Download presentation
Presentation is loading. Please wait.

2
Dementia: So Far, So Near, Majid Barekatain, M.D., Associate Professor of Psychiatry Neuropsychiatrist Isfahan University of Medical Sciences 27-28 Ordibehesht 1392 April 16-17, 2013

3
حرفهای ما هنوز ناتمام.... تا نگاه میکنی : وقت رفتن است باز هم همان حکایت همیشگی ! پیش از آنکه با خبر شوی لحظهی عزیمت تو ناگزیر می شود آی..... ای دریغ و حسرت همیشگی ناگهان چقدر زود دیر میشود ! قيصر امين پور

5
Lancet 1997; 349: 1546-49

7
Prevalence of Dementia Increases with Age

8
Projected Prevalence of AD 16 14 12 0 2 4 6 8 10 2000 20102020203020402050 4 5.8 6.8 8.7 11.3 14.3 Millions 4.5 Million AD Cases Today— Over 14 Million Projected Within a Generation Year Evans DA et al. Milbank Quarterly. 1990;68:267-289.

9
Global Aging

10
Definitions

11
Normal Mild Cognitive Impairment Dementia

12
Dementia An acquired disorder of intellectual impairment produced by a dysfunctional brain

13
Dementia Definition Syndrome of acquired persistent intellectual impairment Persistent deficits in at least three of the following cognitive domains: – memory – Language – Visuospatial – personality or emotional state – Higher cognition Resulting in impairment in Activities of Daily Living (ADL)
")
14
Mild Cognitive Impairment (MCI) Definition Memory complaint usually corroborated by an informant Objective memory impairment for age - that represents a change in function for the person Essentially preserved general cognitive function Largely intact functional activities Not demented Alzheimer’s disease may start like this but many non- AD conditions present like this also Petersen J Int Med 2004;256;183-194
 Definition Memory complaint usually corroborated by an informant Objective memory impairment for age - that represents a change in function for the person Essentially preserved general cognitive function Largely intact functional activities Not demented Alzheimer’s disease may start like this but many non- AD conditions present like this also Petersen J Int Med 2004;256;")
15
Rates of MCI Conversion to Dementia Vary from 1% - 25% per year to AD depending on the definition used and measurement instruments 10% - 12% per year to AD is typical 57% conversion to dementia after 3 years in one study 25% do not convert to dementia even with long term follow-up Chertkow et al. Neurology 2001;56:B46

16
Symptoms of AD Cognitive symptoms include: – Memory loss and impaired temporal orientation – Impaired praxis and spatial ability – Language and executive disturbance Functional symptoms include: – Reduced ability to carry out IADL/ADLs, e.g., dressing, handling money, personal hygiene Henderson & Jorm. In: Maj M, Sartorius N, eds. © 2000 John Wiley & Sons Ltd, Chichester, UK

17
Behavioural/psychological symptoms include: Mood swings Agitation Aggression Wandering The type and timing of symptom expression is highly variable between patients Henderson & Jorm. In: Maj M, Sartorius N, eds. © 2000 John Wiley & Sons Ltd, Chichester, UK Symptoms of AD

18
Cognitive deficits in AD Memory impairment – difficulty in learning new information, and/or forgetting previously learned material Aphasia: impaired language function Apraxia: the inability to perform previously learned skills in the absence of defects in motor or sensory function Agnosia: a failure to recognise objects, eventually progressing to not recognising family members, or their own reflection Decline in executive functioning Spatial and temporal orientation may also be affected Mendez MF, Cummings J. Dementia. A clinical approach. 3rd ed. Philadelphia: 2003

19
Short Term Memory Short-term memory (STM) – Ability to register information – Ability to recall the registered information Free recall (MCI, Mild AD) Cued recall (Mild to Moderate AD) Recognition (Moderate AD) Mendez MF, Cummings J. Dementia. A clinical approach. 3rd ed. Philadelphia: 2003

20
Long term memory Declarative (Moderate AD) – Concepts (semantic) Frontal lobe – Events (episodic) Cortical sensory association areas (auditory and visual) – Words (lexical) temporal lobe (hippocampus) Procedural (Severe AD) – Memory for motor tasks basal ganglia & motor cortex Mendez MF, Cummings J. Dementia. A clinical approach. 3rd ed. Philadelphia: 2003

21
Language Language is the encoding/decoding of a message to communicate thoughts with words or symbols Language can be: – Spoken / Comprehended – Written / Read – Pictured – Gestured Domenico RA. Adv Exp Med Biol 1990; 282:79-88

