Download presentation
Presentation is loading. Please wait.

2
1. Leishmaniasis is a disease caused by an intracellular protozoa parasite. 2. parasitesusceptibility, such as HIV infection and malnutrition. 3. is transmitted by the bite of a sandfly, which is usually one half to one third the size of a mosquito.

4
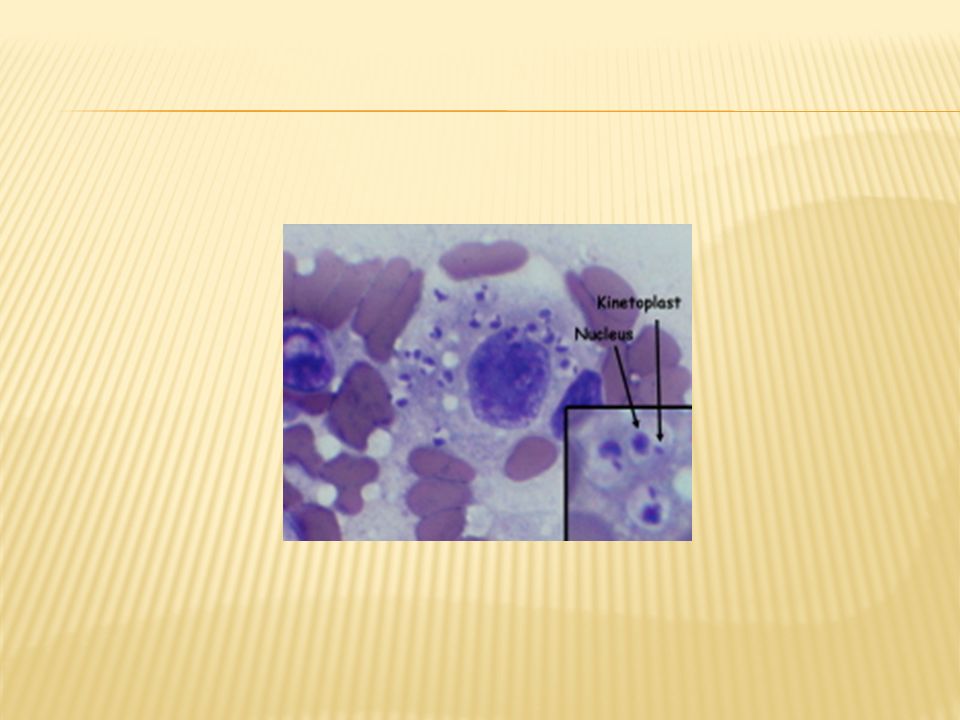
In mammalian hosts, the organism exists as a nonflagellated amastigote composed of a large nucleus and a kinetoplast, with an absent or greatly reduced flagellum, that resides in the phagolysosome of the macrophage. The vector is the sandfly, of the genus Phlebotomus in the Old World and of the genus Lutzomyia in the New World.

5
promastigotes enter into or are ingested by the new host's macrophages, where they transform back into amastigotes, multiply, and eventually spread throughout the reticuloendothelial system. Clinical disease becomes apparent within weeks to months after infection.

6
At one extreme, localized cutaneous disease demonstrates a vigorous immune response, with most cases resolving without intervention. This form of the disease exhibits a helper T-cell subtype 1 immune response, with interleukin 2, interferon-gamma, and interleukin 12 as the prominent cytokines that induce disease resolution.

7
At the other extreme, with visceral or diffuse cutaneous disease, patients exhibit relative anergy to the Leishmania organism and have a prominent helper T-cell subtype 2 cytokine profile.

8
Clinical disease: The 3 primary clinical forms of leishmaniasis are cutaneous, mucocutaneous, and visceral disease. Cutaneous leishmaniasis can be further divided into localized, diffuse cutaneous, recidivans, and post–kala azar dermal leishmaniasis.

