Download presentation
Presentation is loading. Please wait.

1
Prepared by David S. Anderson, Ph.D. Professor of Education and Human Development George Mason University Fairfax, Virginia 703-993-3698 danderso@gmu.edu caph.gmu.edu

2
General Usage Patterns Student-Athletes

3
TRADITIONAL-AGE COLLEGE STUDENTS: ALCOHOL USE IN LAST 30 DAYS http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

4
TRADITIONAL-AGE COLLEGE STUDENTS: DRUNK IN LAST 30 DAYS http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

5
TRADITIONAL-AGE COLLEGE STUDENTS: 5 OR MORE DRINKS IN LAST TWO WEEKS http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

6
USE OF ALCOHOL BY TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE and HEAVY DRINKING http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

7
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF MARIJUANA http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

8
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF ECSTASY http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

9
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF NARCOTICS OTHER THAN HEROIN http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

10
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF COCAINE http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

11
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF INHALANTS http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

12
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF LSD http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

13
TRADITIONAL-AGE COLLEGE STUDENTS: 30 DAY USE OF AMPHETAMINES http://monitoringthefuture.org/pubs/monographs/vol2_2009.pdf

14
Source: Core Institute http://www.siu.edu/departments/coreinst/public_html/

15
AthleteNon-Athlete Regretted behavior46.4%37.2% Missed a class39.4%31.6% Blackout36.0%27.6% Had unplanned sexual activity 31.0%22.7% 5 or more neg. consequences 29.5%20.1% Harvard College Alcohol Study, 2001

16
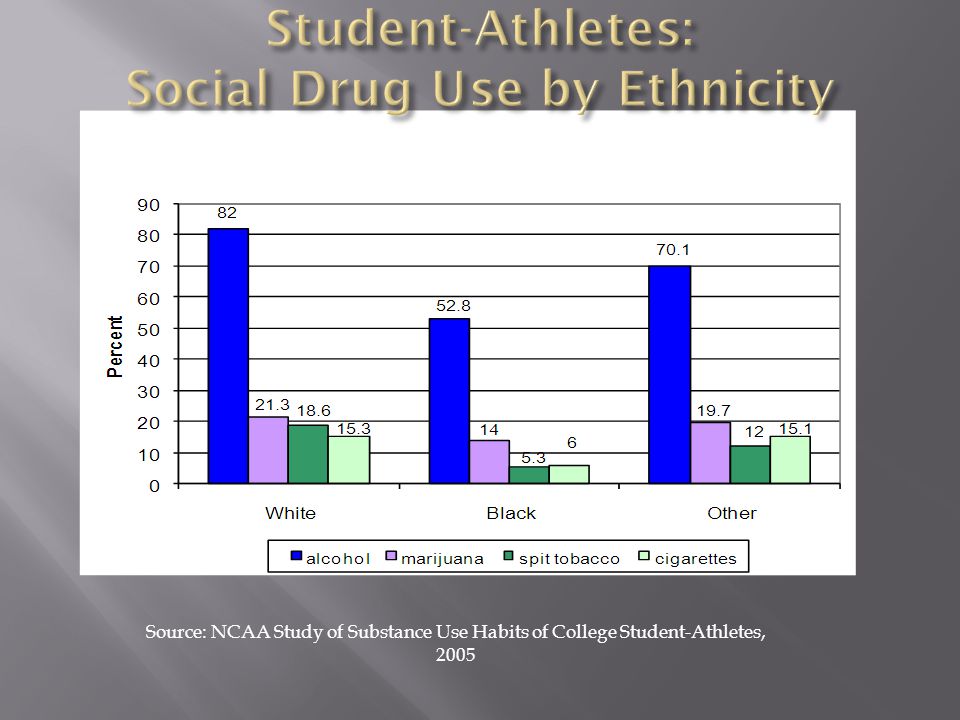
82.6%Recreational or social purposes 13.6%Because it makes me feel good 3.3%Helps me deal with the stresses of college life and college athletics 0.0%Improves my athletic performance Source: NCAA Study of Substance Use Habits of College Student-Athletes, 2005

23
AthleteNonathlete Driving 90.9%91.7% Studying 78.4%74.5% Interferes with athletics 61.2%18.3% On a date 46.4%40.8% Fattening 30.2%26.3% Afraid of getting caught 22.7%18.5% Source: Harvard College Alcohol Study, 2001

24
Approximately 83 percent of the respondents indicated drinking alcohol within the last 12 months. Over half the respondents indicated their first experience with alcohol was between the ages of 14 – 17. The majority of those reporting alcohol usage report frequency of use as less than two days per week. Forty percent of those reporting alcohol usage report drinking six to 10 plus drinks in one sitting. One third of the respondents indicated drinking only during their off season. The majority of the respondents indicated obtaining alcohol from a friend, family member or teammate.

