Download presentation
Presentation is loading. Please wait.

1
Leishmaniasis

2
Different stages of Haemoflagellates

3
Causative agent Leishmania genus parasitic protozoa transmitted to human by sandflies. Over 20 species and subspecies infect human, each causing a different spectrum of symptoms.

4
Promastigote Amasitgote
Leishmania life cycle Promastigote Amasitgote Transformation

5
Taxonomy Phylum: Sarcomastigophora Sub-phylum: Mastigophora
Class: Zoomastigophora Order: Kinetoplastida Suborder: Trypanosomatina Family: Trypanosomatidae Genus: Leishmania Subgenous Leishmania Subgenous Viannia

6
Leishmania life cycle Amastigotes replicate in reticuloendothelial cells (mononuclear cells) including; Monocytes Macrophages in lymph nodes, spleen, and lung; Kupffer cells in sinusoids of liver Microglial cells in the central nervous system. Dendritic cells Promastigotes reproduce in biting fly (Phlebotomus, Lutzomyia)
")
8
Leishmania infects and thrives in macrophages
Promastigotes attached to CR1 and CR3 receptors on the macrophages The parasite invades its host cell passively by phagocytosis (parasitophorous vacuole)
")
9
Leishmania sp. amastigote stage
Ovoid small intracellular parasites in a bone marrow aspirate. The typical rod shaped kinetoplast is seen besides the nucleus.(Giemsa stain).
.")
10
Leishmaniasis vectors
There are over 600 species of sand flies divided into five genera. More than 30 species are proved vectors. Phlebotomus in the Old-world and Lutzomia in the New world are vectors of human leishmaniasis.

11
Procyclics and Metacyclic Promastigotes
Amastigotes are released by digestion, transform into procyclic promastigotes and attach to the midgut epithelium Attached promastigotes divide rapidly Metacyclic (infective) promastigotes cease replication, detach and pass forward into the pharynx from where they are regurgitated into the bite site (detached) (attached)
 promastigotes cease replication, detach and pass forward into the pharynx from where they are regurgitated into the bite site. (detached) (attached)")
12
Two subgenera of Leishmania genus
subgenus Leishmania: develops in the sand fly’s midgut and foregut (suprapylorian) Both Old world and New world visceral and cutaneous species subgenus Viannia: develops in the hindgut and midgut (peripylarian). L. braziliensis complex, L. guyanensis complex.
 Both Old world and New world visceral and cutaneous species. subgenus Viannia: develops in the hindgut and midgut (peripylarian). L. braziliensis complex, L. guyanensis complex.")
13
Importance Leishmaniasis is a parasitic disease transmitted by the bite of sand flies. In at least 88 countries. 350 million people at risk. 12 million people are affected by leishmaniasis. 1.5-2 million new cases of cutaneous leishmaniasis estimated to occur annually. new cases of VL which occur annually. 90% of CL cases were from Afghanistan, Algeria, Brazil, Iran, Peru, Saudi Arabia and Syria. 90% of VL cases were from Bangladesh, India, Nepal, Sudan and Brazil. 90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru.

14
Endemic areas for leishmaniasis
Highlighted areas are parts of the world where leishmaniasis has been reported. Taken from British Medical Journal :378

15
The disease main forms Cutaneous leishmaniasis (CL)
2. Visceral leishmaniasis (VL), (kala-azar) is the most severe form of the disease. Mortality rate 75-95% 3. Mucocutaneous leishmaniasis (MCL), or espundia, disfiguring, destruction of mucous membranes of the nose, mouth and throat cavities. Reconstructive surgery of deformities is an important part of therapy
, (kala-azar) is the most severe form of the disease. Mortality rate 75-95% 3. Mucocutaneous leishmaniasis (MCL), or espundia, disfiguring, destruction of mucous membranes of the nose, mouth and throat cavities. Reconstructive surgery of deformities is an important part of therapy.")
16
Cutaneous Leishmaniasis

17
Cutaneous Leishmaniasis
Skin ulcers on the exposed parts of the body such as the face, arms and legs. Old World: L. major, L. tropica, L. aethiopica (DCL) New World: L. mexicana, L. pifanoi, L. amazonensis, L. venezuelensis, L. granhami,
 New World: L. mexicana, L. pifanoi, L. amazonensis, L. venezuelensis, L. granhami,")
18
Cutaneous Leishmaniasis
Characterized by one or more papules, nodules and sores on the skin Sore like a volcano with a raised edge and central crater. Two figures including urban (dry) and rural (wet) forms. Sores are usually painless but can become painful if secondarily infected chronic but self-limiting Some sores are covered by a scab or have not yet ulcerated so they may look like red raised plaques- sometimes with dry crust/scale
 and rural (wet) forms. Sores are usually painless but can become painful if secondarily infected. chronic but self-limiting. Some sores are covered by a scab or have not yet ulcerated so they may look like red raised plaques- sometimes with dry crust/scale.")
19
Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand…) The skin sores will heal by themselves, but this can take months or years. The sores can leave ugly scars.

20
Infection remains restricted to the initial site of infection (the bite site)
")
22
Leishmania tropica Anthroponotic Cutaneous Leishmaniasis (ACL)
Definitive Host: Humans (occasionally dog?) Intermediate Host: Phlebotomus sand flies Main vector and also in Iran: P. Sergenti Dry or urban C.L. Face> hand, leg and… Incubation period: 2-8 months(usually 2-3 months) Lesion persist for several months (more than one year) then person is immune
 Intermediate Host: Phlebotomus sand flies. Main vector and also in Iran: P. Sergenti. Dry or urban C.L. Face> hand, leg and… Incubation period: 2-8 months(usually 2-3 months) Lesion persist for several months (more than one year) then person is immune.")
23
Leishmania tropica First sign: small papule nodule dry sore Itching
Sores don’t heal very quickly Often mistaken for leprosy or tuberculosis First sign: small papule nodule dry sore Itching Scar (if not treated)
")
24
Upper Eyelid. Note the dry, crusted/scabbed appearance which is different than previous sores shown. Photograph provided by COL Naomi Aronson

