Download presentation
Presentation is loading. Please wait.

1
2014 Annual IHS Podiatry Meeting November 22, 2014

2
. “We do these things not because they are easy, but because they are hard.” John F. Kennedy Rice University Sept. 12, 1962

3
“Coming Together is a Beginning, Keeping Together is Progress, Working Together is Success” Henry Ford

5
Jeffrey M. Robbins, DPM Director, Podiatry Service VACO November 22, 2014

6
At the conclusion of this activity, the participant will be able to: A. Describe the importance of the Prevention of Amputation in Veterans Everywhere Program B. List the components of calculating foot risk score C. Discuss the morbidity and mortality associated with first onset diabetic ulceration

7
Jeffrey M. Robbins, DPM has no financial interest or relationships to disclose.

9
Emphasized importance of highest quality amputee care Identified veterans with amputation as a special disability group Chartered the Advisory Committee on Prosthetics and Special Disabilities Programs

10
1. PURPOSE: This Veterans Health Administration (VHA) Directive defines the scope of the care and treatment provided to veteran patients at risk of primary or secondary limb loss. This is accomplish through the Prevention of Amputation in Veterans Everywhere (PAVE) Program
 Directive defines the scope of the care and treatment provided to veteran patients at risk of primary or secondary limb loss. This is accomplish through the Prevention of Amputation in Veterans Everywhere (PAVE) Program.")
11
Developed to meet the changing needs of veterans ◦ more neuropathy, PVD and diabetes ◦ fewer traumatic amputations ◦ New issues in 2006 with returning OEF/OIF Vets Established a model of care to prevent or delay amputations Proactive early identification of “at risk” populations ◦ Especially veterans with diabetes Track from date of entry to discharge back to the community

12
3. POLICY: It is VHA policy that the PAVE program be established at all VA medical centers. The program will at a minimum provide for

13
1. Screening of at-risk populations 2. Identification of high risk patients 3. Timely and appropriately referral

14
4. Each patient who has suffered an amputation should be offered a visit by their mental health consultation team, to assess coping and provide support as needed either in an individual or group format. (This approach avoids stigmatizing anyone as being singled out as having mental or emotional issues and also minimizes the potential for missing someone who is 'suffering in silence")
.")
15
5. Development of a system to identify and track patients with amputation or those at risk for amputation. ◦ NOTE: (The VACO Patient Care Services PAVE ProClarity Cubes are an acceptable resource from which to develop such a system)
.")
16
6. A PAVE coordinator to provide for ◦ (a) organizational support for the PAVE team, ◦ (b) communication conduit between administration and PAVE/Amputee clinic team providers, ◦ (c) a smooth transition of the DOD patient into the VA system
 organizational support for the PAVE team, ◦ (b) communication conduit between administration and PAVE/Amputee clinic team providers, ◦ (c) a smooth transition of the DOD patient into the VA system.")
17
7. A PAVE Committee should be established to coordinate efforts to address the primary amputation prevention needs of “at risk” patients, and the secondary amputation prevention needs for those patients who have already suffered an amputation. This includes patients who had their amputations outside the VA system of care (e.g. OEF/OIF, private hospital, etc). This may be accomplished by the PAVE coordinators incorporating their efforts in existing primary amputation prevention committees within the medical centers.
. This may be accomplished by the PAVE coordinators incorporating their efforts in existing primary amputation prevention committees within the medical centers..")
18
The field based PAVE Oversight Committee made up of clinical leaders from endocrinology/diabetes, podiatry, PM&R, Prosthetics, nursing the VISN’s, OQP responsible for recommendations for data collection and analyses to permit program evaluation of the screening, surveillance, salvage, and rehabilitative components of the PAVE program, including the following

19
1. Identification of veterans at risk for or who have sustained an amputation Age adjusted and stratified rates of major (AKA and BKA) and minor amputations, and lower extremity non-venous ulcers Patient knowledge and performance of recommended self foot care practices, and satisfaction with foot care. VISN and Facility adherence to the PAVE Directive with respect to formal policies and coordination strategies
 and minor amputations, and lower extremity non-venous ulcers Patient knowledge and performance of recommended self foot care practices, and satisfaction with foot care. VISN and Facility adherence to the PAVE Directive with respect to formal policies and coordination strategies.")
20
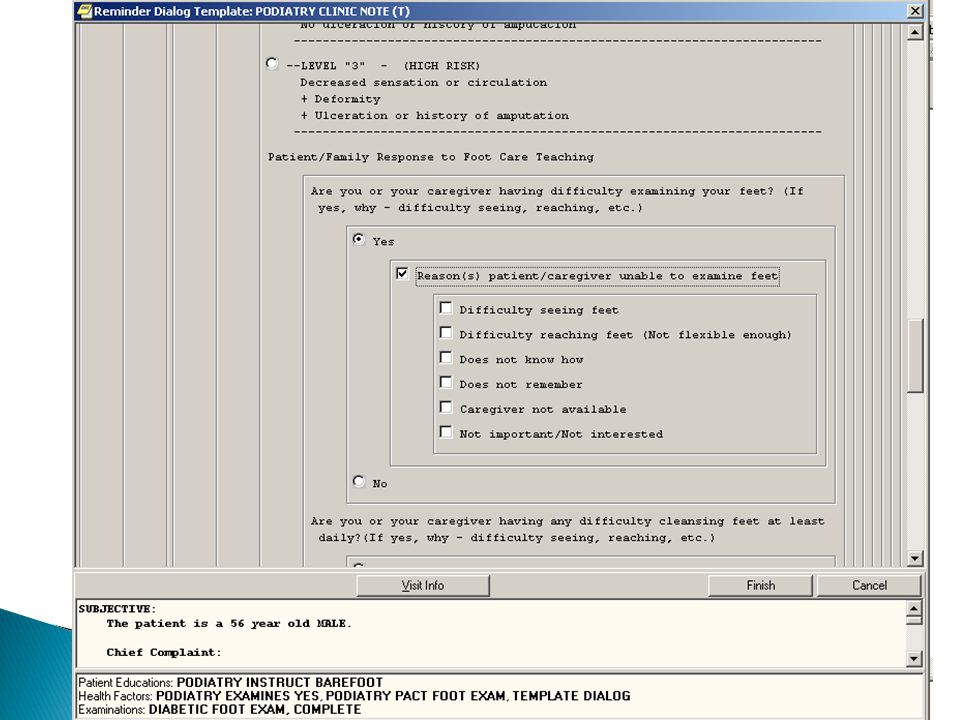
The PAVE committee will use these analyses to identify best practices from the field, and to make recommendations to achieve excellence in patient centered care to the PAVE Oversight Committee for program improvements Recommendations RE: self foot care behaviors

21
Let patients know that these self care behaviors are important to their provider Allows the provider to reinforce the behavior in a quick and efficient manner.