25
Approximately 23.6 percent of the respondents indicated use of marijuana within the last 12 months. For the majority of those reporting marijuana use, the reported age of the first experience with marijuana was between the ages of 16 – 20. Over half of those reporting marijuana usage report frequency of use as less than once per month. The majority of the respondents using marijuana indicated use only during their off season. The majority of the respondents using marijuana indicated obtaining the substance from a friend, family member or teammate.

26
General Usage Patterns

27
"Although statistics on drug use in the United States are not fully reliable, the numbers available indicate that US consumption of cocaine and marijuana has been essentially stable for many years— although considerably reduced from its peak in the 1970s and 1980s. The data also show that, today, the United States consumes illegal substances at a rate some three times that of Europe—although the use of drugs in the EU continues to grow rapidly and a few countries actually consume more per capita than the United States. In both the United States and Europe, the wholesale and street prices of cannabis and cocaine have declined in the past several years, although reportedly their potency has increased and demand remains steady. Across the world, illicit drugs appear to be available at stable or declining prices. A recent EU Commission study concluded that global drug production and use remained largely unchanged during the period from 1998 through 2007.“ Source: Hakim, Peter, "Rethinking US Drug Policy," Inter-American Dialogue (Washington, DC: The Beckley Foundation, February, 2010), p. 4. http://www.thedialogue.org/uploads/Documents_and_PDFs/Documents_and_PDFs... http://www.thedialogue.org/uploads/Documents_and_PDFs/Documents_and_PDFs...
, p")
28
Percentage Change in Lifetime and Monthly Substance Use (ages 12 and older) Percent Change Lifetime Eight- Year %chg 2002-2009 Lifetime Five-Year %chg 2002-2006 Monthly Eight-Year %chg 2002-2009 Monthly Five-Year %chg 2002-2006 ILLICIT DRUGS - ALL+9.7%+3.3%+11.7%+4.3% Marijuana+10.0%+3.0%+14.6%+1.6% Cocaine+7.9%+4.1%-19.0%+19.9% Crack-0.5%+1.8%-13.2%+23.8% Heroin+0.4%+3.2%+17.5%+103.6% Hallucinogens+8.6%+2.8%+5.2%-15.9% Ecstasy+40.2%+20.8%+12.4%-21.9% Psychotherapeutics+8.0%+6.3%+10.6%+12.9% Pain Relievers+18.4%+13.0%+20.1%+19.3% Methamphetamine-16.5%-7.5%-26.5%+7.0% Illicit-other-than- marijuana +7.8%+3.7%+4.3%+9.5% Alcohol+6.7%+4.1%+9.0%+4.6% Alcohol – Heavy-- +8.0%+6.8% Tobacco+1.3%+1.2%-2.5%+1.9%
 Percent Change Lifetime Eight- Year %chg Lifetime Five-Year %chg Monthly Eight-Year %chg Monthly Five-Year %chg ILLICIT DRUGS - ALL+9.7%+3.3%+11.7%+4.3% Marijuana+10.0%+3.0%+14.6%+1.6% Cocaine+7.9%+4.1%-19.0%+19.9% Crack-0.5%+1.8%-13.2%+23.8% Heroin+0.4%+3.2%+17.5%+103.6% Hallucinogens+8.6%+2.8%+5.2%-15.9% Ecstasy+40.2%+20.8%+12.4%-21.9% Psychotherapeutics+8.0%+6.3%+10.6%+12.9% Pain Relievers+18.4%+13.0%+20.1%+19.3% Methamphetamine-16.5%-7.5%-26.5%+7.0% Illicit-other-than- marijuana +7.8%+3.7%+4.3%+9.5% Alcohol+6.7%+4.1%+9.0%+4.6% Alcohol – Heavy %+6.8% Tobacco+1.3%+1.2%-2.5%+1.9%")
29
Percentage Change in Monthly Substance Use (ages 12 and older) Percent Change Monthly Eight-Year %chg 2002-2009 Monthly Five-Year %chg 2002- 2006 ILLICIT DRUGS - ALL +11.7%+4.3% Marijuana +14.6%+1.6% Cocaine -19.0%+19.9% Crack -13.2%+23.8% Heroin +17.5%+103.6% Hallucinogens +5.2%-15.9% Ecstasy +12.4%-21.9% Psychotherapeutics +10.6%+12.9% Pain Relievers +20.1%+19.3% Methamphetamine -26.5%+7.0% Illicit-other-than-marijuana +4.3%+9.5% Alcohol +9.0%+4.6% Alcohol – Heavy +8.0%+6.8% Tobacco -2.5%+1.9% http://www.drugwarfacts.org/cms/Drug_Usage#Change
 Percent Change Monthly Eight-Year %chg Monthly Five-Year %chg ILLICIT DRUGS - ALL +11.7%+4.3% Marijuana +14.6%+1.6% Cocaine -19.0%+19.9% Crack -13.2%+23.8% Heroin +17.5%+103.6% Hallucinogens +5.2%-15.9% Ecstasy +12.4%-21.9% Psychotherapeutics +10.6%+12.9% Pain Relievers +20.1%+19.3% Methamphetamine -26.5%+7.0% Illicit-other-than-marijuana +4.3%+9.5% Alcohol +9.0%+4.6% Alcohol – Heavy +8.0%+6.8% Tobacco -2.5%+1.9%")
30
Treatment Episode Data Set - Admissions (TEDS-A), 2008 http://www.icpsr.umich.edu/quicktables/quickoptions.do
,")
31
Treatment Episode Data Set - Admissions (TEDS-A), 2008 http://www.icpsr.umich.edu/quicktables/quickoptions.do
,")
32
Patterns Linked to Start of Use Use Linked to Homework Checked by Parents Use Linked to Involvement in Activities

