Download presentation
Presentation is loading. Please wait.

1
ADHD in the Classroom: Diagnosis and Treatment Dr. Charles Pemberton, Ed.D, LPCC

2
Introduction Charles Pemberton M.Ed. In Counseling Psychology Ed.D. in Educational Counseling 16 years in Counseling and Mental Health Presented in England, South Africa, Central America, and US. Professor – UL and JCTCS Private Practice – 60% children and families ADHD Depression Aggression Anxiety

3
Today’s Schedule Diagnosis and Identification Treatment Medication Behavioral Modification Tools and Resources Questions

4
What won’t you get today Complete picture of medications A plan that will work everywhere with everyone

5
Causes of ADHD Biological Disorder Neurological – dopamine/norepinephrine Genetic Toxins Head injuries No evidence: Sugar Food additives Allergies Immunizations

6
Diagnosis Attention Deficit/Hyperactivity Disorder Diagnostic and Statistical Manual IV- TR DSM- IV-TR Within the “Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence” grouping, then subgrouped by the category of “disruptive or self injurious behavior”

7
ADHD, Major Diagnostic Features Often will not complete tasks Easily distracted by minor stimuli Work often messy and completed w/o thought Forgetful in day-to-day activities Impulsive (interrupting others, cannot wait turn, etc.) Fidgetiness Excessive talking
 Fidgetiness Excessive talking")
8
Subtypes of ADHD 314.01 ADHD, Combined Type Classical ADHD 314.00 ADHD, Inattentive Type Old ADD Seen more in girls 314.01 ADHD, Hyperactive-Impulsive Type 314.9 ADHD NOS Prominent symptoms but do not meet diagnostic criteria

9
Diagnostic Criteria for ADHD - inattention A 1. Must exhibit 6 or more symptoms of inattention, persisting for minimum of 6 months: fails to give close attention to details often has difficulty sustaining attention often does not seem to listen when spoken to directly often has difficulty organizing tasks and activities often loses things necessary for tasks often easily distracted by extraneous stimuli often forgetful in daily activities

10
Diagnostic Criteria - Hyperactive A 2. Must exhibit 6 or more symptoms of hyperactivity-impulsivity, persisting for minimum of 6 months often fidgets with hands or feet or squirms in seat often leaves seat in classroom often runs about or climbs excessively is often "on the go" or often acts as if "driven by a motor“ often talks excessively often blurts out answers often has difficulty awaiting turn often interrupts or intrudes on others

11
Diagnostic Criteria, cont’d: B. symptom onset PRIOR to age 7 years C. impairment present in two or more environments D. clear clinically significant impairment in functioning E. cannot be accounted for by other mental disorder

12
Prevalence What percentage of children “should” be diagnosed with a form of ADHD?

13
Prevalence of ADHD Estimated at 3-7% of school age children More common in males than females Often diagnosed during elementary school years.

14
Differential Diagnosis of ADHD Must distinguish from age-appropriate behaviors Mental Retardation or Learning Disability Oppositional behavior (ODD, Conduct D/O) Stereotypic Movement D/O Behavior due to medications Mood or Anxiety D/O
 Stereotypic Movement D/O Behavior due to medications Mood or Anxiety D/O")
15
Co morbidity Oppositional Defiance Disorder Conduct disorder Mood Disorder Anxiety Disorder Learning Disorder Tourettes Hx abuse or neglect, multiple foster homes, lead poisoning, Mental Retardation

16
Types according to Dr. Amen Type 1: Classic ADD Restlessness, hyperactivity, constant motion, troubles sitting still, talkative, impulsive behavior, lack of thinking ahead. Type 2: Inattentive ADD Short attention span (especially about routine matters), distractibility, disorganization, procrastination, poor follow-through/task completion.
, distractibility, disorganization, procrastination, poor follow-through/task completion..")
17
Types con’t Type 3: Overfocused ADD Worrying, holds grudges, stuck on thoughts, stuck on behaviors, addictive behaviors, oppositional/argumentative. Type 4: Limbic ADD Sad, moody, irritable, negative thoughts, low motivation, sleep/appetite problems, social isolation, finds little pleasure.