9
Geographic occurrence: Old World leishmaniasis is caused by Leishmania species found in Africa, Asia, the Middle East, the Mediterranean, and India, and it produces cutaneous or visceral disease. New World leishmaniasis is caused by Leishmania species found in Central America and South America, and it produces cutaneous, mucocutaneous, and visceral disease.

10
Localized cutaneous leishmaniasis: Crusted papules or ulcers occur several weeks to months (in rare cases) after sandfly bite inoculation on exposed skin. Lesions may be associated with sporotrichotic spread and usually heal spontaneously.

11
Diffuse cutaneous leishmaniasis: Analogous to lepromatous leprosy, individuals with diffuse cutaneous leishmaniasis cannot mount a cell- mediated immune response to the Leishmania parasite. Multiple, widespread cutaneous papules and nodules, and they are anergic to leishmanin skin testing.

12
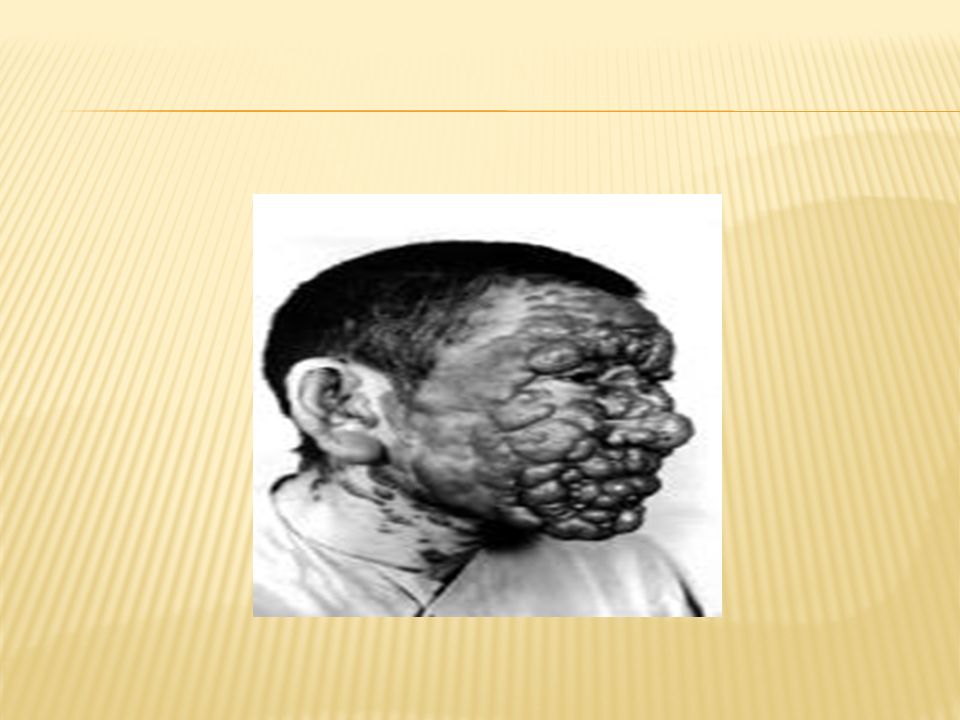
Recidivans cutaneous leishmaniasis: A relatively uncommon clinical variant of leishmaniasis. Recidivans cutaneous leishmaniasis appears as a recurrence of lesions at the site of apparently healed disease years after the original infection. Typically occur on the face. Enlarging papule, plaque, or coalescence of papules that heals with central scarring. Relentless expansion at the periphery may cause significant facial destruction similar to the lupus vulgaris variant of cutaneous tuberculosis.cutaneous tuberculosis

13
Post–kala azar dermal leishmaniasis Develops months to years after the patient's recovery from visceral leishmaniasis. Cutaneous lesions demonstrate great variability, ranging from hypopigmented macules to erythematous papules and from nodules to plaques. Lesions may be numerous and persist for decades. Isolated parasites from the lesions are identical to those that cause the original visceral disease.