25
Rarely can cause visceral (viscerotropic) and diffuse cutaneous infections.
 and diffuse cutaneous infections.")
26
Leishmania major Wet or rural form
Definitive Host: rodents (Rodentia: Gerbillidae) as reservoir host, Humans In Iran: Rhombomys opimus, Meriones libycus, M.hurrianae, Tatera indica Zoonotic Cutaneous leishmaniasis (ZCL) Intermediate Host: Phlebotomus sand flies. In Iran: P. papatasi. Incubation period: some weeks to 3 months ( usually 2 weeks) First sign: small papule nodule Wet sore (exudates) Itching Scar (if not treated) Disease period is usually short (2-8 months) More in hands and feet
 as reservoir host, Humans. In Iran: Rhombomys opimus, Meriones libycus, M.hurrianae, Tatera indica. Zoonotic Cutaneous leishmaniasis (ZCL) Intermediate Host: Phlebotomus sand flies. In Iran: P. papatasi. Incubation period: some weeks to 3 months ( usually 2 weeks) First sign: small papule nodule Wet sore (exudates) Itching. Scar (if not treated) Disease period is usually short (2-8 months) More in hands and feet.")
27
Photograph provided by COL Naomi Aronson

28
Both lesions are leishmaniasis
Note the raised border and wet appearance of the sore on the back of the hand. Sores over joints are very concerning as scarring with healing can lead to limited movement of joint. Photograph provided by COL Charles Oster

30
Sporotrichoid form: Dissemination of amastigotes via the lymphatics to the subcutaneous tissues. Regional lymphadenopathy with fever Different cases from Panama and Brazil. The main causative agents were L (V) panamensis and L (V) guyanensis . Old World CL is less commonly associated with sporotrichoid presentation but several cases have been reported from the Middle East . It is very rare in Europe and only a few cases have been reported in Italy.
 panamensis and L (V) guyanensis . Old World CL is less commonly associated with sporotrichoid presentation but several cases have been reported from the Middle East . It is very rare in Europe and only a few cases have been reported in Italy.")
31
Sporotrichoid form Diffuse cutaneous leishmaniasis Recidivans leishmaniasis

32
Cutaneous leishmaniasis differentials
Fungal Bacterial Viral Inflammatory Neoplastic

33
Leprosy It is primarily a granulomatous disease of the peripheral nerves and mucosa of the upper respiratory tract. Skin lesions are the primary external sign. Left untreated, leprosy can be progressive, causing permanent damage to the skin, nerves, limbs and eyes.

34
Lupus volgaris (a sort of cutaneus TB)
Persistent and progressive form of cutaneous TB. Small sharply defined reddish-brown lesions with a gelatinous consistency (called apple-jelly nodules). Lesions persist for years, leading to disfigurement and sometimes skin cancer
. Lesions persist for years, leading to disfigurement and sometimes skin cancer.")
36
New World cutaneous leishmaniasis
L. mexicana (Chicleros Ulcer) External ear L. pifanoi L. amazonensis main cause of DCL All four leishmaniasis forms L. (V.) peruviana (Uta) L. granhami L. venezuelensis
 External ear. L. pifanoi. L. amazonensis. main cause of DCL. All four leishmaniasis forms. L. (V.) peruviana (Uta) L. granhami. L. venezuelensis.")
37
Visceral Leishmaniasis

38
Two children with visceral leishmaniasis
Two children with visceral leishmaniasis. The size of the spleen is marked on the abdomen. Normally the spleen does not protrude below the bottom rib. Photograph provided by COL Charles Oster

39
Systemic infection of reticulo-entdothelial cells (mostly macrophages) throughout multiple internal organs and the blood
 throughout multiple internal organs and the blood")
40
Kala-azar , Visceral Leishmaniasis
L. donovani complex L. donovani (Asia, East Africa) Strain archibaldi L. infantum (Medditeranian basin and Middle East, in children) L. chagasi ( South & Central America) L. tropica (viscerotropic) L. amazonensis Weeks to months (2-6 months) incubation period
 Strain archibaldi. L. infantum (Medditeranian basin and Middle East, in children) L. chagasi ( South & Central America) L. tropica (viscerotropic) L. amazonensis. Weeks to months (2-6 months) incubation period.")
41
L. donovani, anthroponotic
L. infantum, zoonosis, L. donovani ,(archibaldi), zoonosis, L. chagasi, zoonotic
, zoonosis, L. chagasi, zoonotic.")
42
The most sever leishmaniasis form
Mortality of untreated disease 75-95% Prolonged fever (usually dromedary but also continuous, reminant, interminnent) Splenomegaly, hepatomeglay, Weight loss (cachexia), Progressive anemia, pancytopenia, Hypergammaglobulinemia and hypoalbominemia Skin darkness ( around mounth, forehead, temple) Lymphadenopathy may be present Elevated liver enzymes, Nausea, vomiting. Pancytopenia: normochrome & normocytic anemia, trombocytopenia, but lymphocytosis poor feeding,
 Splenomegaly, hepatomeglay, Weight loss (cachexia), Progressive anemia, pancytopenia, Hypergammaglobulinemia and hypoalbominemia. Skin darkness ( around mounth, forehead, temple) Lymphadenopathy may be present. Elevated liver enzymes, Nausea, vomiting. Pancytopenia: normochrome & normocytic anemia, trombocytopenia, but lymphocytosis. poor feeding,")
43
Visceral Leishmaniasis
Visceral leishmaniasis should be considered in every case with chronic fever returning from an endemic area. Malaria, tropical splenomegaly, schistosomiasis, cirrhosis, portal hypertension, trypanosomiasis, milliary tuberculosis, brucellosis, typhoid fever, bacterial endocarditis, histoplasmosis, malnutrition, lymphoma, and leukemia (Singh, 2006). Apart from fly biting, other routes including; Placental, blood transfusion, mechanical, sexual routes. From the Desert Storm experience, would also consider visceral leishmaniasis in patients with low grade elevated temperature, chronically elevated liver function tests and mild anemia Symptoms usually occur months after sandfly biting Because symptoms are non-specific and often start after redeployment there is usually a delay in diagnosis.
. Apart from fly biting, other routes including; Placental, blood transfusion, mechanical, sexual routes. From the Desert Storm experience, would also consider visceral leishmaniasis in patients with low grade elevated temperature, chronically elevated liver function tests and mild anemia. Symptoms usually occur months after sandfly biting. Because symptoms are non-specific and often start after redeployment there is usually a delay in diagnosis.")
44
Post kala-azar dermal leishmaniasis (PKDL)
Sequel of VL which may manifest years after successful treatment and resolution of Kala-azar. Dermal lesions may contain parasites in great numbers. Post Kala-azar Dermal Leishmaniasis (PKDL) has been caused by L. donovani in East Africa and India Pigmentation, red or skin-colored macule, non-ulcerative nodules
 has been caused by L. donovani in East Africa and India. Pigmentation, red or skin-colored macule, non-ulcerative nodules.")
45
Viscerotropic leishmaniasis
L. tropica Oligoparasitic leishmaniasis Fever, fatigue, digestive tract problems First in desert storm operation in Iraq among American soldiers In Iran: One case from AIDS patient (Tehran), other case (Shiraz)
, other case (Shiraz)")
46
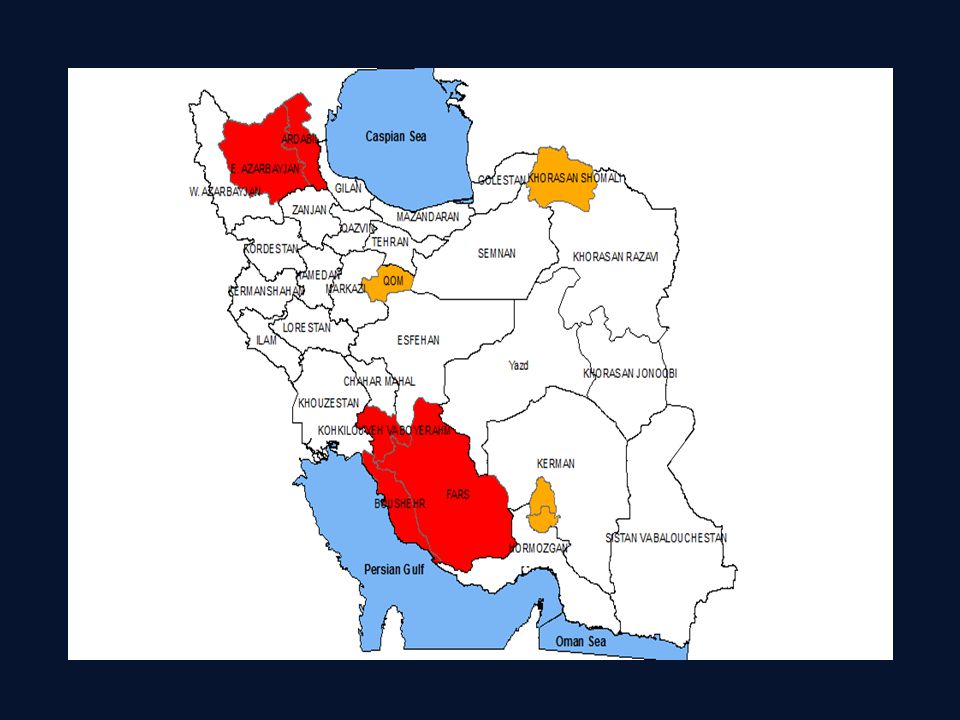
Epidemiology of visceral leishmaniasis in Iran
Mediterranean Kala-azar: - Causative agent is L. infantum - Reservior host: involving canine such as Dog, Jackal, fox, wolf and other wild carnivorouses. - The probable main vector in Iran is Phlebotomus major (Fars), other vectors are P.keshishiani (Fars), P. Perfiliewi (Dashte-Moghan),P. kandelakii (Meshkinshahr). - Age distribution: the disease mainly occurs in children from to 4 years of age.
, other vectors are P.keshishiani (Fars), P. Perfiliewi (Dashte-Moghan),P. kandelakii (Meshkinshahr). - Age distribution: the disease mainly occurs in children from 1 to 4 years of age.")
49
Mucocutaneous Leishmaniasis