18
Types con’t Type 5: Temporal Lobe ADD Inattentive/spacey/confused, emotional instability, memory problems, periodic intense anxiety, periodic outbursts of aggressive behavior seemingly triggered by small events or intense angry criticisms directed at himself for failures and frustrations, overly sensitive to criticism and slights by others, frequent headaches and/or stomachaches, learning difficulties, and serious misperceptions/distortions of people and situations.

19
Types con’t Type 6: Ring of Fire ADD A ring of overactivity in the brain scan image which surrounds most of the brain is the source of the name for this type of ADD. too many thoughts, very hyper behavior, very hyper verbal expressiveness, a hypersensitivity to light, sound, taste, or touch.

20
Amen’s interventions Type 1: Classic ADD Stimulant medication (Ritalin, Adderall, etc.), a diet with more protein and less carbohydrates, intense aerobic exercise. Type 2: Inattentive ADD Stimulant medication, perhaps stimulating antidepressants (Welbutrin, for example), a diet with more protein and less carbohydrates, intense aerobic exercise.
, a diet with more protein and less carbohydrates, intense aerobic exercise..")
21
Amen’s interventions Type 3: Overfocused ADD An antidepressant that has a dual focus on two brain transmitters (seratonin and dopamine) (Effexor, for example), and/or an antidepressant that enhances seratonin (Prozac, Zoloft, Paxil, or others, for example). A stimulant medication may need to be added. A diet with less protein and increased complex carbohydrates will help, along with intense aerobic exercise. Type 4: Limbic ADD An antidepressant that is also stimulating (Effexor or Welbutrin, for example), with a stimulant medication could be added; a balanced diet, and intense exercise.
, with a stimulant medication could be added; a balanced diet, and intense exercise..")
22
Amen’s interventions Type 5: Temporal Lobe ADD Anticonvulsant medication (Neurontin, Depakote for example), a stimulant could be added; a diet with more protein and less simple carbohydrates. Type 6: Ring of Fire ADD Anticonvulsant medication (Neurontin, Depakote for example, a stimulant medication could be added; sometimes some of the newer, different anti- psychotic medications may help (Risperdal, or Zyprexa); a diet with more protein and less simple carbohydrates.
; a diet with more protein and less simple carbohydrates..")
23
Assessment – Am. Acad. Of Pediatrics Evaluate any child 6 to 12 years of age who shows signs of school difficulties, academic underachievement, troublesome relationships with teachers, family members, peers, and other behavioral problems. Use DSM-IV criteria; these require that ADHD symptoms be present in 2 or more of a child's settings, and that the symptoms adversely affect the child's academic or social functioning for at least 6 months. Requires information from parents or caregivers and a teacher or other school professional regarding core symptoms of ADHD in various settings, age of onset, duration of symptoms, and degree of impairment. Assessment for co-existing conditions: learning and language problems, aggression, disruptive behavior, depression or anxiety.

24
Assessment Tools No test available Dx by: Observation Rating Scales Vanderbilt Conner’s SNAP

25
How do we treat ADHD? Medication Differences Dosages Timing Side-effects Efficacy Behavior Modification

26
Types of Medications Methylphenidate Dextroamphetamine Atomoxetene Dexmethylphenidate Antidepressants SSRI’s Tricyclics