14
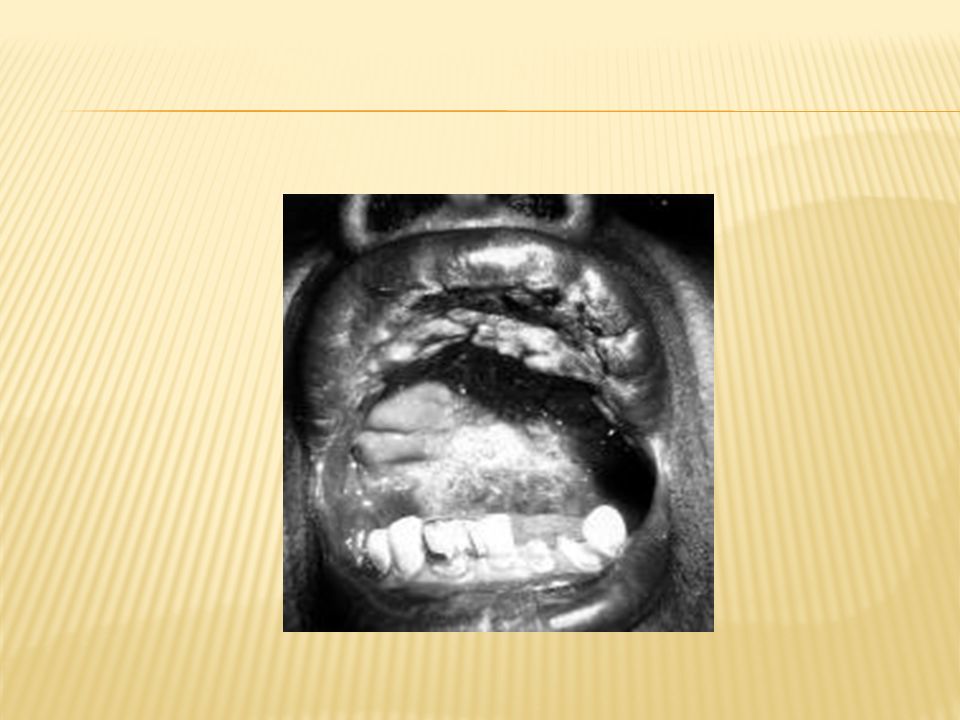
Mucocutaneous leishmaniasis: Predominantly a New World disease, this form of leishmaniasis may not manifest clinically until years after localized cutaneous disease apparently has healed. In a poorly understood manner, certain species of Leishmania migrate to the upper respiratory tract, where relentless destruction of the oropharynx and nose ensues. Gradually, the migration results in extensive midfacial destruction and, occasionally, in death.