50
Espundia or mucocutaenous leishmaniasis

51
Espundia or mucocutaenous leishmaniasis (con.)
May occur months to years after original skin lesion. Lesions can be very disfiguring and destroy all soft parts of the nose and the lips. Death can occurs through secondary bacterial infection. Occurs with Leishmania species from Central and South America Very rarely associated with L. tropica and L. major which are found in the Middle East Hard to confirm diagnosis as few parasites are in the lesion

52
L. (V.) panamensis (ulcer de bejuco)
Three main agents: L. (V.) braziliensis (espundia=MCL) MCL Main causative agent Rodents, occasionally dog and hoarse First self-healing cutaneous After 6 months to years espundia (80% in nasopharynx and nose) L. (V.) panamensis (ulcer de bejuco) MCL second rank agent Sloth, rodent, monkey Along lymphatic vein involves the nasopharynx L. (V.) guyanensis (painbois=CL) Frequent relapse Sloth, Myrmecophagidae Like sporotrichosis (along lymphatic veins)
 braziliensis (espundia=MCL) MCL Main causative agent. Rodents, occasionally dog and hoarse. First self-healing cutaneous. After 6 months to years espundia (80% in nasopharynx and nose) L. (V.) panamensis (ulcer de bejuco) MCL second rank agent. Sloth, rodent, monkey. Along lymphatic vein involves the nasopharynx. L. (V.) guyanensis (painbois=CL) Frequent relapse. Sloth, Myrmecophagidae. Like sporotrichosis (along lymphatic veins)")
55
Immunity TH1: TH2: Macrophage produces IL12 IL12 promote TH0 to TH1
TH1 produces INF gama, IL2, TNF Healing and resistance to disease TH2: TH2 produces IL4, IL5, IL6, IL10, IL13 Sensitivity to disease

56
Diagnosis

57
1. Clinical Diagnosis: Patient history ( endemic region or travel), Signs & symptoms Sores that will not heal, have to be referred for evaluation. Individuals with fevers, weight loss, gastrointestinal complaints, anemia, hypergammaglobulinemia, abnormal liver tests should be referred for evaluation

