Download presentation
Presentation is loading. Please wait.

1
“Diagnostic value of procalcitonin in well appearing young febrile infants”
Pediatrics 2012; 130:

2
Background Well appearing babies who are febrile are a diagnostic challenge. Current practise in the UK and SCH is to use WCC and CRP to aid diagnosis of invasive bacterial infection – but value as diagnostic markers variable. Procalcitonin increasingly used across Europe for the management of febrile babies and other bacterial infections.

3
Procalcitonin (PCT) Peptide precursor of the hormone calcitonin.
Produced by parafollicular cells of the Thyroid, lungs and intestines. Levels rapidly rise in response to bacterial infection, not with viral infection. ½ life 25-30hrs

4
Paper Retrospective study looking at febrile, well appearing babies under 3 months. Recordings of procalcitonin, WCC and CRP. Invasive Bacterial Infection (IBI) the primary outcome. Serious Bacterial Infection also looked at. Also aimed to determine values in babies with negative urine dip.
 the primary outcome. Serious Bacterial Infection also looked at. Also aimed to determine values in babies with negative urine dip.")
5
Methods Retrospective analysis of patients 2007-2010
Infants <3 months/FWS/PCT & blood culture CRP and WCC also if possible 5 Spanish, 2 Italian hospitals LPs on a case-by-case basis

6
Results

7
1112 infants met criteria 289(26%) SBI 23(2.1%) IBI - all +ve blood culture - no +ve CSF
 SBI 23(2.1%) IBI - all +ve blood culture - no +ve CSF")
10
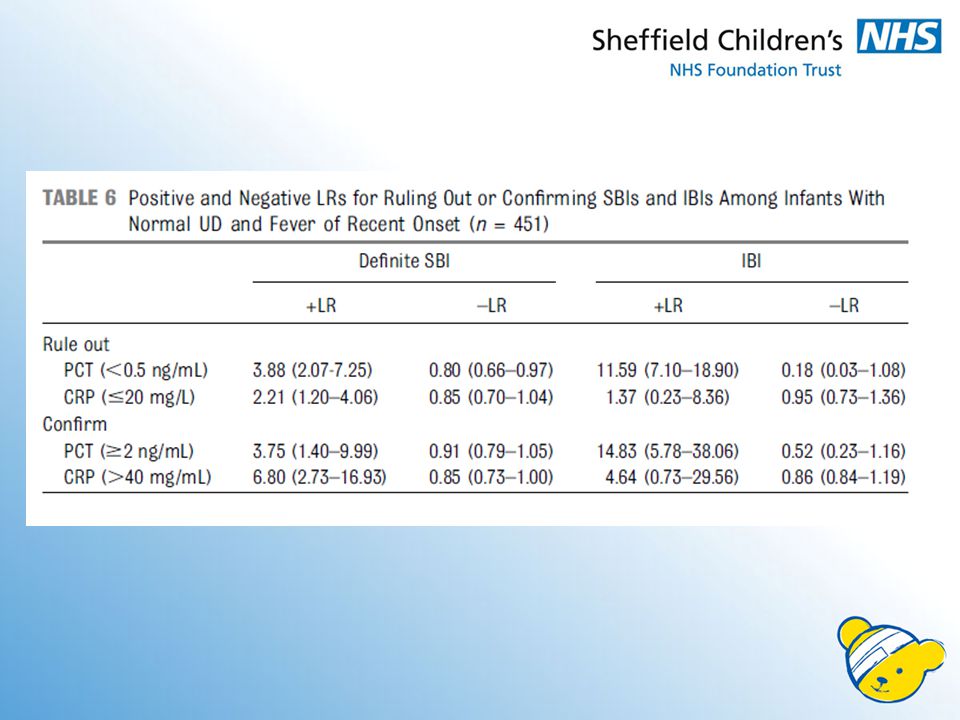
23 IBIs 6 had CRP <20 (4 had PCT >2ng/ml) = 26%
4 had PCT <0.5ng/ml (none with CRP >40) = 17%
 = 17%")
11
Receiver-operator characteristic curves

14
“Only PCT ≥0.5ng/mL was found to be an independent risk factor for IBI in the multivariate analysis (odds ratio 21.69)”
")
15
Pediatrics 2012; 130:815-822 CASP critical appraisal of study
“Diagnostic value of procalcitonin in well appearing young febrile infants” Pediatrics 2012; 130: CASP critical appraisal of study

16
Was there a clear question for the study to address?
Yes In babies under 3 months who are febrile and appear well, do PCT levels offer good prognostic value to identify invasive bacterial infection?