22
Language deficits Mild AD Difficulties with: – word finding/naming – abstract or complex concepts – pronouns – storytelling – humour / sarcasm – initiating conversation – maintaining topic Use of: – semantic paraphasias (substituted words) – circumlocution – empty words (it, stuff, thing) – gesture Relatively intact – comprehension and repetition Domenico RA. Adv Exp Med Biol 1990; 282:79-88

23
Language deficits Moderate AD Decreased word fluency / vocabulary, confrontation naming Few ideas and frequent repeating Poor use of pronouns Poor pragmatics – e.g.- poor topic maintenance, little sensitivity to conversational partners Circumlocution increased More difficulty with complex language comprehension and production Domenico RA. Adv Exp Med Biol 1990; 282:79-88

24
Language deficits Severe AD Severely diminished naming Exhibits more paraphasias (word and sound substitution), echolalia (repetition of other’s speech), palilalia (rep. of own speech) Poor comprehension Use of jargon and rambling speech, incoherence Decreased eye contact Diminished output or may be meaningless or bizarre; may become mute Domenico RA. Adv Exp Med Biol 1990; 282:79-88
 Poor comprehension Use of jargon and rambling speech, incoherence Decreased eye contact Diminished output or may be meaningless or bizarre; may become mute Domenico RA. Adv Exp Med Biol 1990; 282:")
25
Communication Broad term encompassing all the ways we send and receive messages Includes speaking, listening, reading, writing, gesturing, miming Requires a sender and a receiver

26
Communication Verbal – Words Non verbal – Facial expression – Eye contact – Body language – Gesture – Paralinguistics Intonation, loudness, pitch, rithm

27
Functional communication The ability to receive or to convey a message, regardless of the mode, to communicate effectively and independently in a given environment Functional communication involves also functional abilities that enable patients to make themselves understood by relatives and carers. American Speech-Language-Hearing Association (ASHA). Functional Communication Measures Project. Rockville,MD 1990; ASHA., Domenico RA. Adv Exp Med Biol 1990; 282:79-88.
. Functional Communication Measures Project. Rockville,MD 1990; ASHA., Domenico RA. Adv Exp Med Biol 1990; 282:")
28
Executive Function Planning, (Mild to Moderate AD) Working memory, (MCI, Mild AD) Attention, (MCI, Mild AD) Problem solving, (Mild to Moderate AD) Verbal reasoning, (Moderate to Severe AD) Inhibition, (Moderate to Severe AD) Mental flexibility, (Mild to Moderate AD) Task switching, (Mild to Moderate AD) Initiation and monitoring of actions, (Moderate to Severe AD)
 Working memory, (MCI, Mild AD) Attention, (MCI, Mild AD) Problem solving, (Mild to Moderate AD) Verbal reasoning, (Moderate to Severe AD) Inhibition, (Moderate to Severe AD) Mental flexibility, (Mild to Moderate AD) Task switching, (Mild to Moderate AD) Initiation and monitoring of actions, (Moderate to Severe AD)")
29
Symptom progression pattern in patients with Alzheimer’s disease Stage of Global Deterioration Scale (GDS) Adapted from: Reisberg et al. Am J Psychiatry 1982; 139: 1136–1139 MMSE stages Anxiety Misplacing objects Forgetting names Unable to recall names of close family members Disoriented to time and place Unable to perform complex tasks Basic psychomotor skills are lost Delusional behaviour Incontinence Forgetting names one formerly knew well Word and name finding deficit becomes evident Flattening of affect and withdrawal from challenging situations Difficulties dressing properly Can no longer care for oneself Caregiver burden 6 7 Loss of speech, locomotion, consciousness; full-time care needed 2 3 4 5 Severe <10 Moderate 10–19 Mild 20–26 1 0 5 10 15 20 Years after onset

30
Progression and symptoms of AD Pattern of symptoms over time in patients with AD Gauthier. (Ed) Clinical Diagnosis and Management of Alzheimer’s Disease. Third Edition, Informa Healthcare Progression of Alzheimer’s disease MildSevere Deterioration Mood Cognitive function Functional autonomy Behaviour Motor function
 Clinical Diagnosis and Management of Alzheimer’s Disease. Third Edition, Informa Healthcare Progression of Alzheimer’s disease MildSevere Deterioration Mood Cognitive function Functional autonomy Behaviour Motor function.")
31
Difficulties prompting the seeking of help: overview Difficulties listed in order of decreasing importance Area of difficulty: CognitionActivities of daily living BehaviourCommunication Memory/confusion Concentration/attention Orientation/getting lost Recognising people Finding belongings Financial activities Shopping Using telephone Cooking Personality changes Depression Irritability Social withdrawal Wandering Following conversation Writing/reading Speaking Comprehension of language Georges et al, Int J Geriatr Psychiatry 2008; 23 (5): 546–551
: 546–551")
32
Methods of Screening