58
Laboratory Diagnosis of leishmaniasis :
1. Cutaneous Leishmaniasis Tissue sample (scraping, aspirate or punch biopsy) for smear and culture Take scrapings from the sore, put on slides, stain with Wright’s or Giemsa’s stains, and look for amastigotes. Culture (NNN & LIT, Evans, RPMI 1640), Laboratory animals inoculation (Souri andBalb/c mouse) only for L. major (no growth in L. tropica) On occasion, a deep scraping of a skin lesion can be sufficient when the tissue scraping is subjected to giemsa stain, Leishmania culture and/or PCR.
 for smear and culture. Take scrapings from the sore, put on slides, stain with Wright’s or Giemsa’s stains, and look for amastigotes. Culture (NNN & LIT, Evans, RPMI 1640), Laboratory animals inoculation (Souri andBalb/c mouse) only for L. major (no growth in L. tropica) On occasion, a deep scraping of a skin lesion can be sufficient when the tissue scraping is subjected to giemsa stain, Leishmania culture and/or PCR.")
59
Cutaneous Leishmaniasis (con.)
Leishmania skin test (Montenegro test) 0.1 ml (1,000,000 killed L. major promastigote), intradermal, 5mm< induration after 48-72h, DTH Isoenzyme profiles - Zymodemes No serological approaches usually but monoclonal antibodies can be used. DNA hybridisation - PCR
 0.1 ml (1,000,000 killed L. major promastigote), intradermal, 5mm< induration after 48-72h, DTH. Isoenzyme profiles - Zymodemes. No serological approaches usually but monoclonal antibodies can be used. DNA hybridisation - PCR.")
60
2. Visceral Leishmaniasis
Finding Leishmania on biopsy of bone marrow (iliac, sternum, tibia (54-86% sensitivity)), liver (60%), enlarged lymph node (64%), or spleen (98%). Culture (NNN, Evans, LIT) Laboratory animals IP inoculation (Golden hamester) No LST for VL and PKDL diagnosis (Yes for VL and CL epidemiology and MCL and Lupoid diagnosis) Methods available in the US for antibody detection in the serum - IFA test - rk39 dipstick (Kalazar DetectTM)
), liver (60%), enlarged lymph node (64%), or spleen (98%). Culture (NNN, Evans, LIT) Laboratory animals IP inoculation (Golden hamester) No LST for VL and PKDL diagnosis (Yes for VL and CL epidemiology and MCL and Lupoid diagnosis) Methods available in the US for antibody detection in the serum. - IFA test. - rk39 dipstick (Kalazar DetectTM)")
61
Visceral Leishmaniasis (con.)
Serologic tests: Antibody detection: DAT (sen %, spe 72-95%) IFA (sen 55-70, spe 70-89) ELISA,( sen % spe 84-95) Dipstick test (rk39, recombinant antigen 39kd, sen % spe %) DAT is easy, inexpensive, and with high specificity and sensitivity (most usage in Iran) Antigen detection: KAtex (5-20 kd glycoprotein, membranous antigen, easy, field applicable, sen %, spe 100%, positive only in acute disease, useful for HIV/VL ) Formel gel, (Based on hyperimmunoglobulinemia) Multiple myeloma, Schistosomiasis Isoenzyme profiles - Zymodemes Monoclonal antibodies DNA hybridisation – PCR (Schizodem)
 IFA (sen 55-70, spe 70-89) ELISA,( sen % spe 84-95) Dipstick test (rk39, recombinant antigen 39kd, sen % spe %) DAT is easy, inexpensive, and with high specificity and sensitivity (most usage in Iran) Antigen detection: KAtex (5-20 kd glycoprotein, membranous antigen, easy, field applicable, sen %, spe 100%, positive only in acute disease, useful for HIV/VL ) Formel gel, (Based on hyperimmunoglobulinemia) Multiple myeloma, Schistosomiasis. Isoenzyme profiles - Zymodemes. Monoclonal antibodies. DNA hybridisation – PCR (Schizodem)")
64
3. Mucocutaneous Leishmaniasis diagnosis
Early diagnosis and treatment is critical to avoid disfigurement Biopsies should be done but require special training to avoid further disfigurement. Biopsies would be evaluated by the same methods and special laboratories as for cutaneous lesion Because few parasites are present, PCR may be particularly useful

65
Cutaneous and mucocutaneous treatment
Antimony components : Meglumine antimoniate (Glucantime) and Sodium stibogluconate (Pentostam) are drugs of choice. 20 mg/kg/d IV or IM for 20d Pentamidine, Paromomycin are alternative drugs for CL Amphotricine B for antimony resistant MCL Fluconazole may decrease healing time Since L tropica is of more concern in the SWA theatre (because of potential visceralizing infection, rare mucocutaneous involvement, and chronic (recidivans) skin infection) , would not advocate use of azoles routinely as there is not data to support their use in L.tropica and speciation can not be reliably made using clinical appearance. Mucocutaneous infection is treated with a longer treatment course (28 days)
 and Sodium stibogluconate (Pentostam) are drugs of choice. 20 mg/kg/d IV or IM for 20d. Pentamidine, Paromomycin are alternative drugs for CL. Amphotricine B for antimony resistant MCL. Fluconazole may decrease healing time. Since L tropica is of more concern in the SWA theatre (because of potential visceralizing infection, rare mucocutaneous involvement, and chronic (recidivans) skin infection) , would not advocate use of azoles routinely as there is not data to support their use in L.tropica and speciation can not be reliably made using clinical appearance. Mucocutaneous infection is treated with a longer treatment course (28 days)")
66
Visceral leishmaniasis treatment
Pentostam or Glucantime 20 mg /kg/d IV or IM for 28d Amphotricin B: mg/kg IV daily 15-20d Liposomal Amphotricin B (Ambisome): 3 mg/kg/d IV on days 1-5, day 14 and day 21 Low toxicity and high stability, better delivery Alternative: Pentamidine (4mg/kg three times weekly, between 5-25 weeks ), Parmomycine It is not known what species of visceral leishmaniasis is present in Iraq – WHO reports that children have L. infantum. During Desert Storm some of American soldiers were found to have visceral infection with L. tropica. Published studies of liposomal amphotericin for visceral leishmaniasis have not included patients with L. tropica so it is not known for sure that it would be effective but it is expected likely.
: 3 mg/kg/d IV on days 1-5, day 14 and day 21. Low toxicity and high stability, better delivery. Alternative: Pentamidine (4mg/kg three times weekly, between 5-25 weeks ), Parmomycine. It is not known what species of visceral leishmaniasis is present in Iraq – WHO reports that children have L. infantum. During Desert Storm some of American soldiers were found to have visceral infection with L. tropica. Published studies of liposomal amphotericin for visceral leishmaniasis have not included patients with L. tropica so it is not known for sure that it would be effective but it is expected likely.")
67
Visceral leishmaniasis treatment (con.)
Miltefosine (Impavido) (2.5 mg/kg /d p.o. for 28 d) It was developed for cancer therapy at first The only oral drug safer and more tolerable drug (less toxicity for bone marrow and haematopoietic progenitor cells) teratogenic
 (2.5 mg/kg /d p.o. for 28 d) It was developed for cancer therapy at first. The only oral drug. safer and more tolerable drug (less toxicity for bone marrow and haematopoietic progenitor cells) teratogenic.")
69
Leishmaniasis control
Vector control insecticides insecticide impregnated bed nets (IIB) Case finding treatment Aniaml reservoir control Treatment or killing of seropositive dogs Rodent killing Decrease of susceptibility: Childhood age, malnutrition and Immunosuppression are susceptibility factors for VL. eliminating of childhood malnutrition try to produce an efficient vaccine
 Case finding treatment. Aniaml reservoir control. Treatment or killing of seropositive dogs. Rodent killing. Decrease of susceptibility: Childhood age, malnutrition and Immunosuppression are susceptibility factors for VL. eliminating of childhood malnutrition. try to produce an efficient vaccine")
70
0.1 ml in each week for 12 weeks