27
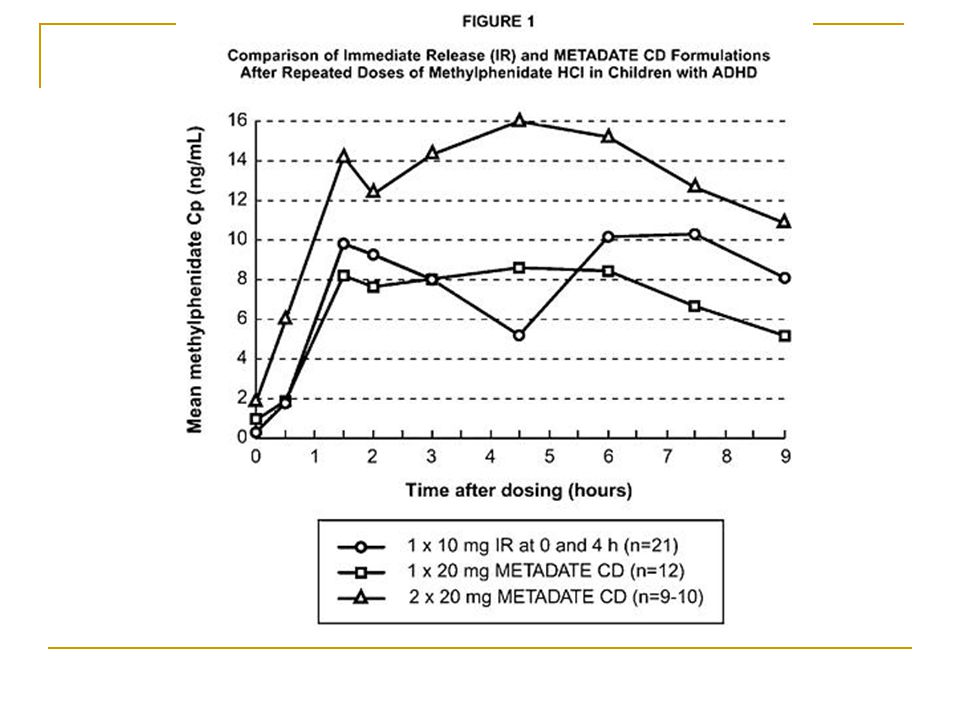
Basic Elements of Methylphenidate Known as: Ritalin, Ritalin SR, Ritalin LA, Concerta, Metadate ER, Metadate CD, Focalin Pharmacology: It is a CNS stimulant, which is chemically related to amphetamine Preparations – 5, 10, 20 mg tabs; sustained release 20 mg tabs; LA 20, 30, and 40 mg capsules. The SR tablet should be swallowed and not crushed or chewed. Concerta comes in 18 and 36 mg extended release tablets. Metadate CD 20 mg capsules; Metadate ER 10 – and 20 – mg tabs. Focalin 2.5, - 5-, 10 - mg tabs.

28
Methylphenidate, cont’d Half-Life – 3-4 hours; 6-8 hours for sustained release It’s a schedule II controlled substance, requiring a triplicate prescription Pre-Drug Work-Up Blood pressure and general cardiac status baseline and periodic blood counts and liver function tests Weight and growth should be monitored in children

29
Methylphenidate, cont’d Adverse Drug Reactions Nervousness and insomnia; can be reduced by decreasing dose. Cardiovascular – Hypertension, tachycardia, and arrhythmias. CNS – Dizziness, euphoria, tremor, headache, precipitation of tics and Tourette’s syndrome, and rarely psychosis. GI – Decreased appetite, weight loss. Case reports of elevated liver enzymes and liver failure. Hematological –Leukopenia and anemia have been reported Growth Inhibition

30
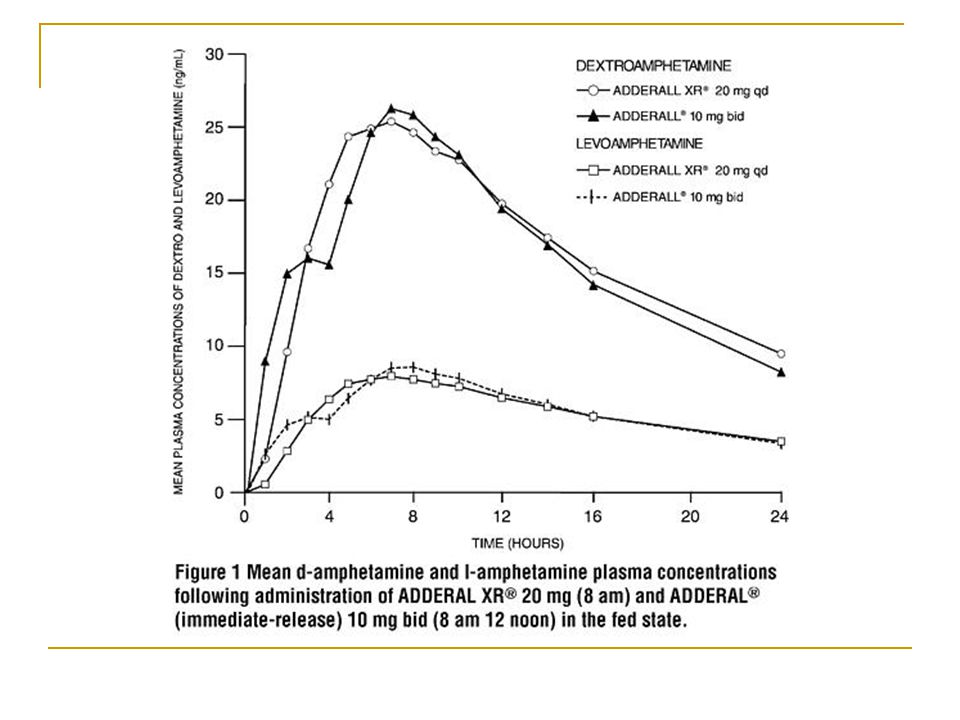
Basic Elements of Dextroamphetamine Known as: Adderall, Adderall XR Pharmacology:causes the release of norepinepherine from neurons. At higher doses, it will also cause dopamine and serotonin release Preparations – Adderall 5-, 7.5-, 10-, 12.5-, 15-, 20-, 30-mg tablets; Adderall XR 5-, 10-, 15-, 20-, 25-, 30-mg capsules.