33
Screening with Biomarkers

34
Biomarkers in AD Cerebrospinal fluid (CSF) biomarkers – Tau ( in CSF in AD) – A 42 ( in CSF in AD) – Neural thread protein (NTP) – Homocysteine ( level, risk of AD) – Isoprostanes (oxidative/nitrative damage - levels in blood and CSF in AD) – Sulfatide ( in CSF in AD) Blood and urine biomarkers – Genetic blood tests and genotyping – Plasma A 42, Homocysteine, isoprostanes, sulfatide – Urine neural thread protein (NTP)
 biomarkers – Tau ( in CSF in AD) – A 42 ( in CSF in AD) – Neural thread protein (NTP) – Homocysteine ( level, risk of AD) – Isoprostanes (oxidative/nitrative damage - levels in blood and CSF in AD) – Sulfatide ( in CSF in AD) Blood and urine biomarkers – Genetic blood tests and genotyping – Plasma A 42, Homocysteine, isoprostanes, sulfatide – Urine neural thread protein (NTP)")
35
Screening with Neuroimaging

36
Early Diagnosis: Structural Neuroimaging Volumetric measurement of hippocampus and entorhinal cortex atrophy with MRI is sensitive (95%) but not specific (40%) for AD Change in MRI hippocampal volume may be predictive over time in both MCI and individuals at genetic risk for AD 7-Tesla and 8-Tesla MRI being used in AD research Laakso et al. Neurology 1996;46:678-81 Golomb et al. Neurology 1996;47:810-3 Whitaker et al. Society for Neuroscience 2001

38
Gray Matter Reductions in AD Using Voxel Based Morphometry Alexander GE et al., ADNI MRI Core Team, 2007

39
Functional Neuroimaging: PET PET shows hypometabolism in bilateral parietal, temporal, and posterior cingulate cortex in AD subjects and those who are asymptomatic but at increased risk for AD (those with Apo E 4) PET predicted 94% of mild cognitive impairment (MCI) subjects whose disease progressed to dementia during a 3 year period Minoshima et al. J Nucl Med 1995;36:1238-48 Minoshima et al. Ann Neurol 1997;42:85-94 Small et al. JAMA 1995;273:942-47

40
Typical AD PET Scan Provided courtesy of M. Mega, MD, PhD, Department of Neurology, UCLA School of Medicine. Normal BrainAD Brain

41
Cognitive Screening

42
Examples of Brief Cognitive Assessment/Screening Tests MMSE Clock Drawing Test Mini-Cog AD8 7-minute Screen Montreal Cognitive Assessment (MoCA) Neuropsychiatry Cognitive Assessment Tool (NUCOG) Self-Administered Gerocognitive Examination (SAGE)
 Neuropsychiatry Cognitive Assessment Tool (NUCOG) Self-Administered Gerocognitive Examination (SAGE)")
43
MMSE Score: 0 (worst) - 30 (best) Tests orientation, attention, mental control, calculations, delayed memory (no clueing), language, and constructional praxis Easy to use, well known Not great for frontal or executive functions Sensitivity 78% and specificity 84% for dementia with a cutoff of 26/30 Takes 7 to 10 minutes; needs examiner PAR bought rights - costs about $1 per use Folstein et al. J Psychiat Res 1975;12:189-98 Feher et al. Arch Neurol 1992;49:87-92