79
روش نمونه برداری از ضایعات لیشمانیوز پوستی
کناره های ملتهب و متورم ضایعات پوستی(لبه خارجی زخم) بیشترین میزان آمستیگوت را دارد. هر چه بافت بیشتر شانس یافتن آمستیگوت بیشتر تمیز کردن محل زخم با پنبه و الکل 70%، با توجه به عفونت باکتریایی و قارچی بر روی ضایعه سالک خشک شدن الکل قبل از نمونه برداری محل نمونه برداری توسط انگشت شصت و سبابه محکم گرفته شود. توسط تیغه اسکالپل نوک باریک و یا لانست استریل شکافی به عمق یک میلی متر در ناحیه ای که توسط دو انگشت گرفته شده ایجاد می شود. از عمق محل شکافته شده خراشهایی به سمت سطح و مرکز ضایعه جهت برداشت نمونه داده می شود.
 بیشترین میزان آمستیگوت را دارد. هر چه بافت بیشتر شانس یافتن آمستیگوت بیشتر. تمیز کردن محل زخم با پنبه و الکل 70%، با توجه به عفونت باکتریایی و قارچی بر روی ضایعه سالک. خشک شدن الکل قبل از نمونه برداری. محل نمونه برداری توسط انگشت شصت و سبابه محکم گرفته شود. توسط تیغه اسکالپل نوک باریک و یا لانست استریل شکافی به عمق یک میلی متر در ناحیه ای که توسط دو انگشت گرفته شده ایجاد می شود. از عمق محل شکافته شده خراشهایی به سمت سطح و مرکز ضایعه جهت برداشت نمونه داده می شود.")
80
ادامه روش نمونه برداری از ضایعات لیشمانیوز پوستی
نوک تیغه اسکالپل را خارج و از مواد برداشت شده 3 اسمیر گرفته می شود و با قلم الماس شماره نمونه یا اسم بیمار بر روی لام شیشه ای ثبت شود. در صورت نیاز به کشت، در کنار شعله نمونه ( بر روی تیغه اسکالپل) به درون محیط کشت دایفازیک منتقل می شود.
 به درون محیط کشت دایفازیک منتقل می شود.")
81
رنگ آمیزی گیمسا محلول تجارتی غلیظ (و متفاوت)
پس از رقیق سازی بتواند گلبول سفید را به خوبی رنگ کند. اسلاید حاوی نمونه بدون شعله ودر دمای اتاق خشک شوند. متانول Methanol 70% متانول خشک شود (اصطلاحا بپرد) بسته به دستور تولید کننده مثلا 1 به 30 یا 1 به 50 رنگ رقیق شود. آبی که جهت رقیق کردن استفاده می شود جهت pH تنظیم شده باشد. بسته به رقت و نوع آن مدت رنگ آمیزی دقیقه است که به طور تجربی بدست می آید. مشاهده با عدسی شیئی 10 و سپس 40 و سپس 100 (با روغن ایمرسیون) ومستقیما بدون لامل حداقل جستجوی 30 شان و یافتن ماکروفاژها در هر کدام از 3 لام نبود ماکروفاژ و فراوانی گلبول قرمز نشانه نمونه نامناسب inadequate)) و ضرورت نمونه گیری مجدد
 بسته به دستور تولید کننده مثلا 1 به 30 یا 1 به 50 رنگ رقیق شود. آبی که جهت رقیق کردن استفاده می شود جهت7.2 pH تنظیم شده باشد. بسته به رقت و نوع آن مدت رنگ آمیزی دقیقه است که به طور تجربی بدست می آید. مشاهده با عدسی شیئی 10 و سپس 40 و سپس 100 (با روغن ایمرسیون) ومستقیما بدون لامل. حداقل جستجوی 30 شان و یافتن ماکروفاژها در هر کدام از 3 لام. نبود ماکروفاژ و فراوانی گلبول قرمز نشانه نمونه نامناسب inadequate)) و ضرورت نمونه گیری مجدد.")
82
ایزولاسیون کشت در محیط NNN
Novy, Macneal, Nicolle آگار 14 گرم NaCl 6 گرم آب مقطر cc 900 حرارت (جوشاندن) تا شفاف شدن ( ولی احتیاط جهت سر ریز نشدن) اتو کلاو و سپس سرد شدن تا حرارت درجه اضافه کردن گلوکز 30گرم در صد به میزان 5 درصد اضافه کردن خون خرگوش دفیبرینه درصد حجم محلول به صورت گرم، تقسیم در لوله های استریل درپیچ دار (3 میلی لیتر)، قرار دادن به شکل slant انتقال به یخچال پس از بستن آگار در هنگام استفاده، اضافه کردن 0.5 تا 1 سی سی PBS یا RPMI به عنوان فاز مایع
 تا شفاف شدن ( ولی احتیاط جهت سر ریز نشدن) اتو کلاو و سپس سرد شدن تا حرارت درجه. اضافه کردن گلوکز 30گرم در صد به میزان 5 درصد. اضافه کردن خون خرگوش دفیبرینه درصد حجم محلول. به صورت گرم، تقسیم در لوله های استریل درپیچ دار (3 میلی لیتر)، قرار دادن به شکل slant. انتقال به یخچال پس از بستن آگار. در هنگام استفاده، اضافه کردن 0.5 تا 1 سی سی PBS یا RPMI به عنوان فاز مایع.")
83
ادامه کشت نمونه بیوپسی پوستی، آسپیراسیون مغز استخوان و خون
2 میلی متر در عمق پایین ترین سطح شیب دار اینکوباسیون در درجه سانتیگراد انگل در فاز مایع رشد کرده و یافت خواهد شد. استریل کار کردن: باکتری و قارچ مانع رشد انگل هستند. بررسی کشت جهت جستجوی انگل: هفته ای یکبار و تا یکماه ( عدم رشد معادل منفی بودن است). اگر انگل دیر رشد باشد زمان بیشتری را نیاز دارد.
. اگر انگل دیر رشد باشد زمان بیشتری را نیاز دارد.")
84
Leishmaniasis Control
WHO interest African trypanosomiasis>Dengo>Leishmaniasis>Malaria>Schistosomiasis>Lymphatic filiriasis> Chagas Close contact of humans and their domestic animals can provide optimal conditions for sand flies and Leishmania transmission (stables provide good breeding ground for larvae) In urban environments infection is mostly human to human In rural areas Leishmaniasis can be a zoonosis Infection in dogs is quite frequent in the Mediterranean
 In urban environments infection is mostly human to human. In rural areas Leishmaniasis can be a zoonosis. Infection in dogs is quite frequent in the Mediterranean.")
85
Ecology of new world leishmaniasis
In the new world most people get infected while working or hunting in the forest Here wild animals including rodents, monkeys and sloths provide a reservoir for the parasite A transmission pattern within a population of wild animals that result in occasional infection of humans is called sylvatic