22
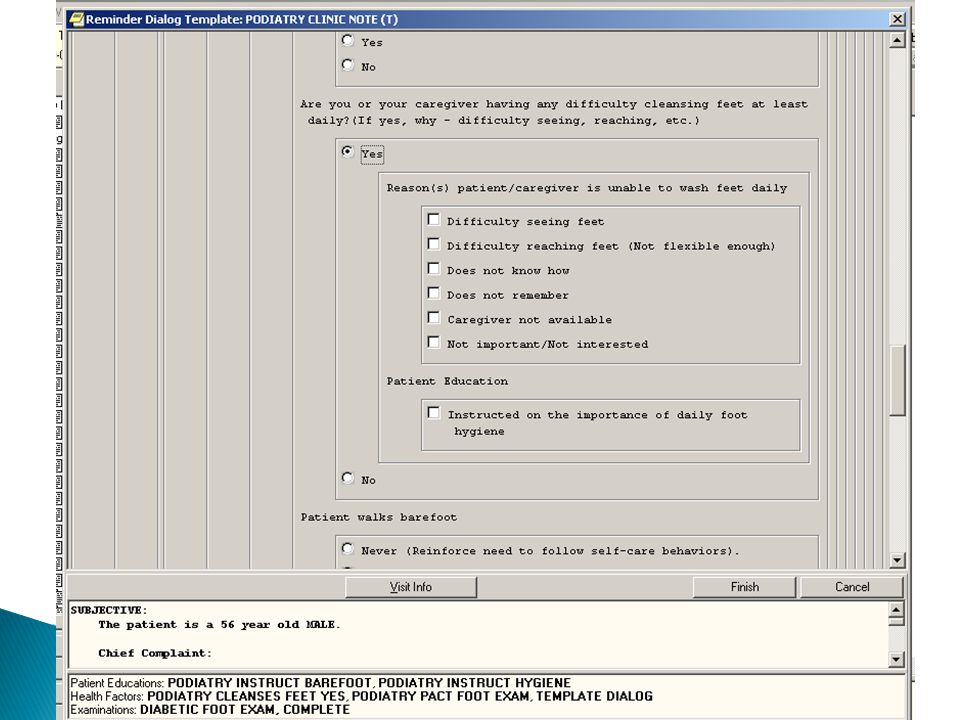
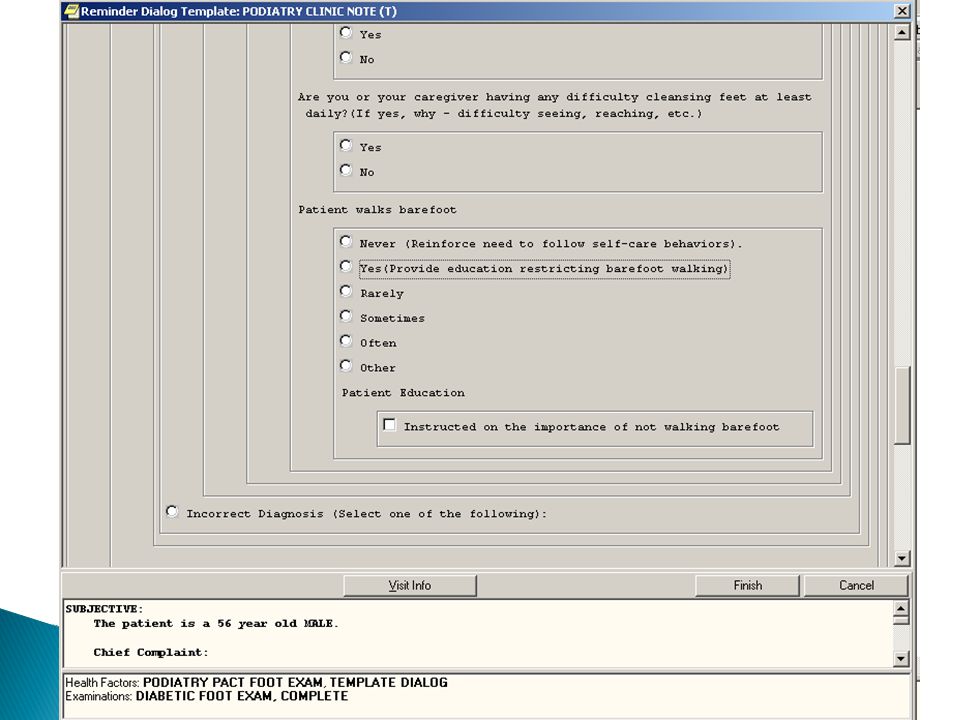
Are you or your caregiver having an problems inspecting your feet every day? ◦ Can’t see or can’t reach ◦ Can we offer you a mirror, etc. Are you or a caregiver having an problems washing your feet? ◦ Can’t see or can’t reach ◦ Can we offer you a sponge on a stick, etc. Do you walk barefoot?

27
A. The Network Director is responsible for: B. Medical Center Director C. Chief of Staff D. PAVE Coordinator

28
Directive provides recommendations for; ◦ Foot Checks ◦ Foot Examinations ◦ Risk Score assignments ◦ Referral strategy ◦ Provides guidelines not mandates!