33
A number of information sources are used to quantify America’s drug problem and to monitor drug abuse trends. Foremost among these sources are the Monitoring the Future (MTF) survey* and the National Survey on Drug Use and Health** (NSDUH). Since 1975, the MTF survey has measured drug, alcohol, and cigarette use as well as related attitudes among adolescent students nationwide. For the 2010 survey, 46,482 students in 8th, 10th, and 12th grades from 396 public and private schools participated. Funded by NIDA, the MTF survey is conducted by investigators at the University of Michigan. The NSDUH is an annual survey on the nationwide prevalence and incidence of illicit drug, alcohol, and tobacco use, abuse, and dependence among Americans aged 12 years and older, conducted by the Substance Abuse and Mental Health Services Administration. Approximately 67,500 people are included in this survey. Because of differences in the timing of administration of the surveys, reported NSDUH data are 1 year behind those of MTF. In MTF and NSDUH, there are three primary prevalence periods for which data are reported: lifetime, past year, and past month (also referred to as “current”). It is generally believed that past year and past month are the better indicators of actual use. However, some analyses are done for only one specific prevalence period. http://www.nida.nih.gov/infofacts/nationtrends.html
 survey* and the National Survey on Drug Use and Health** (NSDUH). Since 1975, the MTF survey has measured drug, alcohol, and cigarette use as well as related attitudes among adolescent students nationwide. For the 2010 survey, 46,482 students in 8th, 10th, and 12th grades from 396 public and private schools participated. Funded by NIDA, the MTF survey is conducted by investigators at the University of Michigan. The NSDUH is an annual survey on the nationwide prevalence and incidence of illicit drug, alcohol, and tobacco use, abuse, and dependence among Americans aged 12 years and older, conducted by the Substance Abuse and Mental Health Services Administration. Approximately 67,500 people are included in this survey. Because of differences in the timing of administration of the surveys, reported NSDUH data are 1 year behind those of MTF. In MTF and NSDUH, there are three primary prevalence periods for which data are reported: lifetime, past year, and past month (also referred to as current ). It is generally believed that past year and past month are the better indicators of actual use. However, some analyses are done for only one specific prevalence period.")
34
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

35
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

36
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

37
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

38
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

39
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

40
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

41
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

42
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

43
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

44
National Survey on Drug Use and Health, 2009 http://www.icpsr.umich.edu/icpsrweb/SAMHDA/

45
According to NSDUH, overall prevalence of underage (ages 12–20) alcohol use and binge drinking has shown a gradual decline across all prevalence periods. In 2009, an estimated 30.2 million people (12.0 percent) aged 12 or older reported driving under the influence of alcohol at least once in the past year. Although this reflects a downward trend from 14.2 percent in 2002, it remains a cause for concern. http://www.nida.nih.gov/infofacts/nationtrends.html The decline in illicit drug use by the Nation’s adolescents since the mid- to late-1990s has leveled off. Among 8th, 10th, and 12th graders, most measures of illicit drug use remained unchanged from 2009 to 2010. Marijuana use rose this year—a sharp contrast to the considerable decline of the preceding decade. The downward trend in ecstasy use has been reversed as well, with significant increases this year following a considerable and recent decline in the belief that its use is dangerous.
 aged 12 or older reported driving under the influence of alcohol at least once in the past year. Although this reflects a downward trend from 14.2 percent in 2002, it remains a cause for concern. The decline in illicit drug use by the Nation’s adolescents since the mid- to late-1990s has leveled off. Among 8th, 10th, and 12th graders, most measures of illicit drug use remained unchanged from 2009 to Marijuana use rose this year—a sharp contrast to the considerable decline of the preceding decade. The downward trend in ecstasy use has been reversed as well, with significant increases this year following a considerable and recent decline in the belief that its use is dangerous..")
46
Prescription and over-the-counter (OTC) medications accounted for most of the top drugs abused by 12th graders in the past year. Among 12th graders, past-year nonmedical use of Vicodin decreased from 9.7 percent to 8.0 percent. However, past-year nonmedical use of Oxycontin remained unchanged across the three grades and has increased among 10th graders over the past 5 years. Moreover, past-year nonmedical use of Adderall and OTC cough and cold medicines among 12th graders remained high at 6.5 percent and 6.6 percent, respectively. Complete NSDUH findings are available at www.oas.samhsa.gov/NSDUHLatest.htm. www.oas.samhsa.gov/NSDUHLatest.htm