31
Dextroamphetamine, cont’d Half-Life – 10-25 hours It’s a schedule II controlled substance, requiring a triplicate prescription Pre-Drug Work-Up Blood pressure and general cardiac status should be evaluated prior to initiating dextroamphetamine. Can precipitate tics Contraindicated in in patients with hypertension, hyperthyroidism, cardiac disease or glaucoma. It is not recommended for psychotic patients ot patients with a history of substance abuse. Weight and growth should be monitored in all children.

32
Dextroamphetamine, cont’d Adverse Drug Reactions Side effects – most common side effects are psychomotor agitation, insomnia, loss of appetite, and dry mouth. Tolerance to loss of appetite tends to develop. Effect on sleep can be reduced by making sure no drug is given after 12 pm. Cardiovascular – Palpitations, tachycardia, increased blood pressure. CNS – Dizziness, euphoria, tremor, precipitation of tics, Tourette’s syndrome, and rarely, psychosis. GI – Anorexia and weight loss, diarrhea, constipation. Growth inhibition

33
Basic Elements of Atomoxetene Known as: Strattera Pharmacology:works via presynaptic norepinepherine transporter inhibition Preparations – 10, 18, 25, 40, and 60 mg capsules.

34
Atomoxetene, cont’d Half-Life – approximately 4 hours Not a schedule II controlled substance Clinical Guidelines – Dividing the dose may reduce some side effects Dose reductions are necessary in presence of moderate hepatic insufficiency Atomoxetine should not be used within 2 weeks of discontinuation of a MAO inhibitor. Atomoxetine should be avoided inpatients with narrow angle glaucoma and, it should be used with caution in patients with tachycardia, hypertension, or cardiovascular disease. It can be discontinued without taper. Pregnancy C category.

35
Atomoxetene, cont’d Adverse Drug Reactions Cardiovascular – increased blood pressure and heart rate (similar to those seen with conventional psychostimulant). BI – Anorexia, weight loss, nausea, abdominal pain. Miscellaneous – Fatigue, dry mouth, constipation, urinary hesitancy and erectile dysfunction.

36
Basic Elements of Dexmethylphenidate Known as: Focalin, Focalin XR Pharmacology:causes the release of dopamine from neurons. Is an isomer of Ritalin. Preparations – Focalin 2.5, 5,10-mg tablets; Focalin XR 5-, 10-, 20-mg capsules.

37
Dexmethylphenidate, cont’d Half-Life – 2.2 hours It’s a schedule II controlled substance, requiring a triplicate prescription Pre-Drug Work-Up Blood pressure and general cardiac status should be evaluated prior to initiating Dexmethylphenidate. Can precipitate tics Contraindicated in in patients with hypertension, hyperthyroidism, cardiac disease or glaucoma. It is not recommended for psychotic patients or patients with a history of substance abuse. Weight and growth should be monitored in all children.