86
In sand fly, amastigotes are surrounded by a peritrophic membrane (PM), a chitin lattice embedded in protein carbohydrate matrix secreted by the epithelium of midgut. Round amastigotes transform to short ellipsoid procyclic promastigotes (6-8mm length). Procyclic promastigotes multiplicate within PM but gradually transform to nectomonad form when divide (in a more elongated form with μm body length). Nectomonades migrate from posterior midgut to anterior part and then into thoracic midgut and cardiac valve. After PM disintegration, some nectomonades attach to midgut epithelium particularly in the thoracic midgut in the vicinity of cardiac valve, inserting their flagella between the microvilli and then transform to haptomonad (5-8µm broad, shorter cells). From day five post feeding, metacyclic infective promastigotes can be observed in lumen (in a detached position). metacyclic promastigote are injected through the food channel in the sand fly proboscis.
. Procyclic promastigotes multiplicate within PM but gradually transform to nectomonad form when divide (in a more elongated form with μm body length). Nectomonades migrate from posterior midgut to anterior part and then into thoracic midgut and cardiac valve. After PM disintegration, some nectomonades attach to midgut epithelium particularly in the thoracic midgut in the vicinity of cardiac valve, inserting their flagella between the microvilli and then transform to haptomonad (5-8µm broad, shorter cells). From day five post feeding, metacyclic infective promastigotes can be observed in lumen (in a detached position). metacyclic promastigote are injected through the food channel in the sand fly proboscis.")
87
Cutaneous Leishmaniasis in Birjand
It is estimated that in recent years an endemic zone of CL has been emerged in Birjand area. In our study, among 80 Giemsa stained smears of CL patients in Birjand which identified by PCR methods, 8 (10%) had Leishmania major and 72 others infected by Leishmania tropica. So both Zoonotic and Anthroponotic cutaneous leishmaniais are endemic in this region.
 had Leishmania major and 72 others infected by Leishmania tropica. So both Zoonotic and Anthroponotic cutaneous leishmaniais are endemic in this region.")
88
Cutaneous Leishmaniasis is usually self-limiting
A chronic but self-limiting dry ulceration at the site of the bite Parasites are not found outside the lesion Nearly absolute resistance to reinfection Inoculation to vaccinate has long been practiced in the middle east

89
Sporotrichoid form: dissemination of amastigotes via the lymphatics to the subcutaneous tissues. Regional lymphadenopathy with fever Different cases from Panama and Brazil. The main causative agents were L (V) panamensis and L (V) guyanensis (Herwaldt, 1999; Melby et al.1992). Old World cutaneous leishmaniasis is less commonly associated with sporotrichoid presentation but several cases have been reported from the Middle East (Kibbi et al. 1987; Ayattolahi, 2006). It is very rare in Europe and only a few cases have been reported in Italy.
 panamensis and L (V) guyanensis (Herwaldt, 1999; Melby et al.1992). Old World cutaneous leishmaniasis is less commonly associated with sporotrichoid presentation but several cases have been reported from the Middle East (Kibbi et al. 1987; Ayattolahi, 2006). It is very rare in Europe and only a few cases have been reported in Italy.")
90
Cutaneous leishmaniasis differentials
Fungal –Paracoccidioidomycosis, chromoblastomycosis, sporotrichosis, blastomycosis Bacterial – Staphylococcal and streptococcal infections, pinta, yaws, syphilis, tuberculosis, leprosy, cutaneous diphtheria, tularemia, tropical pyoderma, and other mycobacterioses Viral -OrfOrf is an exanthemous disease caused by a parapox virus and occurring primarily in sheep and goats. It is also known as contagious pustular dermatitis, infectious labial dermatitis, ecthyma contagiosum, thistle disease[1] and scabby mouth. Orf virus is zoonotic - it can also infect humans.[1] Inflammatory - Sarcoidosis, pyogenic granuloma, lupus Neoplastic - Cutaneous T-cell lymphoma, basal cell carcinoma, squamous cell carcinoma, metastases, Psoriasis, Keloids

91
peritrophic membrane (PM), a chitin lattice embedded in protein carbohydrate matrix secreted by the epithelium of midgut. Round amastigotes transform to short ellipsoid multiplicating procyclic promastigotes (6-8mm length). Procyclic promastigotes gradually transform to nectomonad form when divide (in a more elongated form with μm body length). Nectomonades migrate from posterior midgut to anterior part and then into thoracic midgut and cardiac valve. Nectomonades attach to midgut epithelium particularly in the thoracic midgut in the vicinity of cardiac valve, inserting their flagella between the microvilli and then transform to haptomonad (5-8µm broad, shorter cells). From day five post feeding, metacyclic infective promastigotes can be observed in lumen (in a detached position). metacyclic promastigote are injected through the food channel in the sand fly proboscis.
. Procyclic promastigotes gradually transform to nectomonad form when divide (in a more elongated form with μm body length). Nectomonades migrate from posterior midgut to anterior part and then into thoracic midgut and cardiac valve. Nectomonades attach to midgut epithelium particularly in the thoracic midgut in the vicinity of cardiac valve, inserting their flagella between the microvilli and then transform to haptomonad (5-8µm broad, shorter cells). From day five post feeding, metacyclic infective promastigotes can be observed in lumen (in a detached position). metacyclic promastigote are injected through the food channel in the sand fly proboscis.")
92
Zymodem Serodem Schizodem