47
The Partnership at Drugfree.org http://www.drugfree.org/newsroom/new-research-teen-drug-and- alcohol-use-headed-in-wrong-direction

48
http://monitoringthefuture.org/data/10data.html#2010data-drugs

50
TRADITIONAL-AGE COLLEGE STUDENTS: DRUNK IN LAST 30 DAYS http://monitoringthefuture.org/data/10data.html#2010data-drugs

51
High School and Middle School Youth: 5 or more drinks in a row in last 2 weeks

52
High School and Middle School Youth: Any illicit drug in last 30 days

53
High School and Middle School Youth: Any illicit drug other than marijuana High School and Middle School Youth: Any illicit drug other than marijuana in last 30 days

54
High School and Middle School Youth: 30 Day Marijuana Use

55
High School and Middle School Youth: 30 Day Ecstasy Use

61
New and dangerous club drug being sold to high school and college age students. The U.S. Drug Enforcement Administration (DEA) working with the Michigan State Police and local law enforcement agencies have recently discovered the presence of a new and dangerous club drug that is being sold to high school and college age students at "Rave" parties throughout the Detroit and Ann Arbor areas. This substance is known on the street as "Molly", which is 1-(3-Trifluoromethylphenyl) piperazine (TFMPP). This is an extremely dangerous drug, which is clandestinely manufactured and marketed in "Rave Clubs" as a more intense form of Ecstasy. This drug is an off-white powder generally sold in a gelatin capsule. TFMPP and Benzylpiperazine (BZP) were both given emergency controlled substance scheduling by the U.S. Drug Enforcement Administration in September 2002. TFMPP was given Schedule I status, meaning it has a high potential for abuse and no accepted medical use. This drug first appeared on the West Coast of the United States and these recent seizures in Michigan are the first indication of its presence in the metropolitan Detroit area. TFMPP also goes by the names "legal E", "legal X" or "A2". TFMPP can cause increased heart rate, blood pressure and body temperature. http://www.streetdrugs.org/
 working with the Michigan State Police and local law enforcement agencies have recently discovered the presence of a new and dangerous club drug that is being sold to high school and college age students at Rave parties throughout the Detroit and Ann Arbor areas. This substance is known on the street as Molly , which is 1-(3-Trifluoromethylphenyl) piperazine (TFMPP). This is an extremely dangerous drug, which is clandestinely manufactured and marketed in Rave Clubs as a more intense form of Ecstasy. This drug is an off-white powder generally sold in a gelatin capsule. TFMPP and Benzylpiperazine (BZP) were both given emergency controlled substance scheduling by the U.S. Drug Enforcement Administration in September TFMPP was given Schedule I status, meaning it has a high potential for abuse and no accepted medical use. This drug first appeared on the West Coast of the United States and these recent seizures in Michigan are the first indication of its presence in the metropolitan Detroit area. TFMPP also goes by the names legal E , legal X or A2 . TFMPP can cause increased heart rate, blood pressure and body temperature.")
62
High School Youth Parents Community Leaders http://teenalcoholcultures.gmu.edu

63
Literature Review 250 articles, 59 dissertations/theses, 34 government/non-profit reports, 19 books, 19 data sets Telephone Polling 1623 interviews [1014 parents and 609 teens] 522 are matched pairs [parent and teen] Key Informant and Individual Interviews 58 completed [blend of community, school, law, and health] Expert Interviews 28 completed [includes university, research, government, medical, and authors] The methodology incorporated a blend of approaches, and involves the use of a national Advisory Panel. http://teenalcoholcultures.gmu.edu
![ Literature Review 250 articles, 59 dissertations/theses, 34 government/non-profit reports, 19 books, 19 data sets Telephone Polling 1623 interviews [1014 parents and 609 teens] 522 are matched pairs [parent and teen] Key Informant and Individual Interviews 58 completed [blend of community, school, law, and health] Expert Interviews 28 completed [includes university, research, government, medical, and authors] The methodology incorporated a blend of approaches, and involves the use of a national Advisory Panel.](http://images.slideplayer.com/14/4233638/slides/slide_63.jpg)
64
Focus Groups [N=71] 59 with youth [47 high school, 6 middle school, 6 college] 8 with parents 4 with community leaders 513 youth were involved in focus groups 396 high school and 35 middle school youth High school youth were balanced with boys/girls and white/non- white No notable differences were found based on race/ethnicity Few differences were found based on gender Sites included Northern Virginia, Bucks County (PA), Orange County (FL), Minneapolis, Santa Fe (NM), Northern New Jersey, and rural Georgia. No notable differences were found based on setting (urban/rural/suburban) http://teenalcoholcultures.gmu.edu
![ Focus Groups [N=71] 59 with youth [47 high school, 6 middle school, 6 college] 8 with parents 4 with community leaders 513 youth were involved in focus groups 396 high school and 35 middle school youth High school youth were balanced with boys/girls and white/non- white No notable differences were found based on race/ethnicity Few differences were found based on gender Sites included Northern Virginia, Bucks County (PA), Orange County (FL), Minneapolis, Santa Fe (NM), Northern New Jersey, and rural Georgia.](http://images.slideplayer.com/14/4233638/slides/slide_64.jpg " No notable differences were found based on setting (urban/rural/suburban)")
65
Inadequacy of Current Knowledge Much current knowledge is based on survey research. Limited conversational research is found with teens, parents or other front line personnel. Current expert knowledge is often limited. Disjunction Between Formal and Informal Rules Teens and parents have their own practices and beliefs about what is practical and appropriate. These practices and beliefs often diverge sharply from legal codes. http://teenalcoholcultures.gmu.edu