29
1. FOOT Screening This involves: a. Visual inspection of the skin surface for any lesions, deformities, color or temperature changes or ulcers; b. Screening for circulation, i.e., the palpation of pedal pulses in the foot; and c. Sensory testing using a Semmes-Weinstein 5.07 monofilament to check for loss of protective sensation.

30
2. FOOT Examination This involves a more in-depth evaluation of the foot’s circulation and sensation as well as foot deformities. During this examination, patients are evaluated by a "foot care specialist," e.g., Prevention of Amputation in Veterans Everywhere (PAVE) program member, vascular surgeon, podiatrist, or other health care professional demonstrating appropriate education, training, competencies and licensure necessary to provide such care
 program member, vascular surgeon, podiatrist, or other health care professional demonstrating appropriate education, training, competencies and licensure necessary to provide such care.")
31
RISK ASSESSMENT LEVEL "At-risk" is defined as patients with diabetes, peripheral vascular disease and/or end stage renal disease, who are considered highly susceptible to develop foot ulcers. “High Risk” is defined as any patient who has had an amputation for any reason, and patients with a foot risk score of 2 or 3.

32
a. Level 0, Normal Risk. These patients have no evidence of sensory loss, diminished circulation,, ulceration, or history of ulceration or amputation. Patients with diabetes should receive foot care education and annual foot screening. These patients do not require therapeutic footwear. b. Level 1, Low Risk. These individuals demonstrate one or both of the following Foot deformity or minor foot infection (and a diagnosis of diabetes). Patient education, preventative care and annual foot screening are required. The patients in this category and the following two categories (Level 2 and Level 3) should not walk barefoot. Special attention is to be directed to shoe style and fit. These individuals do not need therapeutic footwear.
. Patient education, preventative care and annual foot screening are required. The patients in this category and the following two categories (Level 2 and Level 3) should not walk barefoot. Special attention is to be directed to shoe style and fit. These individuals do not need therapeutic footwear..")
33
c. Level 2, Moderate Risk. These individuals demonstrate sensory loss (inability to perceive the Semmes-Weinstein 5.07 monofilament) and may have one additional finding below. Diminished circulation as evidenced by absent or weakly palpable pulses, (this would require follow-up examination to determine level of vascular disease before a final risk score can be determined) Foot deformity or minor foot infection (and a diagnosis of diabetes).
 and may have one additional finding below. Diminished circulation as evidenced by absent or weakly palpable pulses, (this would require follow-up examination to determine level of vascular disease before a final risk score can be determined) Foot deformity or minor foot infection (and a diagnosis of diabetes)..")
34
These individuals require: ◦ therapeutic footwear and orthoses to accommodate foot deformities, to compensate for soft tissue atrophy, and to evenly distribute plantar foot pressures. ◦ Patient education, regular preventive foot examination and care in podiatry or other foot care specialty clinic. Patient health education (PHE) must include the implications of sensory loss and the importance of daily foot inspections. NOTE: May require Diabetic Socks and Depth Inlay Shoes based on clinical judgment.
 must include the implications of sensory loss and the importance of daily foot inspections. NOTE: May require Diabetic Socks and Depth Inlay Shoes based on clinical judgment..")
35
Level 3, High Risk. These individuals demonstrate peripheral neuropathy with sensory loss (inability to perceive the Semmes- Weinstein 5.07 monofilament) and diminished circulation and foot deformity or minor foot infection (and a diagnosis of diabetes). or any of the following by itself Prior ulcer, Osteomyelitis or history of prior amputation Severe PVD (intermittent claudication, dependent rubor with pallor on elevation, or critical limb ischemia manifested by rest pain, ulceration or gangrene., Charcot’s joint disease with foot deformity. End Stage Renal Disease ◦ These individuals are at highest risk of lower extremity events. Individuals in this category require extra depth footwear with soft molded inserts. They may require custom molded shoes and braces (e.g., double upright brace, patella tendon bearing orthoses, etc.). More frequent clinic visits are required with careful observation, regular preventive foot care, and footwear modifications. NOTE: May require Diabetic Socks, Depth Inlay Shoes or Custom-Molded Orthopedic Shoes based on clinical judgment.
 and diminished circulation and foot deformity or minor foot infection (and a diagnosis of diabetes). or any of the following by itself Prior ulcer, Osteomyelitis or history of prior amputation Severe PVD (intermittent claudication, dependent rubor with pallor on elevation, or critical limb ischemia manifested by rest pain, ulceration or gangrene., Charcot’s joint disease with foot deformity. End Stage Renal Disease ◦ These individuals are at highest risk of lower extremity events. Individuals in this category require extra depth footwear with soft molded inserts. They may require custom molded shoes and braces (e.g., double upright brace, patella tendon bearing orthoses, etc.). More frequent clinic visits are required with careful observation, regular preventive foot care, and footwear modifications. NOTE: May require Diabetic Socks, Depth Inlay Shoes or Custom-Molded Orthopedic Shoes based on clinical judgment..")
36
Foot Check in Primary Care FRS 0 or 1 FRS 2 or 3 Referred to podiatry for a foot examination Annual foot check in Primary Care FRS 0 or 1 FRS 2 or 3 Appropriate level of on- going care

37
Patients 1,827,620 Age Avg 68.9 Amputation Last 18 Mos 8,724 Hx Amputation Last 10 Years 66,332 Hx Charcot Foot 6,412 Hx Diabetes 1,528,289 Hx ESRD 20,212 Hx Foot Deformity or Surgery432,312 Hx Gangrene 9,001 Hx Neuropathy 414,248 Hx Non-Healing Ulcer 72,769 Hx Osteomyelitis 16,989 Hx PVD 344,354 Hx PVD Surgery 10,558 Hx Smoking % 20.71%

43
Best system anywhere but we need to do even better We have been following patient centered medical home principals Must do better to convince patients to engage in self foot care practices. PAVE and ASoC coordination, co-operation should help us improve the system of care. HIS with support from leadership should be able to develop a similar system of care.

