Download presentation
Presentation is loading. Please wait.

1
CARE PATIENT ON RESPIRATORY SUPPORT
Presentor : chua mei yin Moderator : dr. mohd ridhwan mohd nor

2
Protocols + Checklist + Physician’s Rounds

3
PLAY THE IMPORTANT ROLES !!
Reduce errors Encourages teamwork Help improves the quality of care received by intensive care patient

4
Outline of presentation
Goal Review communications Check ventilator settings & mode Care of ETT General Care - FAST HUG - FAST HUGSBID Oral, Eyes & Skin Care Sleep Radiation Physiotherapy Monitoring Infection control Educate patient & family

5
Goals of Monitoring & Managing the ventilated patient
Ensure proper airway Ensure adequate oxygenation & ventilation Maintain hemodynamic stability Interpretation of Ventilator alarms &troubleshooting Prevent infection Prevent complications related to bedridden state

6
REVIEW COMMUNICATIONS

7
1) Communication among care providers ~ Promotes optimal outcome ~ Find out the goal of the therapy for patient ~ Indication for mechanical ventilation ~ Indication for icu admission ~ Do-not–resuscitate status 2) Communication with the patient ~ Provide writing tools or a communication board so pt can express her needs
 Communication among care providers ~ Promotes optimal outcome ~ Find out the goal of the therapy for patient ~ Indication for mechanical ventilation ~ Indication for icu admission ~ Do-not–resuscitate status 2) Communication with the patient ~ Provide writing tools or a communication board so pt can express her needs")
8
Check Ventilator Settings & Modes
Read patient order & obtain in formation about the ventilator. Familiarize with ventilator alarms and the actions to take when an alarm sounds. Keep resuscitation bag at bedside Know how to hyperventilate & hyperoxygenate patient. Provides/restore adequate ventilation when patient or equipment problems require patient removed from ventilator.

9
Check following settings: Respiratory rate
Fraction of inspired oxygen ( fio2) Tidal volume Peak inspiratory pressure (PIP) Ventilator mode of patient: Ventilator itself Respiratory flow sheet PIP – the pressure needed to provide each breath. Target below 30cm H20. High indicate a kinked tube, need for suctioning, bronchospasm,e.g. pulmonaryh edema or pneumothorax.
 Tidal volume. Peak inspiratory pressure (PIP) Ventilator mode of patient: Ventilator itself. Respiratory flow sheet. PIP – the pressure needed to provide each breath. Target below 30cm H20. High indicate a kinked tube, need for suctioning, bronchospasm,e.g. pulmonaryh edema or pneumothorax.")
10
Care of ETT Ensuring correct position Securing the tube Measuring cuff pressure Suspecting leak Suspecting tube blockade Suctioning

11
Size of ETT mm for mm for Larger ETT in Asthma, COPD Tube position, confirmed by: Clinical examination 5 point auscultation CXR Etco2

12
Cuff pressure keep < 25mmHg - Inflate cuff to seal - lowest pressure that seal or low leak Every nursing duty check cuff pressure If partial block is suspected. change ETT **ETT with subglottic suction port- reduced incidence of VAP RCT High cuff pressure ( > 25 cm H20) affect ciliary Function & cause mucosal ischaemia.
 affect ciliary. Function & cause mucosal ischaemia.")
14
SUCTIONING General suctioning recommendation:
Suction only as needed –not according to a schedule. Hyperoxygenate the patient BEFORE & AFTER suctioning to help prevent O2 desaturation Don’t instill normal saline into the ETT in an attempt to promote secretion removal 2004 American Association for respiratory care CPG Limit suctioning pressure to the lowest level needed to remove secretions Suction for the shortest duration possible

15
Type of suction Open suction Closed suction

16
Occlude catheter while passing in
Fresh cathether with every use Preoxygenate with 100% o2 Suction cycle < 20s Occlude catheter while passing in Once obstruction is encountered withdraw slightly & suck while coming out Repeat if required Open suction

18
Closed suction Use in hypoxic patient ( FiO2 >0.6), PEEP > 10
MDR infections

19
** Combine suction with physiotherapy & postural drainage
Monitor BP, HR,SPO2 &Arryhtmias

20
GENERAL CARE FAST HUG FAST HUGS BID

21
F A S T H U G

22
FAST HUG A simple, short mneumonic to highlights some keys aspects in the general care of all critically ill patients. Should be considered at least once a day during rounds Can be used as mental checklist when individual staff members attending the patients.