66
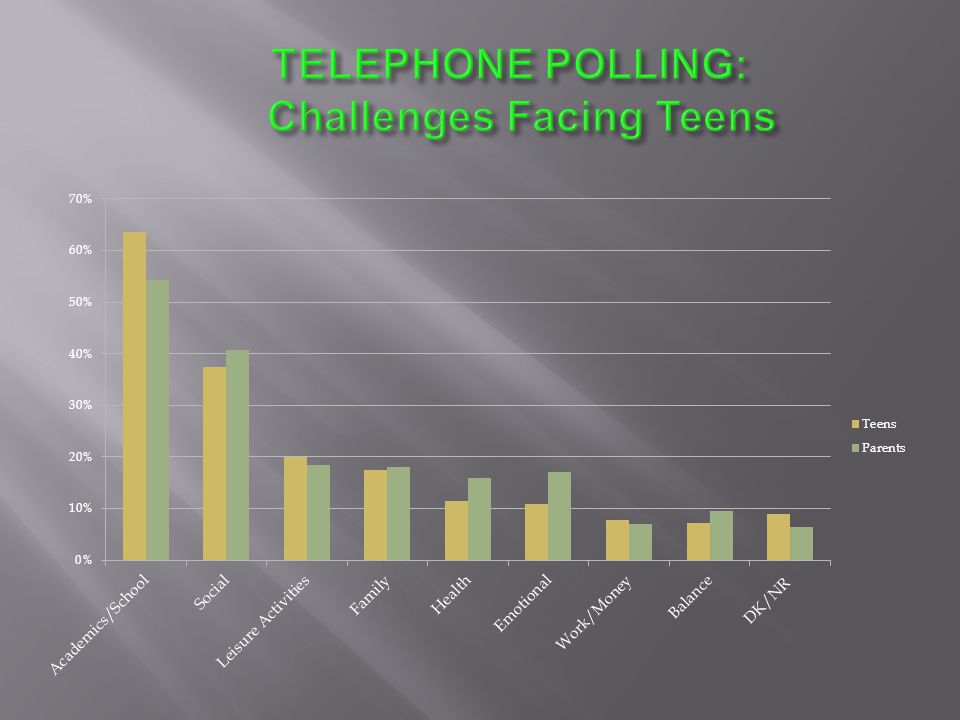
Differences Between Parent and Teen Views Teens cite academic challenges more often than parents. Teens are more likely to cite emotional or social reasons for drinking and for getting drunk. Parents attach more importance to family relationships as motivators for teens’ drinking or not drinking. Extreme Teen Behavior Teens engage in high risk drinking behaviors on a frequent basis. Teens who drink do so for emotional and social reasons.

67
Lack of Helpful Information Teens have minimal knowledge of alcohol’s effects (beyond drinking and driving consequences). Teens and parents are unaware of helpful resources. Teens and parents lack skills for meaningful dialogue on alcohol. Not Sure What to Do Parents and community leaders are unsure how to address teen drinking. Parents and community leaders focus primarily on policy or law enforcement approaches. http://teenalcoholcultures.gmu.edu

76
Teens report that obtaining alcohol is quite easy, through relationships (older siblings, friends, co- workers), places of purchase, theft or party settings. Unlike other studies, our middle school teens report having few to no experiences with alcohol. Boys are typically expected to provide alcohol for girls. http://teenalcoholcultures.gmu.edu

77
Teens drink primarily to get drunk; drinking for taste or mild effects is rare. Teens drink to deal with stress, to facilitate group membership, and to feel better. Teens’ transition to high school is a high-risk time. http://teenalcoholcultures.gmu.edu

78
Early drinking experiences are frequently dangerous “trials by fire” where teens learn by experimentation. While youth are aware of family and legal consequences, they are often confident that they will not get caught. http://teenalcoholcultures.gmu.edu