44
Where do we stand?

45
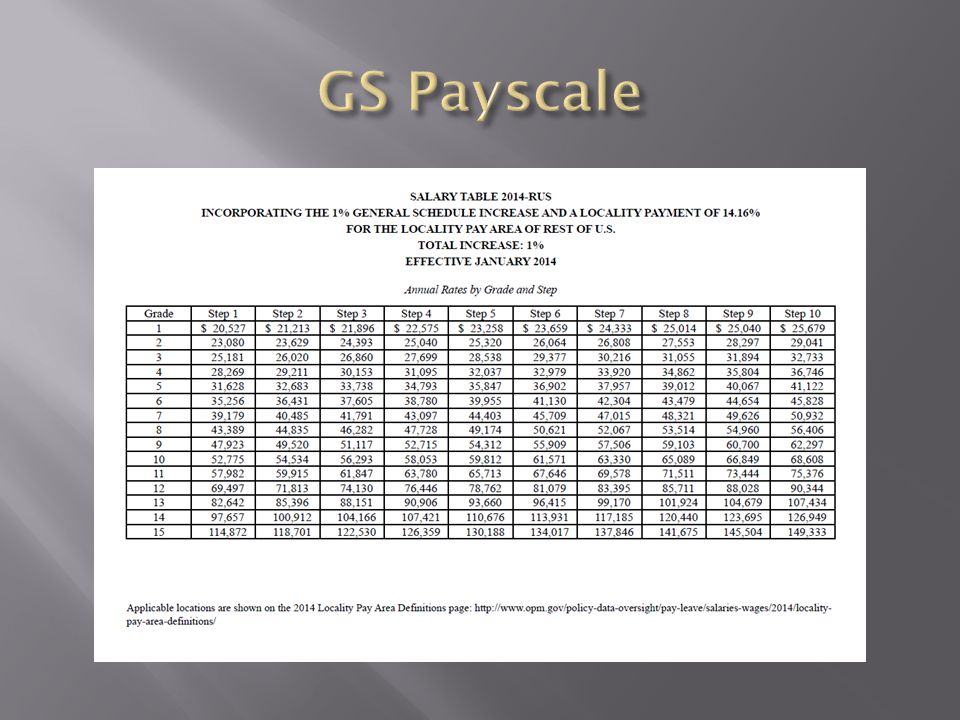
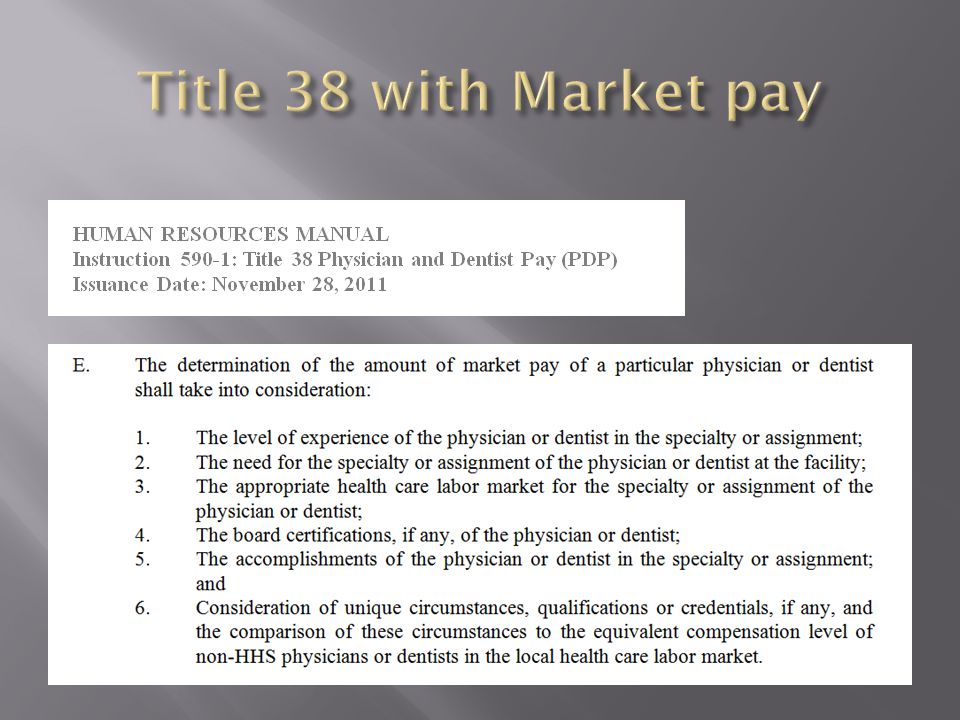
Title 5. GS (General Schedule) Pay scale. Eligible for Title 38 Max salary in Title 38 is limited by Level IV of Executive Schedule (Currently $157,000) Ineligible for Market Pay This is reserved for Physicians (MD,DO) and Dentists Eligible for Overtime
 Ineligible for Market Pay This is reserved for Physicians (MD,DO) and Dentists Eligible for Overtime.")
47
Title 38 Pay table matches GS pay scale. Ineligible for Market Pay. Ineligible for Overtime. Ineligible for LRP

50
IHS LRP is typical but not guaranteed. Local HR recommends podiatrists hired at a 14-1. Appointments above the minimum possible but are difficult to obtain. Recruitment bonuses can be difficult to obtain. Relocation expenses are offered but typically amount to less than $10,000 and usually will not pay to ship your car. Locality pay/ adjustment. Board Certification Pay? “Can be considered as a factor in a superior qualifications/appointment above the minimum or an incentive justification. No separate payment otherwise.” Eligible for Retention Allowance (up to 25%) but can be difficult to obtain and may be discontinued in next few years.
 but can be difficult to obtain and may be discontinued in next few years..")
51
Regulations tightened Ongoing Retention incentives are “problematic” Must be justified. Succession plan must be in place. IHS has a cap on the 3Rs; IHS is NOT in danger of going over the cap at this time.

