Download presentation
Presentation is loading. Please wait.

1
Implantation & Equipment Implantation & Equipment Department of Thoracic & Cardiovascular Surgery Seoul National University Hospital

2
Types of Pacemaker Temporary Pacemaker Permanent Pacemaker

3
The Pacemaker System Patient Lead Pacemaker Programmer Lead Pacemaker

4
Pacing System Analysis Ohm’s law ; R=E/I R; resistance in ohms E; potential in volts I ; current in amps Unipolar system: the negative alligator clip of the cable is attached to the electrode(anode) and the positive clip to an indifferent electrode(12-15cm2, stainless steel) Bipolar system: the cathode(tip electrode) is usually the most proximal(pin) terminal and anode(ring electrode) is connected to the less proximal(ring) terminal of the lead
 and the positive clip to an indifferent electrode(12-15cm2, stainless steel) Bipolar system: the cathode(tip electrode) is usually the most proximal(pin) terminal and anode(ring electrode) is connected to the less proximal(ring) terminal of the lead")
5
Pacing Threshold & Sensitivity Current threshold(mA) is the quantity of electron/ion flow across the electrode that is required to initiate depolarization of the myocardium. This may also be expressed in terms of current density or current per unit of electrode surface area, usually milliamps per square millimeter The voltage threshold(V) is the amount of potential drop required to maintain this current flow Lead impedance is a measure of the total resistance to current flow along the lead conductors, across the electrode-tissue interface, and across the body tissues
 is the amount of potential drop required to maintain this current flow Lead impedance is a measure of the total resistance to current flow along the lead conductors, across the electrode-tissue interface, and across the body tissues.")
6
Pacing Threshold & Impedance Pulse generator and lead along the body provide a continuous circuit for current flow and the total pacing system resistance is comprised of three part Lead conductor and tissue resistance are relatively constant, while polarization resistance increases throughout the period during which current is flowing Largely as a result of polarization resistance, lead impedance varies directly with pulse duration and current amplitude and inversely with electrode surface area

7
Stimulation Threshold & Resistance With time, a layer of fibrosis forms around the electrode tip, causing separation of the electrode surface and viable tissue The stimulation threshold at implant will provide a basis for estimating the expected rise in thresholds that results from this fibrotic buildup Threshold may rise transiently to levels of 4 to 5 times those at implant but generally decline after 14-21 days to levels of 2 or 3 times the acute values Newer electrode materials and configuration may lessen the development of the fibrous capsule, thus decreasing both transient & permanent rises in threshold

8
Pacing Threshold & Impedance Pulse generator and lead along the body provide a continuous circuit for current flow and the total pacing system resistance is comprised of three part Lead conductor and tissue resistance are relatively constant, while polarization resistance increases throughout the period during which current is flowing Largely as a result of polarization resistance, lead impedance varies directly with pulse duration and current amplitude and inversely with electrode surface area

9
Pacing System Resistance Lead conductor elements 60-150 ohms Body tissues 200-500 ohms Polarization resistance 15-35% ( The alignment of oppositely charged ions at the electrode-tissue interface during a pacing impulse)
")
10
Acceptable Threshold Limit (Acute) Acute implant stimulation threshold –Atrium Less than 1.0-1.5 Volts Less than 1.5-2.0mA(current) –Ventricular Less than 1.0 Volts Less than 2.0mA(current) Acute implant sensing thresholds –Atrium Greater than 1.5-2.0 mV –Ventricular Greater than 5.0 mV Acute implant lead impedance. Both chamber within 300-1000 ohms

11
Acceptable Threshold Limit (Chronic) Chronic voltage stimulation threshold Less than 50% of nominal voltage output of pulse generator at pulse width <1.0 Chronic current stimulation threshold –Atrium ; less than 3.0-3.5mA –Ventricular; less than 3.0-3.5mA Chronic sensing thresholds –Atrium ; greater than 1.0 mV –Ventricular ; greater than 4.0 mV Chronic lead impedance –Atrium ; 300-1000 ohms –Ventricular ; 500-1000 ohms
 Chronic voltage stimulation threshold Less than 50% of nominal voltage output of pulse generator at pulse width <1.0 Chronic current stimulation threshold –Atrium ; less than mA –Ventricular; less than mA Chronic sensing thresholds –Atrium ; greater than 1.0 mV –Ventricular ; greater than 4.0 mV Chronic lead impedance –Atrium ; ohms –Ventricular ; ohms")
12
Acute Threshold Measurement Factors Type of lead Lead-tissue interface Location of lead within the heart Length of time after lead fixation