38
Dexmethylphenidate, cont’d Adverse Drug Reactions Side effects – most common side effects are psychomotor agitation, insomnia, loss of appetite, and dry mouth. Tolerance to loss of appetite tends to develop. Effect on sleep can be reduced by making sure no drug is given after 12 pm. Cardiovascular – Palpitations, tachycardia, increased blood pressure. CNS – Dizziness, euphoria, tremor, precipitation of tics, Tourette’s syndrome, and rarely, psychosis. GI – Anorexia and weight loss, diarrhea, constipation. Growth inhibition

42
Release Characteristics ConcertaMetadate CD Ritalin LA Immediate Release 22%30%50% Delayed Release 78%70%50% TechnologyOrosEurandSODAS

43
Other Medications Dexadrine Cylert Since marketing in 1975, 13 cases of acute hepatic failure have been reported to the FDA. 11 resulted in death or transplant. Attenade Paxil Wellbutrin Zoloft Trileptal Celexa/Lexapro Effexor

44
When to use, when to change Side effects Past history Substance abuse Efficacy Onset time Stimulant first line, Strattera second Follow MD

45
Closing Thoughts Stimulants still first line defense Look at choice of drug based upon time of release Be aware of study sponsor Addictive nature Subscribe to Medscape

46
Behavior Modification Classroom Home Basics of Behaviorism

47
Steps in Behavior Modification Identify behavior Chart behavior for baseline Identify motivators Establish realistic goals Match motivators with behavior changes Short term Long term Implement Plan Evaluate Plan Modify and repeat

48
Measurable/Realistic Goal Measurable Long term and Short Term Goals Who will measure? What is the goal? Where is the behavior now? When will we measure? How will we measure?

49
Consequences RewardPunishment Positive ↑ behavior by ‘+‘ something ↓ behavior by ‘+‘ something Negative ↑ behavior by ‘-‘ something ↓ behavior by ‘-‘ something

50
Consequences examples RewardPunishment Positive Add TV time when no hitting Add chores when there is hitting Negative Take away chore when there is no hitting Take away toy when there is hitting

51
Other Behavior Therapy techniques Token Economy Time outs

52
Classroom Rewards Homework reductions Physical Contact Computer Access Additional recess Free time in class Tickets/stickers Time to finish homework in class Special pen or paper

53
Helping a child control his behavior Daily Schedule Cut down distractions Organize your house Set small, reachable goals Limit choices Use calm discipline - distraction

54
Tools/Resources ADD/ADHD Behavior-Change Resource Kit Teenagers with ADD: A Parents’ Guide www.myadhd.com www.adhdhelp.com www.amenclinic.com ADDitude Magazine

55
References American Academy of Pediatrics. Diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. Pediatrics. 2000;105:1158-1170. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-IV-TR. In: Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence: Diagnostic Criteria for Attention-Deficit/Hyperactivity Disorder. Washington, DC: American Psychiatric Association; 1994:92-93. National Institute of Mental Health. National Institutes of Health. Attention deficit hyperactivity disorder. Available at: http://www.nimh.nih.gov/publicat/helpchild.cfm. Accessed April 19, 2002. U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General. Available at: http://www.surgeongeneral.gov/library/mentalhealth/chapter3/sec4.html. Accessed April 19, 2002. Dulcan M. Practice parameters for the assessment and treatment of children, adolescents, and adults with attention- deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 1997;369(suppl):855-1215. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-IV-TR. In: Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence: Diagnostic Criteria for Attention-Deficit/Hyperactivity Disorder. Washington, DC: American Psychiatric Association; 1994:92-93. National Institute of Mental Health. National Institutes of Health. Attention deficit hyperactivity disorder—questions and answers. Available at: http://www.nimh.nih.gov/publicat/adhdqa.cfm. Accessed April 19, 2002. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000. Fauman, M. A. (2002). Study Guide to DSM-IV-TR. Washington, DC: American Psychiatric Publishing, Inc.
: American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-IV-TR. In: Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence: Diagnostic Criteria for Attention-Deficit/Hyperactivity Disorder. Washington, DC: American Psychiatric Association; 1994: National Institute of Mental Health. National Institutes of Health. Attention deficit hyperactivity disorder—questions and answers. Available at: Accessed April 19, American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, Fauman, M. A. (2002). Study Guide to DSM-IV-TR. Washington, DC: American Psychiatric Publishing, Inc..")
Similar presentations





>")
 By: Bianca Jimenez Period:5.>")
. Diagnostic and.>")

 is one of the most common childhood disorders and can continue.>")

/ Attention Deficit Hyperactivity Disorder (ADHD) A condition of the brain that makes it difficult for children to control.>")




 Kiefer, MaryJane ED 6362 – Education of Exceptional Children Dr. M. McCloulskey Fall 2001.>")