93
Animal leishmania that occatinally transmitted to human
L. inerity (guinapig): linear kinetoplast, large cytoplasmic vacule, metastatic property L. adlery, L. agame, L. gimnodactily (خزندگان L. turanica, L. gerbili, L, arabica (rodents) L. daini ( the biggest Leishmania amastigote), L. hertigi ( خارپشت)
: linear kinetoplast, large cytoplasmic vacule, metastatic property. L. adlery, L. agame, L. gimnodactily (خزندگان. L. turanica, L. gerbili, L, arabica (rodents) L. daini ( the biggest Leishmania amastigote), L. hertigi ( خارپشت)")
94
Rizhoplast Longitudinal binary fission Infective Metacyclic ( in stationary phase) Sandfly peptides in بزاق : increase severity, inhibit complement, vasodilant, anti-coagulant
 Sandfly peptides in بزاق : increase severity, inhibit complement, vasodilant, anti-coagulant")
95
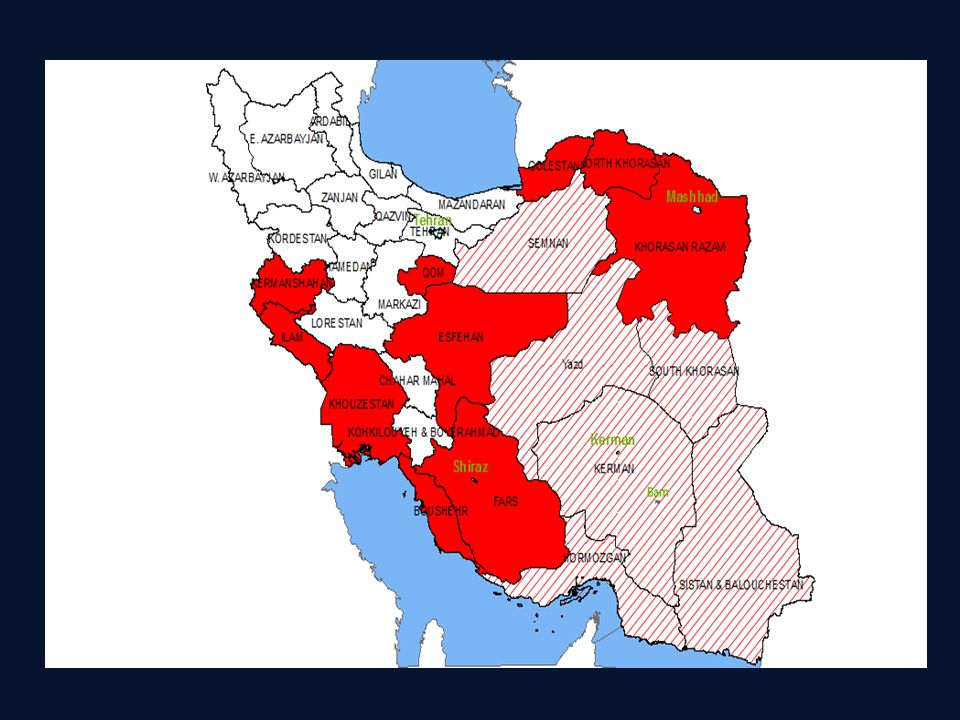
Iran: Bam, Shiraz, Kerman, Tehran, Mashhad, Sabzevar, Neishaboor
L. tropica in world: P. sergenti P. cocasicus Iran: Bam, Shiraz, Kerman, Tehran, Mashhad, Sabzevar, Neishaboor In all seasons

96
In last summer month and first fall
L. major In world: P. papatasi, P. lonipes, P. cocacicus, P. Ansari In Iran: Rhombomys opimus ( central;Isfahan, Fars, northeast: khorasan), Meriones libycus (Yazd), M.hurrianae (southest: sistan & Bloochestan), Tatera indica, Nosekia indica (west: khozestan) In last summer month and first fall
, Meriones libycus (Yazd), M.hurrianae (southest: sistan & Bloochestan), Tatera indica, Nosekia indica (west: khozestan) In last summer month and first fall.")
97
LST is positive in: cured VL, MCL, last ACL phase (recidivans)
L. aethiopica P. Pedifer Hyrax Due to immune deficecy in second signall (B71(CD80) and B72(CD86) in CMI Anergy No response to treatment LST is negative in: DCL, VL, PKDL, early phase of urban CL LST is positive in: cured VL, MCL, last ACL phase (recidivans)
 and B72(CD86) in CMI. Anergy. No response to treatment. LST is negative in: DCL, VL, PKDL, early phase of urban CL. LST is positive in: cured VL, MCL, last ACL phase (recidivans)")
98
ZCL sorts Tardy exuicerating Acute necrotizing Abortive Erysipdoid
Horn Exematoid Verueoid Tamral sprotrichoid

99
Aconitate hydratase diffrentiate leishmania subgenus from viannia

100
New World cutaneous leishmaniasis
L. mexicana (Chicleros Ulcer) External ear Rodent, human CL and DCL L. pifanoi (DCL) DCL like L. aethiopica L. amazonensis main cause of DCL Not kealing DCL in AIDS All four leishmaniasis forms Rodent, Oposum, Fox L. (V.) peruviana (Uta) Like L. tropica self-healing lesion Probably originated from L. tropica but differe in zymodem. Reservoir :Dog, and probably a redont L. granhami L. venezuelensis
 External ear. Rodent, human. CL and DCL. L. pifanoi (DCL) DCL like L. aethiopica. L. amazonensis. main cause of DCL. Not kealing DCL in AIDS. All four leishmaniasis forms. Rodent, Oposum, Fox. L. (V.) peruviana (Uta) Like L. tropica self-healing lesion. Probably originated from L. tropica but differe in zymodem. Reservoir :Dog, and probably a redont. L. granhami. L. venezuelensis.")
101
L. chagasi (similar zymodem and schizodem pattern with L. infantum)
American kala-azar: L. chagasi (similar zymodem and schizodem pattern with L. infantum) Dogs and fox L. longipalpis Indian kala-azar anthroponotic P. argantipes 5-9 years PKDL in 20% of cases 6 months after healing Loaded amastigotes A good source for sandfly Butterfly distribution on face (like lupus) No systematic manifestation such as fever and splenomegaly
 Dogs and fox. L. longipalpis. Indian kala-azar. anthroponotic. P. argantipes. 5-9 years. PKDL in 20% of cases 6 months after healing. Loaded amastigotes. A good source for sandfly. Butterfly distribution on face (like lupus) No systematic manifestation such as fever and splenomegaly.")
102
Medditereanian kala-azar
Middle east and Meditteranian basin 1-4 years children Canidea P. major, P. longicuspis, P, chinensis, P. perfiliewi, P. kandelakii, P. ariasi, P. perniciosus