13
Optimal Placement of Leads Acceptable eletrophysiologic values Visual assessment on fluoroscopic examination Adequate securing of the lead and is in good contact with viable tissue

14
Electrophysiologic Complications Pacemaker syndrome Ventricle Atrial Pacemaker-mediated tachycardia

15
Venous Route Subclavian vein Cephalic vein External jugular V Internal jugular V Transvenous Implantation

19
Atrial Endocardial Placement

20
Ventricle Atrial

21
Epicardial Implantation Indications Multiple endocardial lead failure Abnormalities of thoracic venous anatomy Presence of congenital heart disease Presence of tricuspid valve prosthesis Repeated development of exit block of endocardial lead Small infants and occasionally in children

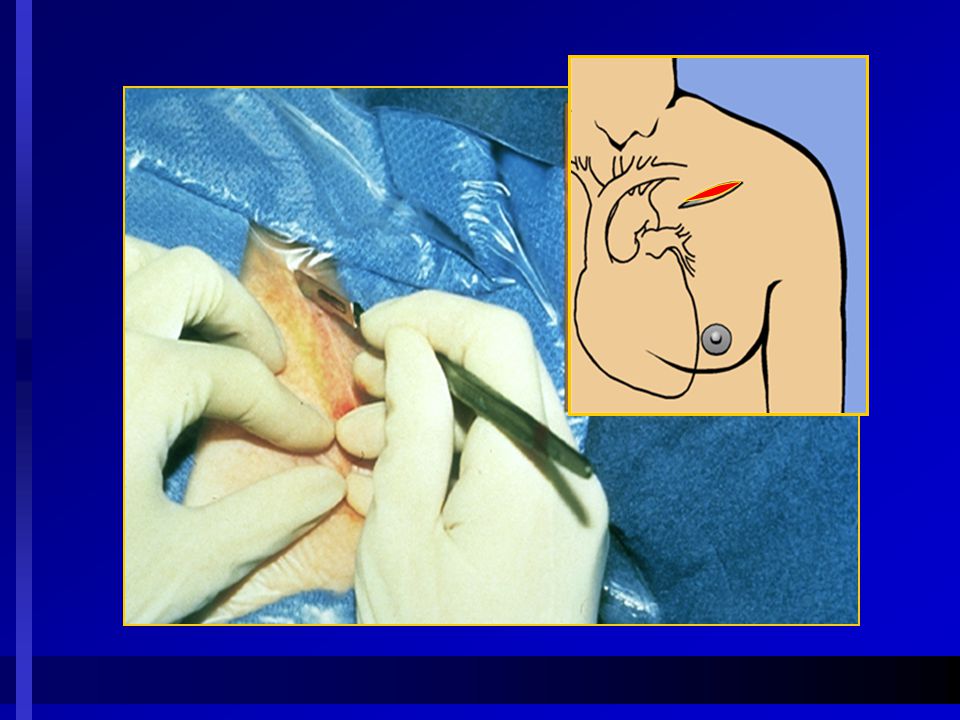
22
Epicardial Implantation A; Subxiphoid approach B; Anterior thoracotomy Ideal electrode distance in bipolar pacing; 0.8-1.2cm

23
Connection of the leads to the Pacing System Analyzer (PSA)
")
24
Connection to Pacemaker Insure the leads are placed behind the Pacemaker