15
Visceral leishmaniasis (kala azar): Leishmania parasites localize to the reticuloendothelial system, rather than to the skin, and produce a potentially lethal widespread systemic disease.
: Leishmania parasites localize to the reticuloendothelial system, rather than to the skin, and produce a potentially lethal widespread systemic disease.")
16
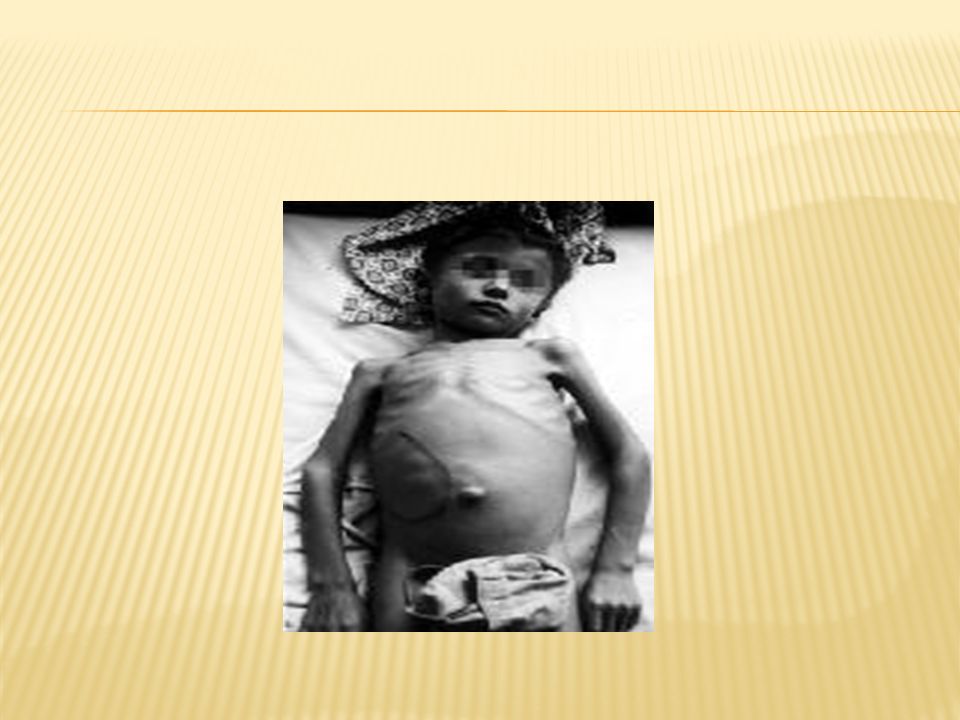
Symptoms of visceral leishmaniasis can be confused with many other infectious diseases; however, in endemic areas, the typical patient has wasting and presents with massive splenomegaly, pancytopenia, hypergammaglobulinemia, and intermittent fevers (although they are less acutely ill than patients with malaria).
.")
17
A typical lesion of localized cutaneous leishmaniasis begins as an inflammatory papule, which later progresses to an ulcer. This may be associated with sporotrichotic lymphatic spread. In the vast majority of cases, the ulcers heal spontaneously with scarring.

21
Patients with diffuse cutaneous leishmaniasis develop hundreds of papules, nodules, and plaques throughout the skin in a clinical picture that can be reminiscent of lepromatous leprosy. This form of leishmaniasis often is resistant to therapy and may assume a chronic course.

23
In recidivans cutaneous leishmaniasis, typically, psoriasiform plaques occur on the face and progress centrifugally, bearing a striking resemblance to lupus vulgaris. Similar to disseminated disease, recidivans cutaneous leishmaniasis may be resistant to therapy and result in a disfiguring clinical picture

26
In post–kala azar dermal leishmaniasis, cutaneous lesions are polymorphous, ranging from hypopigmented or erythematous macules to papules and nodules that may coalesce.

29
The hallmarks of visceral leishmaniasis are fever, malaise, hepatosplenomegaly, anorexia, wasting, pancytopenia, and hypergammaglobulinemia. Occasionally, the skin becomes severely xerotic and hyperpigmented because of melanocyte stimulation. This form of leishmaniasis frequently is lethal if not treated.

31
Localized cutaneous leishmaniasis Old World -Leishmania major, Leishmania tropicaNew World – L mexicana New World – L mexicana Recidivans cutaneous leishmaniasis Old World – L tropica New World – L braziliensis

32
The differential diagnosis of localized cutaneous leishmaniasis is extensive and includes impetigo, pyoderma gangrenosum, deep fungal infection, mycobacterial infection, sarcoidosis, and squamous cell carcinoma.impetigopyoderma gangrenosum sarcoidosissquamous cell carcinoma Recidivans cutaneous leishmaniasis may mimic cutaneous tuberculosis (lupus vulgaris, tuberculosis verrucosa cutis), psoriasis, deep fungal infection, or nummular dermatitis.psoriasisnummular dermatitis
, psoriasis, deep fungal infection, or nummular dermatitis.psoriasisnummular dermatitis")
33
Mucocutaneous leishmaniasis may simulate paracoccidioidomycosis, histoplasmosis, syphilis, yaws, rhinoscleroma, squamous cell carcinoma, and midline granuloma of the face.histoplasmosis syphilisyawsrhinoscleroma