80
Parents are often unsure how to talk to their teens and to other parents about teen alcohol consumption. Parents feel a lack of information and guidance. Parents are aware of the divergence between legal codes and informal practices. Public moralism and zero tolerance laws make frank conversation with their teen(s) and other parents difficult. http://teenalcoholcultures.gmu.edu
 and other parents difficult.")
81
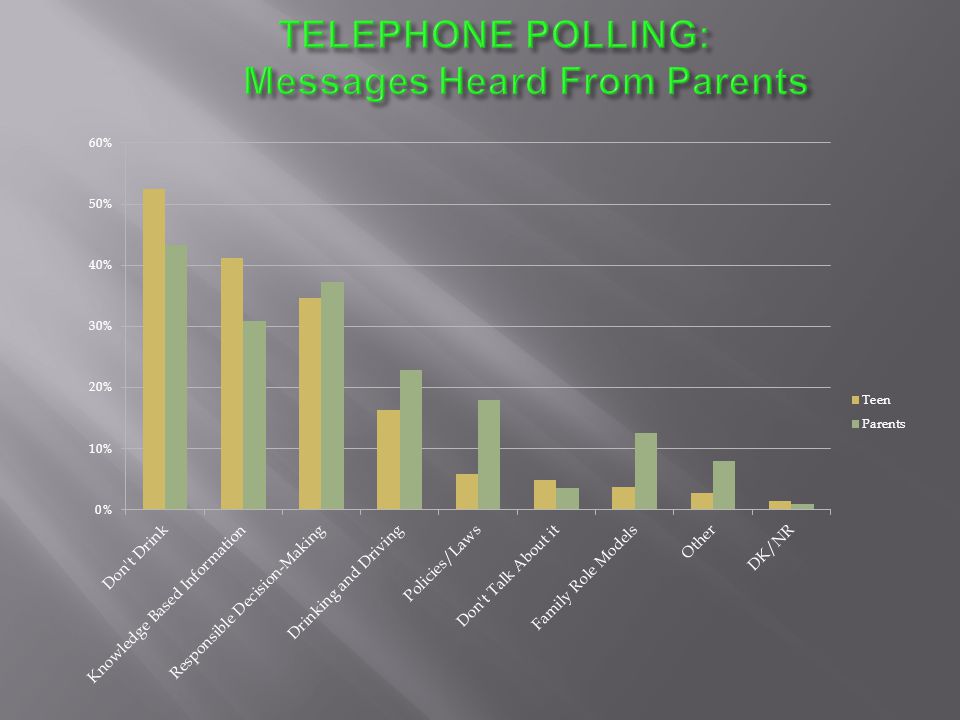
Parents are four times as likely as teens to think that alcohol education programs, such as those at school, are effective. Parents believe that schools emphasize informational and legal messages, including don’t drink alcohol affects your health don’t drink and drive alcohol use is illegal under 21 Teens report limited to no conversations on alcohol with parents during teen years. http://teenalcoholcultures.gmu.edu

82
Teens want more information about alcohol. Teens want judgment-free information about alcohol from sources they can trust; they do not trust school-based education programs. Most teens report that alcohol is talked about by school authorities, and report informational, legal and proscriptive messages. Whatever their actual behavior, teens report hearing and respecting messages about not drinking and driving. http://teenalcoholcultures.gmu.edu

83
Teens typically don’t see drinking as a problem, unless they get in trouble with those in authority. Teens see other teens’ drinking as more of a problem than their own, even if the behavior is essentially the same. Teens overwhelmingly deny the importance of peer pressure in decisions to consume or not consume alcohol. However, teens have a poorly developed concept of peer pressure. Teens see drinking as pleasurable and often essential to socializing with other teens. For many teens, drinking is a primary extracurricular activity. http://teenalcoholcultures.gmu.edu