23
GENERAL CARE F = Feeding A = Analgesic S = Sedation T = Thromboembolic prophylaxis H= Head- of- bed elevation U= Stress Ulcer prevention G= Glucose control

24
F = Feeding

25
Malnutrition increases complications & worsens outcomes of critically ill patients. In general, kcal/kg/day is acceptable & achievable target intake. Should started early , preferably within 24-48hrs icu admission. Optimal constituents of feeding solutions remain under debate.

26
A = Analgesic Pain can effect patient’s psychological & physiological recovery. Critically ill pt feel pain due not only to their illness but also routine procedures e.g. turning, suctioning& dressing changes. One study of 5957 patients , > 63% received no analgesic before painful procedure.

27
How to assess pain in critically ill patients?
Subjective measures of pain- related behaviours ~ facial expression, movement Physiologic indicators ~ Heart rate, blood pressure > 5 indicate of pain

29
Pharmacological therapies to relieve pain included:
opioids non opioids Continuous infusion of analgesic drugs or regularly administered doses are more effective than bolus doses given as “needed” I.V. administration of analgesic allows closer and more rapid titration to patients needs than I.M. or subcutaneous administration. Care should be taken to ensure analgesic is adequate but not excessive.

30
S = Sedation No rules governing how much to give & how often.
Sedative administration must be titrated individual. CCC ( Calm, comfortable and collaboration) rule help to determine whether patients are appropriately sedated. Daily discontinuation of sedation may reduce the length of ICU stay & the need for imaging procedures Kress et al
 rule help. to determine whether patients are appropriately. sedated. Daily discontinuation of sedation may reduce the. length of ICU stay & the need for imaging procedures. Kress et al.")
32
-2 to +1

33
T = Thromboembolic prophylaxis

34
T – Thromboembolic Prophylaxis
Still underused because is still often forgotten and yet mortality & morbildity rates a/w thromboembolism are considerable & can be reduce by prophylaxis. Among patients who do not received prophylaxis, objectively confirmed rate of DVT range between %. It has thus recommended all patients received at least s/c heparin unless CI.

35
The most effective method of prophylaxis still unclear
The most effective method of prophylaxis still unclear. The benefit of prophylaxis must be weighed against the risk of complications.

37
H= Head- of- bed elevation

38
Several studies demonstrated that having the head of
bed inclined at 45 degrees can decrease the risk incidence of gastroesophageal reflux. Patient nurses in semirecumbent reduce rate of nosocomial pneumonia. A randomised trial. Lancet 1999 Raising the head of the bed may not be enough, because patients especially when sedated might slides down in the bed. Attempts must be made to keep head of bed & thorax elevated.

39
U= Stress Ulcer prevention
Stress ulcer prevention is important notably for patients who are at risk of developing stress- related gastrointestinal hemorrhages. The optimal medication is still not clear. In 1200 critically ill patients undergoing mechanical ventilation, those treated with ranitidine had significantly lower rates of clinically significant GI bleeding than patients treated with sucralfate although there was no difference in the mortality rates between two groups. Multicenter study by Cook et al

41
G= Glucose control

42
Many units now aim to keep blood sugar levels below
8.3 mmol/L as recommended guidelines for the management of severe sepsis & septic shock. Keeping blood glucose levels < 7.8 mmol/L resulted in 29.3% decrease in hospital mortality rates & 10.8% reduction in length of ICU stay. Krinsley

43
FAST HUGSBID S = Spontaneous Breathing Trial B = Bowel Care I = Indwelling Catheter removal D = De-escalation of Antibiotitcs