52
U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES/INDIAN HEALTH SERVICE RECRUITMENT, RELOCATION, AND RETENTION INCENTIVES CONTINUATION, REDUCTION, OR TERMINATION OF RETENTION INCENTIVE The basis for paying all retention incentives must be certified at least annually, in writing, by the Authorized Agency Official, whether or not there is a written service agreement. Note: A retention incentive must be terminated if the employee is demoted or separated for cause, receives a rating of less than Fully Satisfactory or equivalent, or otherwise fails to fulfill the service agreement, if applicable. The organization must reduce or terminate the amount/percentage of a retention incentive when conditions change such that the original determination to pay the incentive no longer applies, or when payment is no longer warranted given a change in labor market factors, or an incentive is no longer required to retain the employee(s), or the need for the employee’s service no longer justifies the incentive. EMPLOYEE INFORMATION Name: Position Title: Pay Plan, Occupation Series, Grade/Step: Organizational Unit: Duty Station: Work Schedule: ☐ Full-time ☐ Part-time - number of normal hours per pay period: REVIEW OF INCENTIVE Basis for Review: ☐ Annual certification ☐ OtherThis is a(n): ☐ Individual incentive ☐ Group incentive Effective date of initial incentive: Total amount of initial incentive: Percentage of initial incentive: Retention incentive is to be terminated effective: Retention incentive is to be continued effective: Not-to-Exceed: Total amount of continued incentive: Percentage of continued incentive: JUSTIFICATION FOR CONTINUING INCENTIVE Describe, as applicable, how the following factors contribute to the determination that the retention incentive is necessary. Employment trends and labor market factors. Recent recruitment efforts. Special or unique competencies required for the position. Efforts to use non-pay authorities in lieu of or in addition to retention incentives. Desirability of duties, work or organizational environment, or geographic location of the position. Extent to which employee’s departure would impair the organization’s ability to carry out an activity, perform a function, or complete a project that the organization deems essential to its mission.
, or the need for the employee’s service no longer justifies the incentive. EMPLOYEE INFORMATION Name: Position Title: Pay Plan, Occupation Series, Grade/Step: Organizational Unit: Duty Station: Work Schedule: ☐ Full-time ☐ Part-time - number of normal hours per pay period: REVIEW OF INCENTIVE Basis for Review: ☐ Annual certification ☐ OtherThis is a(n): ☐ Individual incentive ☐ Group incentive Effective date of initial incentive: Total amount of initial incentive: Percentage of initial incentive: Retention incentive is to be terminated effective: Retention incentive is to be continued effective: Not-to-Exceed: Total amount of continued incentive: Percentage of continued incentive: JUSTIFICATION FOR CONTINUING INCENTIVE Describe, as applicable, how the following factors contribute to the determination that the retention incentive is necessary. Employment trends and labor market factors. Recent recruitment efforts. Special or unique competencies required for the position. Efforts to use non-pay authorities in lieu of or in addition to retention incentives. Desirability of duties, work or organizational environment, or geographic location of the position. Extent to which employee’s departure would impair the organization’s ability to carry out an activity, perform a function, or complete a project that the organization deems essential to its mission..")
56
http://www.bls.gov/oes/current/oes291081.htm

59
http://www.bls.gov/oes/current/oes291081.htmhttp://www.bls.gov/oes/current/oes291081.htm

60
APMA 2012 Surveymeanaverage Group Practice employed$192,767 Hospital employed$226,760 210,000 ACFAS 2012 Survey Board Certified RRA$259,899 Board Certified Foot$213,975 237,000 GS Pay scale APMA 25% Ret Sub Total LRP Total APMA 14-1 $99,881 -52% 24,970 124,851 18,000 142,851 -32% 14-6 $116,525 -45% 29,131 145,656 18,000 163,656 -22% 15-6 $137,069 -35% 34,267 171,336 18,000 189,336 -10%

61
Title 5 special salary approved OPM Title 38 special salary approved HHS (“easier”) Could shift Max salary to lower grade/step: For example could have 15-5 making $157,000 You will always be capped however and may “pigeon hole” yourself within pay structure. Long term may hurt your argument for Market pay

68
Survey Data Comparison between Civil Service Tribal VA Private Hospital Employed MD, DO, Dentists Board Certification

70
Topics: National Pod Council List Serve Podiatry File Server (FTP) National Library Of Medicine Access IHS Website USA Jobs Website
 National Library Of Medicine Access IHS Website USA Jobs Website")
71
The National Podiatry Council List Server List Moderator is Roland Palmquist, DPM

72
Purpose The List server allows rapid distribution of information to all members. This is essentially an e-mail distribution list.

73
How to Access Potential users must first sign up for the server by going here: http://listserv.ihs.gov/scripts/wa.exe?SUBED1=NATIONAL PODCOUNCIL&A=1 http://listserv.ihs.gov/scripts/wa.exe?SUBED1=NATIONAL PODCOUNCIL&A=1 Fill in the form and click to Subscribe/Unsubscribe.

74
How It Works Send an e-mail addressed to: nationalpodcouncil@listserv.ihs.gov I will be notified (as the list serve Moderator) of your request. I will read the post and approve to send to all. Sometimes I will question if you want it posted to everyone and contact you for clarification.

75
WARNING When you respond to an e-mail on the list serve it will automatically send it to me to post on the list server. I have received several private correspondences which people sent to the list serve rather than reply to an individual directly by mistake!

76
What is FTP site This is a secure file sharing site. Use this to share documents/files with the group.

77
How to Access FTP Site ftp://ftp.ihs.gov/pubs/NationalPodiatryCouncil Go to above link and select a file to view. Files are READ ONLY.

78
How Do I Post to the FTP Site? Attach the file to an E-mail and sent to: Wes Yamada [WesY@GRHC.ORG] If files are larger than 100mb, see next slide.