34
Visceral leishmaniasis may be confused with a variety of other infectious diseases or febrile systemic illnesses, including schistosomiasis, malaria, tropical splenomegaly syndrome, histoplasmosis, malnutrition, typhoid fever, brucellosis, miliary tuberculosis, lymphoma, leukemia, African trypanosomiasis, and bacterial endocarditis.schistosomiasis malariatyphoid fever brucellosismiliary tuberculosisAfrican trypanosomiasis bacterial endocarditis

35
Skin scrapings can be obtained from the base of an active ulcer, or a 4-mm biopsy specimen can be obtained from the edge of a suggestive lesion or ulcer. The parasite consists of a nucleus and a kinetoplast surrounded by a cell wall. Visualization of all 3 features (ie, nucleus, cell membrane, and kinetoplast) is required to make a diagnosis based on microscopy findings.
 is required to make a diagnosis based on microscopy findings..")
36
Diagnosis is usually much easier using Giemsa- stained touch preparations. Diagnosis is usually much easier using Giemsa- stained touch preparations.The diagnostic sensitivity of microscopic identification of leishmanial amastigotes is typically 75-85%.

38
Polymerase chain reaction (PCR) is now routinely used in experienced laboratories as a rapid diagnostic technique. Visceral leishmaniasis has been diagnosed for a very long time using the same methodology described above for cutaneous lesions but applied to either splenic, hepatic, or bone marrow aspirates.

39
Similar to the purified protein derivative testing (PPD for Mycobacterium tuberculosis), Montenegro leishmanin skin testing (LST) has been used for decades to determine previous or current exposure to Leishmania parasites.
, Montenegro leishmanin skin testing (LST) has been used for decades to determine previous or current exposure to Leishmania parasites.")
40
local therapies for some forms of cutaneous leishmaniasis include (1) cryotherapy, (2) infiltration of sodium stibogluconate at 0.3-0.8 mL, (3) local heat therapy at 40-42°C. To date, no vaccines are commercially available. For 50 years, the mainstay of antileishmanial therapy has been pentavalent antimony (sodium stibogluconate or meglumine antimonate). liposomal amphotericin B has replaced pentavalent antimony as the drug of choice for visceral disease.
. liposomal amphotericin B has replaced pentavalent antimony as the drug of choice for visceral disease..")
41
Alternative treatment regimens with acceptable cure rates are pentamidine, paromomycin, interferon-gamma plus antimony, and amphotericin B.

42
sodium stibogluconate (Rx) - Pentostam, stibogluconate sodium 20 mg Sb/kg/day (maximum 850 mg) IV/IM x20-28 days Anorexia AnorexiaNausea/vomiting Abdominal pain ECG changes
 - Pentostam, stibogluconate sodium 20 mg Sb/kg/day (maximum 850 mg) IV/IM x20-28 days Anorexia AnorexiaNausea/vomiting Abdominal pain ECG changes")
43
Headache Lethargy Myalgia Raised liver enzymes Coughing and substernal pain Anaphylaxis (rare) Fever Sweating Flushing Vertigo Bleeding from nose or gum Jaundice Rash Pain and thrombosis on intravenous administration, intramuscular injection also painful
 Fever Sweating Flushing Vertigo Bleeding from nose or gum Jaundice Rash Pain and thrombosis on intravenous administration, intramuscular injection also painful")
44
Contraindications Significant renal impairment; breast-feeding.

Similar presentations













>")
>")







 (VL) Leishmania tropica (CL) Leishmania major (CL) Leishmania aethiopica (CL) Leishmania mexicana (Complex)>")

. caused by intracellular protozoan parasites of the genus Leishmania transmitted by phlebotomine sandflies disease involving.>")

 (Dum-Dum fever, Black fever)}>")