44
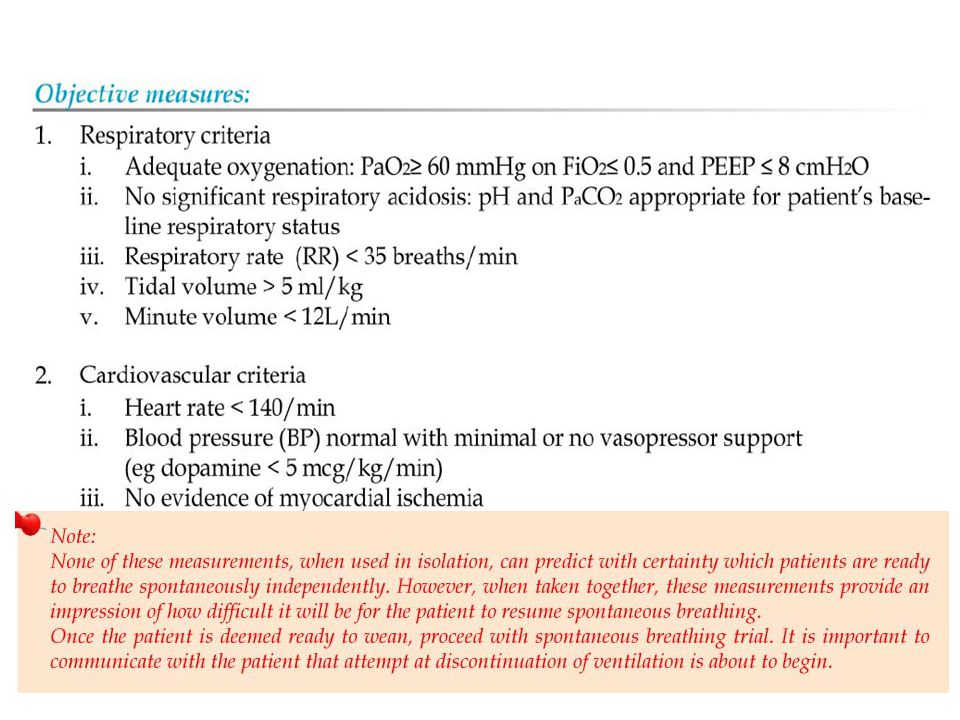
S = Spontaneous Breathing Trial
Daily assessment of SBT has been show to be a safe, effective & highly predictive method for determining which pt will tolerate ventilator separation. Prolonged mechanical ventilation a/w increased rate VAP & in hospital & total mortality. Should be considered at least daily & performed in highly protocolized fashion by well-trained team of nurses & respiratory therapist.

45
WEANING: Readiness All ventilated patients must have “ readiness criteria” evaluated daily ( after discontinuing sedation)
")
49
YES

50
During weaning trial all patient must be observed
Closely to identify the existence of “ distress” High RR Respiratory patern ( paradox, nasal flaring) Low VT Drop in O2 saturation < 90% Increased hr ( > 20% from baseline) Anxiety, agitation, diaphoresis Somnolence
 Low VT. Drop in O2 saturation < 90% Increased hr ( > 20% from baseline) Anxiety, agitation, diaphoresis. Somnolence.")
51
B = Bowel Care

52
B = Bowel Care Disorders of GI motility, including ileus, constipation & diarrhoea are common in critically ill patient & may contribute to additional disease burden. Institutional guidelines & use of standardized definitions of constipation & diarrhoea may facilitate bowel dysfunction management. Routine assessment & tx to maintain normal bowel function should be conducted in all critically ill patients.

53
I = Indwelling Catheter removal
Indwelling catheter including urinary, arterial, central venous, pulmonary artery & dialysis catheters are commonly used in critically ill patients. Because they penetrate through body’s natural protective mechanism, they are at risk for local & systemic infection. Early discontinuation & removal, when these catheters are no longer needed, remains an important strategy to combat catheter-associated infections.

54
Daily more frequent) assessment should be performed of the ongoing need for these catheters, and their removal, when not medically necessary.
 assessment should be performed of the ongoing need for these catheters, and their removal, when not medically necessary.")
55
D = De-escalation of Antibiotitcs/Streamlining
Once a pathogen has been identified & antimicorbial susceptibilities have been reported, the regime should be converted to most narrow-spectrum, cost effective& pathogen specific antibiotic. Minimizes exposure to broad-spectrum antimicrobial therapy. Same principles can be applied to other pharmacologic treatments which should be regularly re-evaluated for appropriate indications to minimize risk of adverse effects & medications errors.