79
How Do I Post Files to Large to E-Mail? If you have a large file you can not attach to an e- mail, you can transfer via IHS Secure File Transfer here (up to 100mb)… You could have the user send the file utilizing the Secure data transfer service https://securedata.ihs.gov/bds/Login.do https://securedata.ihs.gov/ (Redirects to above) https://securedata.ihs.gov/
… You could have the user send the file utilizing the Secure data transfer service (Redirects to above)")
80
This is the NIH Link. Choose a data base-Pub Med.

81
Enter search parameters and search.

82
Preview Articles Here.

83
Click NIH Library Link to Access Article.

84
Check Links to See if Free/ Downloadable

85
Look for PDF download and Click

86
Here is the Article to Read/Save

87
What If I Can’t Open a Free Copy? Click on NIH Library Link.

88
Request Through Document Delivery

89
Choose Indian Health Service

90
Complete Form and Submit

91
Inter Library Loan-Summary You can do your PubMed searches through HSRL online library and be able to either obtain full text of the article if we own it or the ability to order the article at that time when we do not own it. Go to: http://nihlibrary.ors.nih.gov/ezproxy/ihs.htmhttp://nihlibrary.ors.nih.gov/ezproxy/ihs.htm Click on : Click here to login with your IHS Agency credentialsClick here to login with your IHS Agency credentials Log in with your user credentials or IHS ID card. Click the Pub med link. Search for the info you want. Click the NIH library button in corner. Choose the IHS User bar. Fill in your e-mail address twice and send. Diane Cooper Informationist/Biomedical Librarian for IHS Division of Library Services National Institutes of Health

92
IHS Website www.ihs.gov General info about IHS

95
Federal Job Search Engine https://www.usajobs.gov/ Apply for Federal Jobs here.

96
Questions?

97
NATIONAL IHS PODIATRY: A YEAR IN REVIEW Title 38 – Market Pay Contact with VA and Federal Services Strongly Recommend becoming a Member of the Federal Services APMA Next meeting: APMA National – Orlando; July 23-26, 2015

98
NATIONAL IHS PODIATRY: A YEAR IN REVIEW August 10,2014 – Dr. Wesley Yamada – new Podiatry Chief Clinical Consultant (CCC) for the IHS Dr. Matthew Pettingill – Deputy CCC Free Monofilaments: Contact Sheila Silva – Gallup Warehouse: (505) 722 1578 or the HRSA website http://www.hrsa.gov/leaporder/ http://www.hrsa.gov/leaporder/
 for the IHS Dr. Matthew Pettingill – Deputy CCC Free Monofilaments: Contact Sheila Silva – Gallup Warehouse: (505) or the HRSA website")
99
NATIONAL IHS PODIATRY: A YEAR IN REVIEW Shoes – Sole Nation Shoes Going Our of Business Contact Ernesto Castro 480-390-8983 or Isabel – 480-612-7433 ernesto@solenationhealth.com or ernestocastro@cox.net ernesto@solenationhealth.com Ernie is willing to sell the Company to any Tribe FTP Website Reorganization Meeting Minutes and Slides - Project Updates Annual Meeting Prep- Articles Wound Care Best Practice Algorithm

100
NATIONAL IHS PODIATRY: A YEAR IN REVIEW Automated Data Collection Tool for Wound Care AZ State Senator Carlyle Begay Directory of Podiatrists Salary Survey: Federal: from GS13 – GS15 <$100K = 2$100-$150K = 4 (2*) $150-$175K = 5 $175 - $200K = 1 >$200K = 2 Others: “GS-14/8 + retention; GS15 + retention; ?GS14) (no actual salary numbers given)
 $150-$175K = 5 $175 - $200K = 1 >$200K = 2 Others: GS-14/8 + retention; GS15 + retention; GS14) (no actual salary numbers given)")
101
NATIONAL IHS PODIATRY: A YEAR IN REVIEW Attempts of Council Charter Submission Do we want or need it? CCC vs NCIHP Number of CCC’s = 18 (Addiction/Pain Med, Adv Practice RNs, Anesthesiology, ED, FM, ID, IM, OB, PA’s, PT, Geriatrics, Nephrology, Opthalmology, Optometry, Peds, PODIATRY, Surgery.) Number of National Councils = 3 (Nurses, Pharmacists and Dental) Number of Professions with CCC and NC = 1(*) (Dental has a Consultant to the CCC but they don’t have an official “Dental” Position)
 Number of National Councils = 3 (Nurses, Pharmacists and Dental) Number of Professions with CCC and NC = 1(*) (Dental has a Consultant to the CCC but they don’t have an official Dental Position).")
102
Questions?

103
STRATEGIC PLANNING How many can we do? Workgroup Volunteers for: DDTP (Division of DM Treatment and Prevention) for review of online material for DM foot care and Amputation Prevention Program PDs/Recruitment Standards OTHERS: Council or not Market Pay- National registry of IHS DPMs Salary Survey - Grants Peer Review- Getting Started Packet IPC Residency Program and/or Rotation development Establish Best Practice Wound Care/Amputation Prevention and document (Peer Review-data for Rockville Funding)
 for review of online material for DM foot care and Amputation Prevention Program PDs/Recruitment Standards OTHERS: Council or not Market Pay- National registry of IHS DPMs Salary Survey - Grants Peer Review- Getting Started Packet IPC Residency Program and/or Rotation development Establish Best Practice Wound Care/Amputation Prevention and document (Peer Review-data for Rockville Funding).")
104
Questions?