25
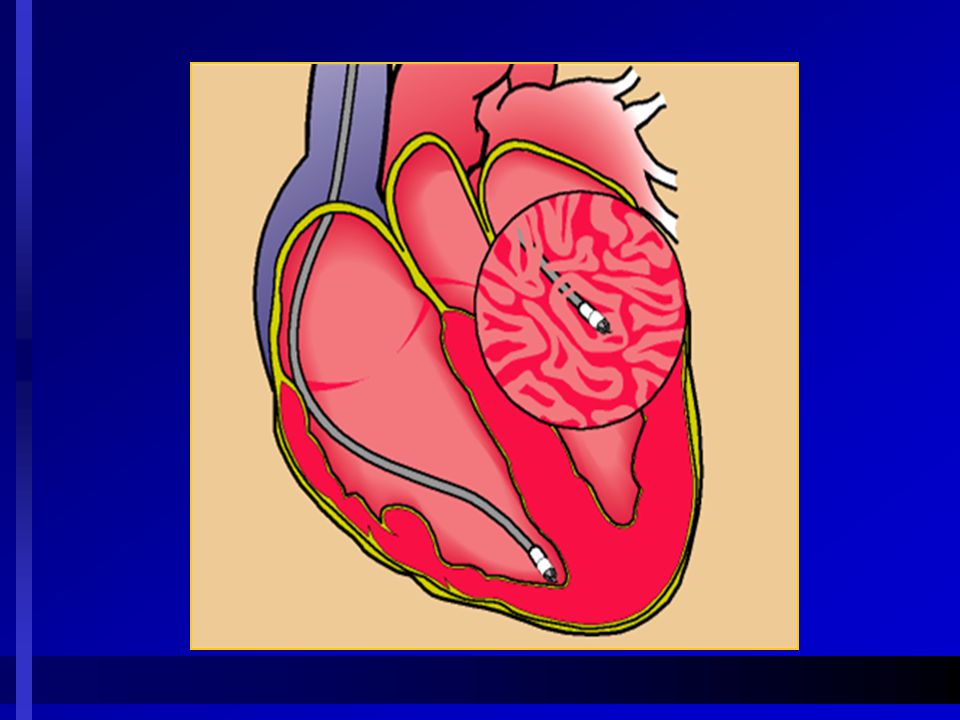
Temporary Epicardial Pacing Temporary pacing leads are invaluable in the diagnosis and treatment of arrhythmia after cardiac surgery. Bipolar leads have been shown to have better pacing and sensing function compared with unipolar leads Atrial leads were implanted directly into the lateral muscular part of right atrium near interatrial groove. Temporary epicardial atrial leads are more effective when placed in the atrial body of right atrium than wrapped within the right atrial appendage Ventricular leads were implanted into the myocardium on the anterior surface of the right ventricle.

26
Biventricular Pacing Indication Adjuvant treatment for patients with heart failure and intraventricular conduction delay Acute hemodynamic improvement is most likely to be observed when QRS duration is greater than 150 ms in patients with left bundle-branch block. Techniques Usually, left ventricular lead implant is accomplished percutaneously through coronary sinus cannulation, advancing the lead into a major cardiac vein. Epicardial lead placement is often a rescue procedure, so it offers advantages related to its safety and shorter implant time.

27
Biventricular Epicardial Pacing Selection of implantation site Selection of the best implantation site was made by echocardiography with tissue Doppler imaging in combination with intraoperative electrophysiologic measurements. Leads were positioned, but not fixed, on several spots of the left ventricular epicardial surface. The final site was chosen on the basis of the longest atrioventricular delay in activation. The target was the posterolateral wall of the left ventricle in most of the patients

28
Early Implantation Complications 1. Surgical Pneumothorax Arterial or venous vascular injury Air embolism Cardiac chamber perforation Lead dislodgment due to inadequate fixation Neural (brachial plexus) injury 2. Wound Hematoma Infection Drainage
 injury 2. Wound Hematoma Infection Drainage.")
29
Late Implantation Complications Surgical 1. Venous thrombosis 2. Pulmonary embolism 3. Constrictive pericarditis ( after asymptomatic perforation) 4. Pulmonary embolism 5. Tricuspid valvular insufficiency Wound 1. Infection 2. Generator migration 3. Skin erosion 4. Device manipulation by patient (Twiddler’s syndrome)
 4. Pulmonary embolism 5. Tricuspid valvular insufficiency Wound 1. Infection 2. Generator migration 3. Skin erosion 4. Device manipulation by patient (Twiddler’s syndrome).")
30
Pacemaker Malfunction (Pacing) 1. Lead position Displacement Microdislodgment Perforation Poor placement at implantation 2. Inadequate device output Power source failure (end of life) Programming error below safety factor Microchip component failure 3. Increased pacing threshold Acute postimplant rise Late fibrotic exit block Myocardial infarction Metabolic, toxic, or electrical influence 4. High resistance in lead system Lead fracture
 Programming error below safety factor Microchip component failure 3. Increased pacing threshold Acute postimplant rise Late fibrotic exit block Myocardial infarction Metabolic, toxic, or electrical influence 4. High resistance in lead system Lead fracture.")
31
Pacemaker Malfunction (Sensing) 1. Skeletal myopotentials Pectoral Abdominal Diaphragmatic 2. Cardiac events T-wave Atrial R-wave sensing Ventricular P-wave sensing Concealed extrasystoles 3. Generator malfunction Programming error-high sensitivity or output Programming error-short refractory period Microchip malfunction 4. Connector malfunction Loose set screw Current leak from header 5. Lead malfunction Conductor fracture Insulation break Polarization potentials 6. Environmental interference Electromagnetic

32
Transvenous Lead Extraction A.Cook transvenous lead extraction system B. Common sites of adhesion

Similar presentations









: Pericardium:>")