17
Was there a comparison with an appropriate reference standard?
Yes Comparison to CRP, WCC and TNC

18
Did all the patients get the diagnostic test and the reference standard?
But 99.8% did get both PCT and CRP, so nearly!

19
Could the results of the test of interest have been influenced by the results of the reference standard? No Both CRP and PCT measured in 99.8% of cases

20
Is the disease status of the of the tested population clearly described?
Yes Invasive bacterial infection confirmed on blood culture or positive CSF

21
Were the methods for performing the test described in sufficient detail?
Yes, but…. Explained in detail but some discrepancies: Some centres used “normal paediatric assessment triangle”, some didn’t. Variation in collection of urine (Spain SPA or catheter, Italy bag urine x2) Therefore different rates of “UTI” (22 vs 30%)
 Therefore different rates of UTI (22 vs 30%)")
22
What are the results?

25
Are the results presented in such a way we can work them out?
No One small table of actual figures, all other results are statistical diagrams and calculated figures. Ranges of figures don’t match the text.

26
Are the results presented in such a way we can work them out?
No, ctd Different graphs and cut-off points mentioned at different times. Only 23 IBIs, could have shown values for each

27
“Only PCT ≥0.5ng/mL was found to be an independent risk factor for IBI in the multivariate analysis (odds ratio 21.69)” ?

28
How sure are we about the results?
Some couldn’t have happened by chance (p values <0.05) For PCT vs CRP, +ve LR 95% confidence intervals don’t overlap (when confirming IBI +ve LR)
 For PCT vs CRP, +ve LR 95% confidence intervals don’t overlap. (when confirming IBI +ve LR)")
29
How sure are we about the results?
Not so sure? Receiver operator curve areas, CIs all overlap Many false +ves and –ves Text and tables don’t match Unreliable and inconsistent urine collection ? No meningitis in all patients

30
Can the results be applied to the patients of Sheffield?
Yes/No Developed populations, similar diagnostic criteria and similar disease processes But what cutoff points would we use? SBI not reliable, and we rarely use urine bags and catheters for samples. Also, don’t use urine dip < 1 year. Better performance when ruling in an infection, more useful clinically Only 2% of these patients had IBI, and results didn’t mention if these were the patients who became clinically unwell anyway, or at what time (not excluded)
")
31
Can the test be applied to patients in Sheffield?
Cost of PCT assay £10-£15 ? CRP £10? Simple lab test, ? Compatible with existing machinery

32
Were all outcomes important to the individual or population considered?
Yes Early detection of IBI and prompt use of antibiotics would improve outcome

33
What would be the impact of using this test on the patients in Sheffield?
? More IBI diagnosed early and treated promptly, leading to better outcome ? Less antibiotics prescribed for non IBIs. Additional benefit, or instead of CRP?

34
Conclusion Positives Good idea and potentially a good pro-inflammatory marker. Seems to perform well, with good +ve LR. Positive predictor more useful, to identify the 2% with IBI and start abx Better than CRP, but is this good enough to change practise?

35
Conclusion Limitations Data incomplete and difficult to interpret
Unreliable data collection and definition of diagnostic criteria. All SBI diagnosis not reliable and non- transferrable to Sheffield

36
Questions?

Similar presentations





 in any IB science course is based upon two kinds of assessments.>")




 in adults has grown rapidly. Although.>")

 Director of Evidence-Based Practice, Quality Management.>")