84
Underlying or Core Factors Intrinsic or Vital FactorsExtrinsic FactorsContextual Factors *Strong core values *Feel connected to past and future *Has a sense of purpose *Family bonds *Feeling loved and listened to *Feeling capable (confidence) *Aware of areas of concern *Knows where to turn for assistance *Feels supported *Has balance in life *Good coping skills to deal with anxiety, stress, high expectations *Friends provide support *Friends encourage behavior change as needed *Spend family time together *Healthy family *Has open communication / conversation with parents *Has meals with families *Has good sense of personal boundaries *Feels affirmation *Has clear and reasonable expectations *Skills to interact with others *Sees parents as partners and guides *Reflect on self *Has positive role models *Engaged in activities, clubs *Has opportunity to learn by doing, experiment, make mistakes *Is encouraged to stretch and extend comfort zone The Teen’s WorldThe Role of Alcohol http://teenalcoholcultures.gmu.edu
 *Aware of areas of concern *Knows where to turn for assistance *Feels supported *Has balance in life *Good coping skills to deal with anxiety, stress, high expectations *Friends provide support *Friends encourage behavior change as needed *Spend family time together *Healthy family *Has open communication / conversation with parents *Has meals with families *Has good sense of personal boundaries *Feels affirmation *Has clear and reasonable expectations *Skills to interact with others *Sees parents as partners and guides *Reflect on self *Has positive role models *Engaged in activities, clubs *Has opportunity to learn by doing, experiment, make mistakes *Is encouraged to stretch and extend comfort zone The Teen’s WorldThe Role of Alcohol")
85
Underlying Causes Intrinsic FactorsExtrinsic FactorsContextual Factors *Stress *Feel pressure *Discouragement *Disenfranchised *Lonely *Seeking own identity *Insecure *Hopelessness *Lack coping skills *Boredom (nothing to do) *Not comfortable being alone *Lack of goals or mission *Escape *To experience things themselves *No reflection *To fit in *To be older *To rebel *Unrealistic expectations (life, situations) *Lack knowledge and information *Lack meaningful conversation with parents *Lack of role models *Allure (TV, songs, ads) *No substantive, consistent legal consequences *Conflicting messages (adults drink) * Educational dishonesty, inadequacy, mistrust *Peer acceptability *Peers’ encouragement *Ease of access *Party availability *Alcohol is readily available *Societal acceptability The Teen’s WorldThe Role of Alcohol http://teenalcoholcultures.gmu.edu
 *Not comfortable being alone *Lack of goals or mission *Escape *To experience things themselves *No reflection *To fit in *To be older *To rebel *Unrealistic expectations (life, situations) *Lack knowledge and information *Lack meaningful conversation with parents *Lack of role models *Allure (TV, songs, ads) *No substantive, consistent legal consequences *Conflicting messages (adults drink) * Educational dishonesty, inadequacy, mistrust *Peer acceptability *Peers’ encouragement *Ease of access *Party availability *Alcohol is readily available *Societal acceptability The Teen’s WorldThe Role of Alcohol")
86
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors http://teenalcoholcultures.gmu.edu

87
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors

88
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors

89
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors

90
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors

91
FRAMEWORK FOR YOUTH RISKY ALCOHOL DECISIONS Underlying Causes Intrinsic Factors Extrinsic Factors Contextual Factors

92
TYPE OF EFFORT PolicyProgramTrainingEnvironment GROUP OR ORGANIZATION Schools Consistently implemented rules and regulations Standards for school employees and visitors Curriculum that is meaningful Clubs and organizations After school activities Personnel preparation with identification and referral School bonding and community-building activities Recognition for positive contributions Law Enforcement Laws and policies throughout the community Enforcement of laws Sponsor local events Participate in community activities Mentoring youth Community resource officers in school and community settings Health Services Services available for teens Public awareness materials Community forum and dialog How to identify problematic use How to be supportive Promote as trusted source Spokespersons Community Standards and guidelines Community forum and dialog Prepare adults and community leaders to understand today’s youth needs Group meeting behavior Volunteering for community events Public awareness activities Youth-Serving Organizations Engage in establishing community policies Community-wide activities Mentoring opportunities for older teens Provide awards for positive contributions http://teenalcoholcultures.gmu.edu

94
Mephedrone, also known as 4-methylmethcathinone ( 4-MMC ), or 4-methylephedrone, is a synthetic stimulant and entactogen drug of the amphetamine and cathinone classes. Slang names include meph, [5] drone, [6] and MCAT. [7] It is reportedly manufactured in China and is chemically similar to the cathinone compounds found in the khat plant of eastern Africa. It comes in the form of tablets or a powder, which users can swallow, snort or inject, producing similar effects to MDMA, amphetamines and cocaine. syntheticstimulantentactogendrugamphetaminecathinone [5] [6] [7]khateastern Africa MDMAamphetaminescocaine As well as producing the intended stimulant effects, negative side effects occur when mephedrone is used, with teeth grinding the most common. The metabolism of mephedrone has been studied in rats and humans, and the metabolites can be detected in urine after usage. Nothing is known about the potential neurotoxicity of mephedrone, but scientists have suggested possible dangers associated with its use based on its similarity to other drugs. Several people have died after consuming mephedrone, but some deaths that the media attributed to the drug were later determined to have been caused by other factors.side effectsteeth grindingmetabolismneurotoxicity Mephedrone was first synthesized in 1929 but did not become widely known until it was rediscovered in 2003. By 2007 mephedrone was reported to be available for sale on the internet, by 2008 law enforcement agencies had become aware of the compound and by 2010 it had been reported in most of Europe, becoming particularly prevalent in the United Kingdom. Mephedrone was first made illegal in Israel in 2008, followed by Sweden later that year. In 2010 it was made illegal in many European countries and in December 2010, the EU ruled it illegal across Europe. In Australia, New Zealand, and the USA it is considered an analog of other illegal drugs and can be controlled by laws similar to the Federal Analog Act. In the USA, this only applies if the drug is sold for human consumption, allowing it to be sold legally if labeled as 'plant food' or 'bath salts'.analogFederal Analog Act

95
Buy 4-MMC/ Mephedrone, bk-MDMA/Methylone, MDAI, MDPV, 4-MEC/ Modified MEphedrone and other research chemicals. Each product has its own unique qualities. We import direct from the factory so we can guarantee a quality product - over 99.9% purity. Plantfeedshop is one of the most reputable and trusted retailers of, Mephedrone, Methylone, MDAI, 4-MEC and MDPV - We have built our superb reputation by offering our customers a pleasant & professional shopping experience, excellent quality products with FREE delivery and friendly customer support. We also wholesale Mephedrone, Methylone, MDAI, 4-MEC and MDPV contact us for more details. When you buy research chemicals from us you are guaranteed of the highest quality available on the market, high purity products, secure payment, very discreet, fast and discreet international delivery. International customers please do ensure you check your national laws before ordering.