44
Folstein et al. J Psychiat Res 1975;12: 189-98 MMSE

46
Mini-Mental State Examination: Typical change over time Mild Cognitive Impairment (MCI)
")
47
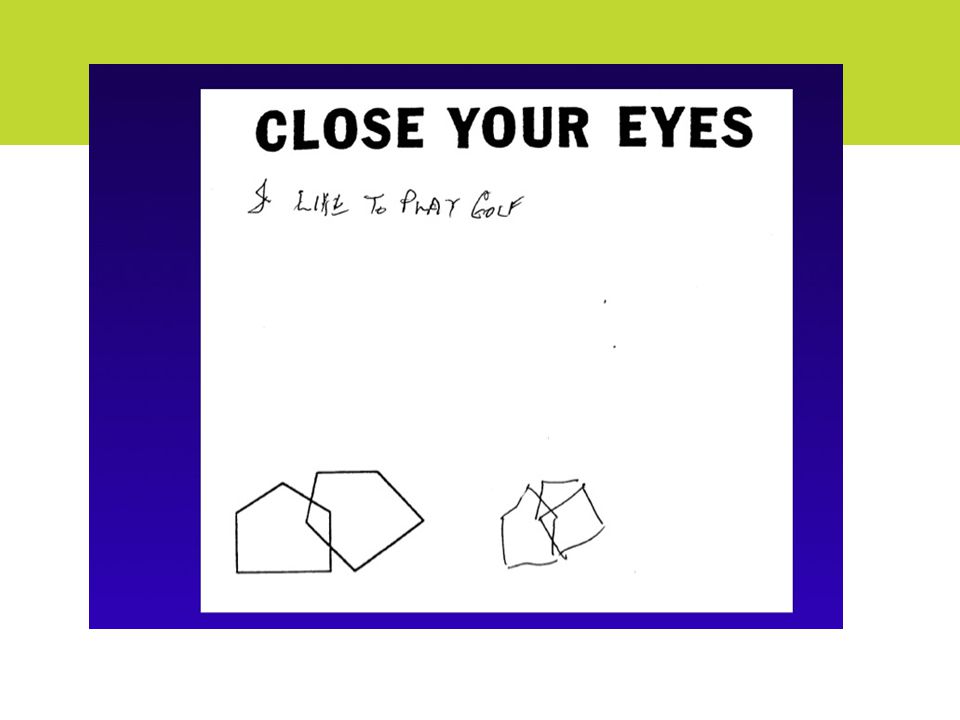
Clock Drawing Test Various scoring methods Tests constructional praxis, visuospatial skills, and executive functioning Easy to use, well known Limited in evaluating other cognitive domains Sensitivity 83% and specificity 72% for AD Takes 1 minute; needs no examiner Shulman et al. Int Geriatr Psychiatry 1986;1:135-40 Cahn et al. Arch Clin Neuropsych 1996;11:529-39

48
Early Diagnis: Cognitive Screening

49
Mini-Cog 3-item recall and clock drawing Easy to use Limited in evaluating other cognitive domains Sensitivity 76% and specificity of 89% for dementia Score not influenced by language or education Takes 3 minutes; needs examiner Borson S et al. Int J Geriatr Psychiatry 2000;15:1021-1027 Borson S et al. JAGS 2003;51:1451-1454

50
Mini-Cog

51
AD8 Score: 0 (best) - 8 (worst) Informant rates changes in the patient’s judgment, interests, memory, functioning, and orientation Easy to use Does not measure patient cognition Sensitivity 84% and specificity 80% for dementia with a cutoff of 2 or greater Takes 3 minutes; needs examiner and informant Folstein et al. J Psychiat Res 1975;12:189-98 Feher et al. Arch Neurol 1992;49:87-92

52
AD8 Galvin et al. Neurology 2006;67:1942- 1948

53
7 Minute Screen Special scoring calculator required Tests orientation, memory, clock drawing, verbal fluency Not easy to use in primary care office Low scores very specific for AD Sensitivity 92% and specificity 96% for AD vs normal controls Takes 7 - 12 minutes; needs examiner Solomon et al. Arch Neurol 1998;55:349-55

54
7 Minute Screen

55
Montreal Cognitive Assessment (MOCA) Score: 0 (worst) - 30 (best) Tests orientation, memory, clock drawing, constructions, verbal fluency, naming, repetition, attention, abstraction, calculations, executive (trails B) Not easy to give in primary care office Sensitivity 100% and specificity 87% for AD vs normal controls with a cutoff of 26/30 Takes 10-13 minutes; needs examiner Nasreddine et al. J Am Geriatr Soc 2005;53:695-699

56
MOCA Nasreddine et al. J Am Geriatr Soc 2005;53:695-699

57
Self-Administered Gerocognitive Exam (SAGE) Score: 0 (worst) - 22 (best) Tests orientation, memory, language, fluency, naming, visuospatial, abstraction, calculations, executive functioning, and problem solving Self-administered, easy to use Limited memory evaluation; excellent executive measures Takes 10 to 15 minutes; needs no examiner Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.edu

58
SAGE Page 1 at sagetest.osu.edu Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.edu

59
SAGE Page 2 at sagetest.osu.edu Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.edu

60
SAGE Page 3

61
at sagetest.osu.edu Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.edu SAGE Page 4

62
Staged Screening: Impact of Diagnosis

63
Screening for Cognitive Impairment No cognitive screening test is diagnostic If normal, serious conditions are less likely The “worried well” can be relieved that they were “tested” and they did fine Serial screening could be suggested over time If abnormal, further evaluation may be considered

64
Staged Screening Approach for Cognitive Impairment One single test or score should not be the only criteria to embark on an expensive dementia evaluation Doing a screening process in stages may provide better evidence for diagnosis of MCI or dementia A staged screening process is recommended

65
و.... ناگهان چقدر زود دير مي شود !

Similar presentations








 Training Program>")











 Josepha A. Cheong, MD University of Florida Departments of Psychiatry.>")


 have included.>")