann Thorac Surg 2005; 80:66-71.
Raivio Conclusions 82% of the patients had an obvious hemostatic response 25% had “severe postoperative thromboembolic or thrombotic complications” All of the Heart or Heart/Lung transplant patients died They recommend caution in the use of rFVIIa

25
Cost Concerns The cost of rFVIIa is significant
1.2 mg, 2.4mg, and 4.8 mg vials 2.4 mg “costs” $850 at VAMC 2.4 mg “costs” $2184 at OUMC Estimated cost in literature is about $5000 for a 90 mcg/kg dose in a 70kg patient Cost to OUMC 8/04-8/05 for 46 doses in 35 patients was $299,240 However, the cost of intractable bleeding is also high Average incremental increase in cost of $3,866 Bleeding requiring reexploration increases mortality 7-fold (15.4%) and the additional cost is $10,000
 and the additional cost is $10,000.")
26
Oklahoma City VAMC and rFVIIa
rFVIIa was first used at the OKC VAMC for intractable post-Cardiotomy bleeding in December 2002 Since that time 16/564 patients have received rFVIIa

27
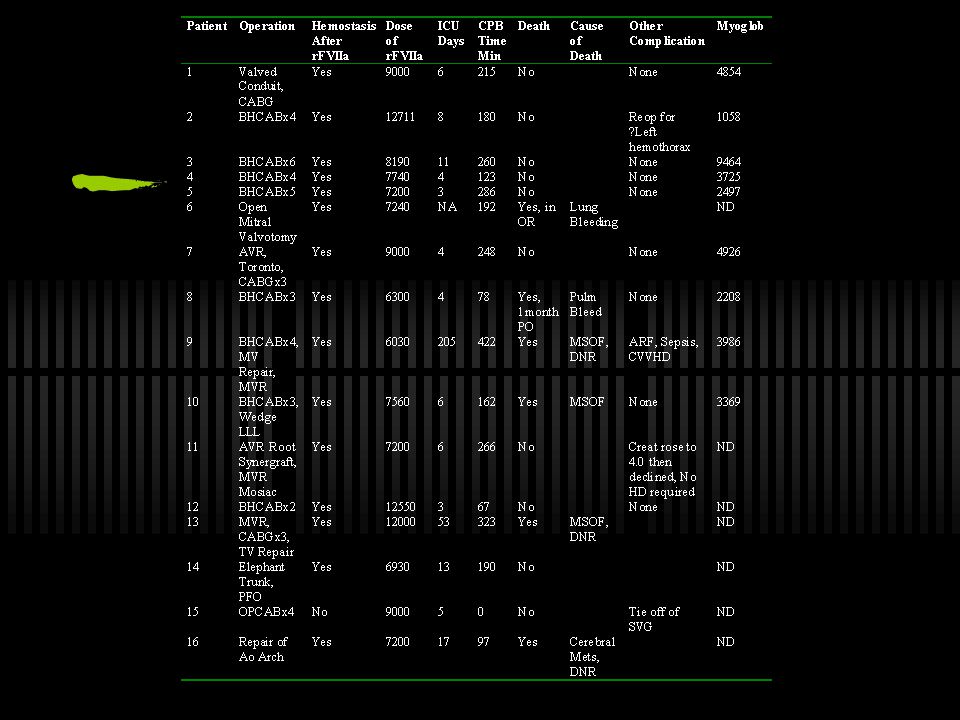
Demographics 16 patients Mean Age 63.9 yrs (54-76) Elective 37.5%
Urgent % Emergency % Amicar % Aprotinin 75% Nothing % Few of these patients were receiving IIb/IIIa inhibitors/Plavix

28
Patient Characteristics
Mean Preop EF 49% Mean rFVII Dose mcg/kg Mean NYHA/CCS /2.94 Mean CPB Time min One OPCAB Patient Mean Operative Time 413 min Mean Intubation Time 53 hours Mean SICU Days days Mean Hospitalization Days days

31
Total Blood Product Use

32
Blood Usage in Pts With rFVIIa Postop

33
Cell Saver Use Pre/Post-FVII

34
PRBC Use Pre/Post-FVII

35
Platelet Use Pre/Post-FVII

36
FFP Use Pre/Post-FVII

37
Cryoppt Use Pre/Post-FVII

38
Chest Tube Output/Hr

39
Outcomes 2/16 patients were returned to the OR for re-exploration
One was bleeding from a side branch of a SVG One had stopped bleeding and had only about ml of blood total in the left chest and mediastinum This represents all of the patients returned (with or without rFVIIa) for the past 4 years
 for the past 4 years.")
40
Mortality 6/16 patients died
1/16 (6.25%) died in the OR/within 30 days 5/16 died from 36 to 208 days later 31.25% overall mortality for these patients Overall mortality 4.1% (23/564) from 12/02-7/05 5/16 of these deaths were attributed as Operative Mortality by CICSP and these are included in the 4.1%
 died in the OR/within 30 days. 5/16 died from 36 to 208 days later % overall mortality for these patients. Overall mortality 4.1% (23/564) from 12/02-7/05. 5/16 of these deaths were attributed as Operative Mortality by CICSP and these are included in the 4.1%")
41
Time To Death

42
Future Directions rFVIIa, while expensive, may be less expensive than re-exploration rFVIIa may salvage some patients who otherwise would not have survived Is there a role for rFVIIa earlier in the care of these patients?

43
Other Issues Other Off-label uses for rFVIIa
Relative contraindications to transfusion Multiple RBC allo-antibodies Refractoriness to platelet transfusions ?? Plavix poisoning IgA deficiency who should not get FFP Jehovah’s Witnesses When is the best time to give rFVIIa? Who decides who gets and when to give rFVIIa?

Similar presentations




>")









 and recombinant Factor VIIa Mechanism of Action Jerrold H. Levy, MD Emory University School of Medicine and Emory Healthcare Atlanta,>")



 Regionaal.>")