105
STRATEGIC PLANNING Workgroup Volunteers for: DDTP (Division of DM Treatment and Prevention) for review of online material for DM foot care and Amputation Prevention Program PDs/Recruitment Standards OTHERS: Council or not Market Pay- National registry of IHS DPMs Salary Survey - Grants Peer Review- Getting Started Packet IPC Residency Program and/or Rotation development Establish Best Practice Wound Care/Amputation Prevention and document (Peer Review-data for Rockville Funding)
 for review of online material for DM foot care and Amputation Prevention Program PDs/Recruitment Standards OTHERS: Council or not Market Pay- National registry of IHS DPMs Salary Survey - Grants Peer Review- Getting Started Packet IPC Residency Program and/or Rotation development Establish Best Practice Wound Care/Amputation Prevention and document (Peer Review-data for Rockville Funding)")
106
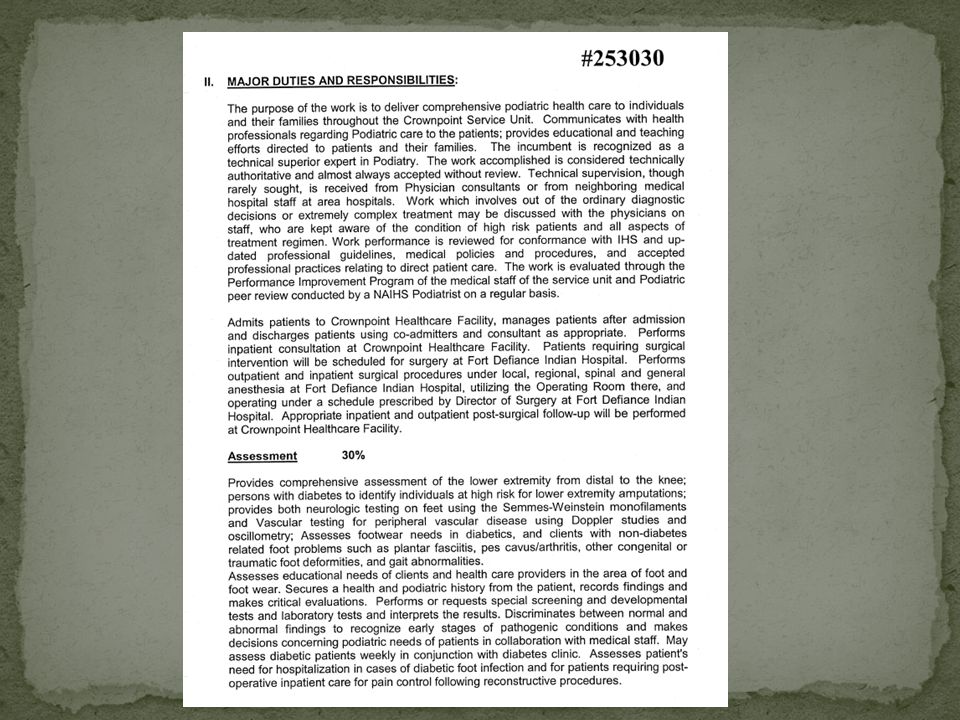
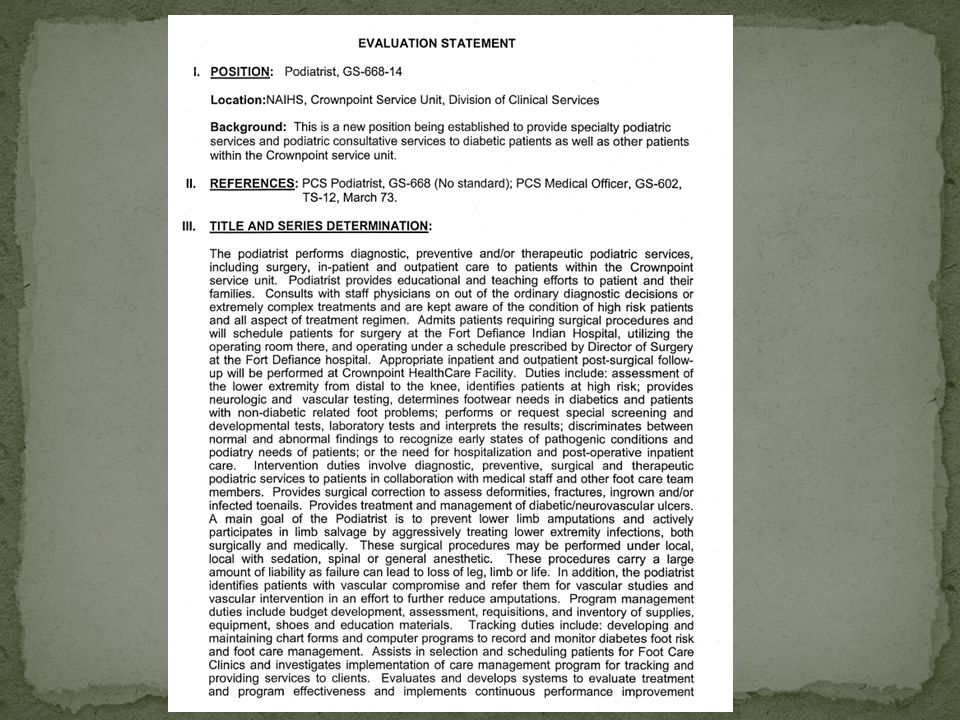
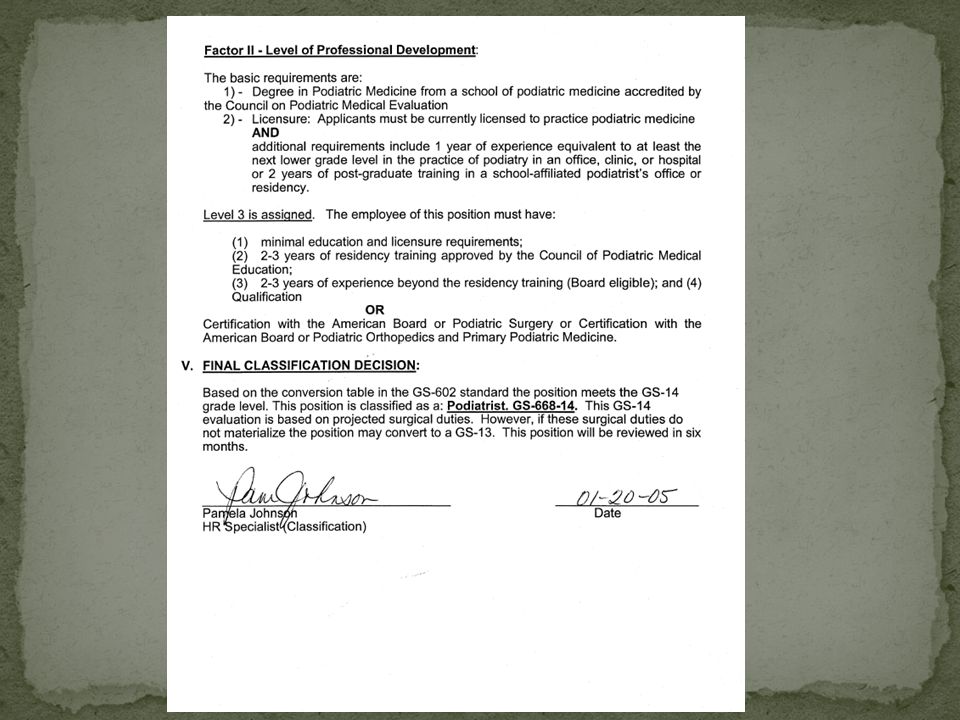
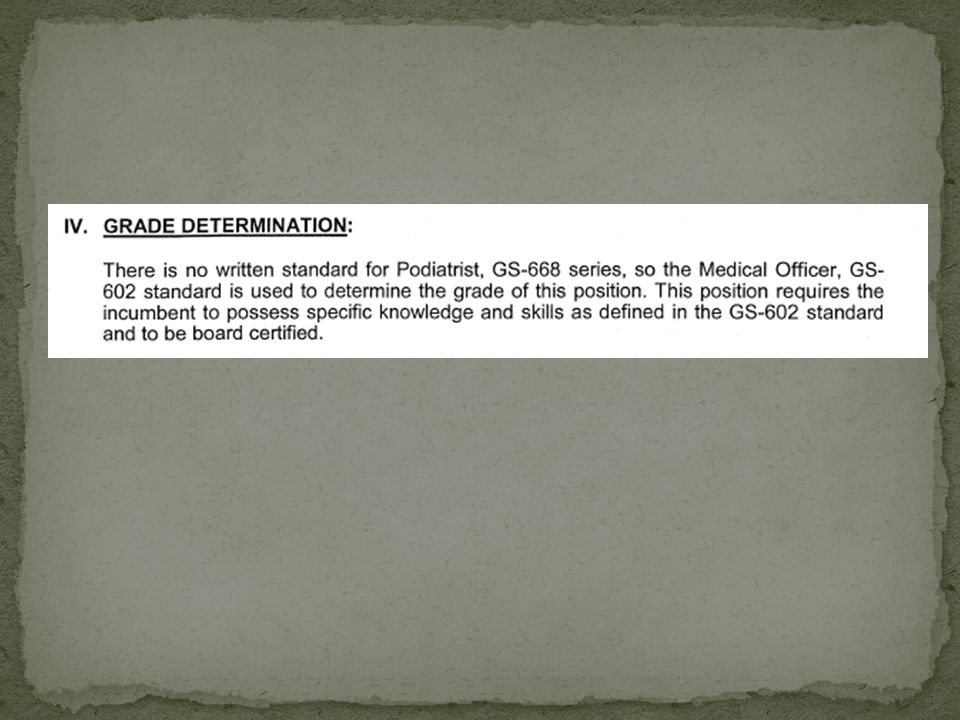
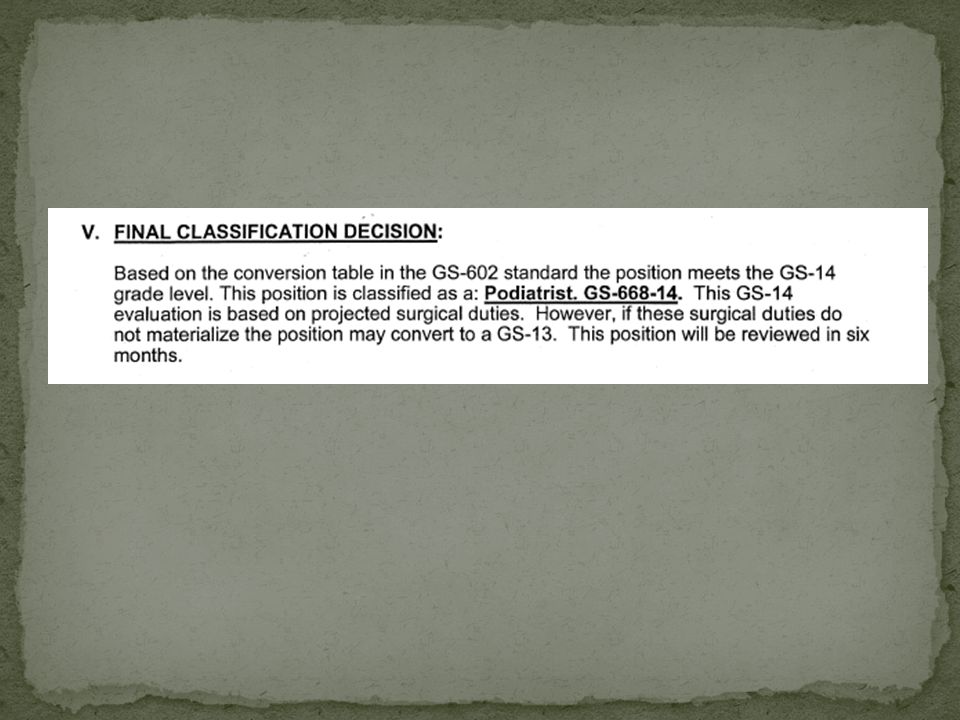
Standardized PD

115
Crownpoint Phoenix

117
Crownpoint Phoenix

Similar presentations




































 970-8421.>")