96
We can supply folowing reserch chemicals and herbals: 4-MMC/ Mephedrone MDPV bk-MDMA/ Methylone 4-MEC/ MODIFIED MEPHEDRONE MDAI Marijuana/ Cannabis seeds Sumatra Red Vein Kratom /Mitragyna speciosa Sumatra White Vein Kratom / Mitragyna speciosa Borneo Red Vein Kratom / Mitragyna speciosa Borneo White Vein Kratom / Mitragyna speciosa Salvia Divinorum Common names used for this chemical: 4-MMC, 4MMC, 4-methylmethcathinone, Mephedrone, Methedrone, Methadrone, Mephadrone, M-CAT, MM-CAT Meow/Miaow Plant Feeder 4-mec 4-methylethylcathinone. Mephedrone Substitute Legal Mephedrone Methylone, bk-MDMA, Arlone, Explosion, M1, Ease MDPV, Methylenedioxypyrovalerone MDAI; 5,6-Methylenedioxy-2-aminoindane HCl; 6,7-dihydro-5H-cyclopenta[f][1,3]benzodioxol- 6-amine

97
The term bath salts refers to a range of water-soluble, usually inorganic solid products designed to be added to a bath. They are said to improve cleaning, improve the experience of bathing, serve as a vehicle for cosmetic agents, and some even claim medical benefits. [ citation needed ] Bath salts have been developed which mimic the properties of natural mineral baths or hot springs. Such salts include:inorganic bathing citation neededhot springs magnesium sulfatemagnesium sulfate (Epsom salts) sodium chloridesodium chloride (table salt) sodium bicarbonatesodium bicarbonate (baking soda) sodium hexametaphosphatesodium hexametaphosphate (Calgon, amorphous/glassy sodium metaphosphate) sodium sesquicarbonate borax Although, chemically speaking, many organic substances commonly used in bath water (such as soap and many other surfactants) are salts, these are not referred to as "bath salts", as they are not used in the form of hard, crystalline granules. On the other hand, some organic salts such as sodium citrate can be used in bath salts. soapsurfactants sodium citrate Fragrances and colors are often added to bath salts, and one purpose of salts is as a vehicle or diluent to extend fragrances, which are otherwise often too potent for convenient measurement or use. Other common additives to bath salts are oils (agglomerating the salts to form amorphous granules, the product being called "bath beads" or "bath oil beads"), foaming agents, and effervescent agents. diluent Although bath salts are often packaged for retail in windowless boxes or bags, the more attractive versions may also be displayed in transparent containers. For instance, the needlelike appearance of sodium sesquicarbonate crystals makes them attractive for such purposes.
 sodium chloridesodium chloride (table salt) sodium bicarbonatesodium bicarbonate (baking soda) sodium hexametaphosphatesodium hexametaphosphate (Calgon, amorphous/glassy sodium metaphosphate) sodium sesquicarbonate borax Although, chemically speaking, many organic substances commonly used in bath water (such as soap and many other surfactants) are salts, these are not referred to as bath salts , as they are not used in the form of hard, crystalline granules. On the other hand, some organic salts such as sodium citrate can be used in bath salts. soapsurfactants sodium citrate Fragrances and colors are often added to bath salts, and one purpose of salts is as a vehicle or diluent to extend fragrances, which are otherwise often too potent for convenient measurement or use. Other common additives to bath salts are oils (agglomerating the salts to form amorphous granules, the product being called bath beads or bath oil beads ), foaming agents, and effervescent agents. diluent Although bath salts are often packaged for retail in windowless boxes or bags, the more attractive versions may also be displayed in transparent containers. For instance, the needlelike appearance of sodium sesquicarbonate crystals makes them attractive for such purposes..")
98
In the UK to avoid being controlled by the Medicines Act, designer drugs such as mephedrone have been described as "bath salts" or "plant food", despite the compounds having no history of being used for these purposes. Due to these inaccurate descriptions of products, it is possible that selling the compounds under these descriptions could be illegal under the Trade Descriptions Act. [25][26][27]Medicines Act mephedroneTrade Descriptions Act [25][26][27] In the USA similar descriptions have been used to describe mephedrone as well as methylenedioxypyrovalerone (MDPV). [28] methylenedioxypyrovalerone [28]
. [28] methylenedioxypyrovalerone [28].")
Similar presentations

























.>")

 Briefing for DHHS, September 5, 2007 Joe Gfroerer Office of Applied Studies Substance.>")


>")





>")

>")