103
G6PD enzyme can differentiate L. guyanensis from L. panamensis
L. laiensoi Agoti L. colombiensis sloth

104
L. (V.) panamensis (Ulcer de bejuco)
Three main agents: L. (V.) braziliensis (Espundia=MCL) MCL Main causative agent Rodents, occasionally dog and hoarse First self-healing cutaneous After 6 months to years Espundia (80% in nasopharynx and nose) Fastidious growth in culture Reflecting bodies L. (V.) panamensis (Ulcer de bejuco) MCL second rank agent Sloth, rodent, monkey Along lymphatic vein involves the nasopharynx Sandfly: Luteromia, psycodopigus Easily growthable in culture media L. (V.) guyanensis (Painbois=CL) Frequent relapse Metastatic Sloth, مورچه خوار Like sporotrichoid (along lymphatic veins)
 braziliensis (Espundia=MCL) MCL Main causative agent. Rodents, occasionally dog and hoarse. First self-healing cutaneous. After 6 months to years Espundia (80% in nasopharynx and nose) Fastidious growth in culture. Reflecting bodies. L. (V.) panamensis (Ulcer de bejuco) MCL second rank agent. Sloth, rodent, monkey. Along lymphatic vein involves the nasopharynx. Sandfly: Luteromia, psycodopigus. Easily growthable in culture media. L. (V.) guyanensis (Painbois=CL) Frequent relapse. Metastatic. Sloth, مورچه خوار. Like sporotrichoid (along lymphatic veins)")
105
GP63 Major surface protein, metaloprotease (Zn)
Hb degradation and role in promastigote methabolism Resistance against lysosome function in macrophage phagolyzozome Role in attachment of parasite to macrophage receptors CR1 (CD35) and CR3 (CD11blCD18) Degradation of collagen and fibronectin
 and CR3 (CD11blCD18) Degradation of collagen and fibronectin.")
106
LPG 25% of promastigote weight
Role in attachment of parasite to macrophage receptors Proteinase C inhibition Phagosome-lysosome attachment inhibition Protection against tripsin enzyme in sandfly midgut Role in glycocalex production and protection against lysosome

107
Glycosyl phospatidyl inositol
Glycocalyx conformation Resistance against lysosome in phagolysosome

108
Biohasic media Monophasic media NNN LIT Evans HOMEM RPMI1640 Graces
Schneider drosophila

109
Leishmania and Trypanosoma
From the seven genera in the Trypanosomatidae family, only 2 genera, Leishmania and Trypanosoma, are important parasites of humans. Not all parasites in the family possess all the four morphological forms: Leishmania spp. - possesses only amastigote & promastigote forms Trypanosoma brucei - has only epimastigote & trypomastigote Trypanosoma cruzi - has all four forms

110
P.o. =per os= by oral route

112
Cutaneous and mucocutaneous treatment
Antimony components : Meglumine antimoniate (Glucantime) and Sodium stibogluconate (Pentostam) are drugs of choice. 20 mg per kg, daily IV or IM for 20d Pentamidine, Paromomycin are alternative drugs for CL Amphotricine B for antimony resistant MCL Fluconazole may decrease healing time in L. major infection Since L tropica is of more concern in the SWA theatre (because of potential visceralizing infection, rare mucocutaneous involvement, and chronic (recidivans) skin infection) , would not advocate use of azoles routinely as there is not data to support their use in L.tropica and speciation can not be reliably made using clinical appearance. Mucocutaneous infection is treated with a longer treatment course (28 days)
 and Sodium stibogluconate (Pentostam) are drugs of choice. 20 mg per kg, daily IV or IM for 20d. Pentamidine, Paromomycin are alternative drugs for CL. Amphotricine B for antimony resistant MCL. Fluconazole may decrease healing time in L. major infection. Since L tropica is of more concern in the SWA theatre (because of potential visceralizing infection, rare mucocutaneous involvement, and chronic (recidivans) skin infection) , would not advocate use of azoles routinely as there is not data to support their use in L.tropica and speciation can not be reliably made using clinical appearance. Mucocutaneous infection is treated with a longer treatment course (28 days)")
113
Leishmaniasis Control
WHO interest African trypanosomiasis>Dengo>Leishmaniasis>Malaria>Schistosomiasis>Lymphatic filiriasis> Chagas Close contact of humans and their domestic animals can provide optimal conditions for sand flies and Leishmania transmission (stables provide good breeding ground for larvae) In urban environments infection is mostly human to human In rural areas Leishmaniasis can be a zoonosis Infection in dogs is quite frequent in the Mediterranean
 In urban environments infection is mostly human to human. In rural areas Leishmaniasis can be a zoonosis. Infection in dogs is quite frequent in the Mediterranean.")
114
Ecology of new world leishmaniasis
In the new world most people get infected while working or hunting in the forest Here wild animals including rodents, monkeys and sloths provide a reservoir for the parasite A transmission pattern within a population of wild animals that result in occasional infection of humans is called sylvatic

115
reaction is seen in people with previous contact to the antigen who have developed cellular immunity. Conversion occurs after several weeks in CL, and in VL usually only after treatment and cure (Peters and Killick-Kendrick, 1987). Present and past infections can not be differentiated. The Montenegro skin test is occasionally used in diagnosis of cutaneous disease (eg, in epidemiological surveys), because of its simple use and high sensitivity and specifi city;118 however, it fails to distinguish between past and present infections. Pentavalent antimonial drugs Pentavalent antimony has been drug of choice for all forms of leishmaniasis such as visceral leishmaniasis. Two of the most important drugs of this class are Sodium stibogluconate and Meglumine antimoniate. Toxicity and parenteral administration make them not ideal. Some side effects with the spectrum from arthralgias and ache to chemical pancreatitis have been observed (Roscoe, 2005). In India and some other regions, resistance to these drugs is a rising problem (Bhattacharyya et al. 2002). Administration dosage of them is 20mg/kg/day for 28 days in case of VL and for 20 days in case of CL (Herwaldt, 1999
, because of its simple use and high sensitivity and specifi city;118 however, it fails to distinguish between past and present infections. Pentavalent antimonial drugs. Pentavalent antimony has been drug of choice for all forms of leishmaniasis such as visceral leishmaniasis. Two of the most important drugs of this class are Sodium stibogluconate and Meglumine antimoniate. Toxicity and parenteral administration make them not ideal. Some side effects with the spectrum from arthralgias and ache to chemical pancreatitis have been observed (Roscoe, 2005). In India and some other regions, resistance to these drugs is a rising problem (Bhattacharyya et al. 2002). Administration dosage of them is 20mg/kg/day for 28 days in case of VL and for 20 days in case of CL (Herwaldt,")
Similar presentations





















>")

>")





 Leishmania form Rounded shape, absence of free flagellum,>")


, contain only two genera that parasitize.>")
 (VL) Leishmania tropica (CL) Leishmania major (CL) Leishmania aethiopica (CL) Leishmania mexicana (Complex)>")



. caused by intracellular protozoan parasites of the genus Leishmania transmitted by phlebotomine sandflies disease involving.>")