56
Oral, Eyes & Skin care

57
Oral Care preferably 8 hourly Remove oral airway
Move ET tube to opposite corner Clear mouth of all secretions Paint mouth with 2% chlorhexidine ** Reduces rates of VAP

58
Eye Care Moisol eyes drop Tape both eyes in paralysed pt
Appropriate antibiotic drops

59
Skin Care Daily Bath makes patient comfortable & fresh
improves circulation Observe skin daily for redness, injuries, swelling, rashes or other infections & bony prominences for bed sore. Cut short the finger & toe nails Hair care- Shampoo as required Back care- Apply olive oil from shoulders to buttocks with brisk circular movement

60
SLEEP IN ICU Cause of sleep deprivation in ICU: Environmental factors
Pathophysiological factors

61
Enviromental factors Noise Lighting practices Pt care activities Diagnostic procedures Sedatives Analgesics

62
Pathophysiological factors
Stress Organ dysfunction Inflammatory response Pain Psychosis

63
Integrated strategy to promote sleep in the
intensive care unit: Noise reduction ( < 50dB) Diurnal lighting practices Use of sleep- promoting pharmacologic agent Minimizing use of pharmacologic agents inhibiting sleep Uninterrupted time for adequate sleep Appropriate physiologic support Active promotion of patient orientation Patient- ventilator synchrony Relaxation techniques
 Diurnal lighting practices. Use of sleep- promoting pharmacologic agent. Minimizing use of pharmacologic agents inhibiting sleep. Uninterrupted time for adequate sleep. Appropriate physiologic support. Active promotion of patient orientation. Patient- ventilator synchrony. Relaxation techniques.")
64
RADIATION

65
A daily CXR is indicated for pt with acute
cardiopulmonary problems & for patients on mechanical ventilation. In pt with a central venous catheter, a Swan- Ganz catheter, Feeding tube, chest tube placement, only post procedure radiographs indicated. Stable cardiac monitoring pt & those with purely extrathoracic disease require only admission films upon entry to ICU, unless clinical condition demands. American College Of Radiology

66
PHYSIOTHERAPY Specialized job Round the clock
Continuum from preventing respiratory failure, to managing pt on ventilator to pt who have been weaned Prevented complications related to MV Percussion, vibration, change of position, postural drainage ,suction for chest physiotherapy Limb physiotherapy

67
MONITORING

68
VENTILATION OXYGENATION HEMODYNAMIC URINE OUTPUT ABG

70
Infection Control Measures
Control of the reservoirs of infection Interruption of the transmission of bacteria from person to person Individual device related measures Staff education Surveillance Regular audit

71
Control of the reservoirs of infection
Disinfection of pt area/bay between pt ( include bed, monitor, ventilator, other equipment, furniture, floor , walls) Appropriate sterilization of reusable equipment Appropriate disposal of disposable equipment including sharps Appropriate surveillance of personnel as reservoirs.
 Appropriate sterilization of reusable equipment Appropriate disposal of disposable equipment including sharps Appropriate surveillance of personnel as reservoirs.")
72
Cross contamination Put on gloves before handling respiratory contaminated objects. Wash hands with soap & water or an alcohol- based antiseptic hand rub before & after contact with mucous membrane, respiratory secretions, or contaminated objects and before and after contact with pt with respiratory device. Wear gown when you anticipate being soiled with respiratory secretions and change it before caring for another patient.

73
Between their uses on different patients, sterilize or subject to high-level disinfection reusable hand- powered resuscitation bags ( AMBU)
")
74
In addition to routine hand hygiene the following should also be considered in ventilated pt: Intubation: If elective- standard handwash + sterile gloves Emergency – handrub + sterile gloves Suctioning : Alcohol hand rub before & after procedure Clean glove Bronch: Surgical hand/forearm scrub Full sterile field, gown & gloves. Always consider masks, splash guard & eyewear ( PPE) Full chlorhexidine handwash if accidental exposure to secretions.
 Full chlorhexidine handwash if accidental exposure to secretions.")
76
Educate family & patient
Seeing a loved one attached to mechanical ventilation frightening. To ease distress in pt & family, teach them why mechanical ventilation is needed & emphasize the positive outcomes it can provide. Explain what you are doing Communicate desired outcomes so the patient & family can actively participate in the plan of care.

78
REFERENCE Give your patient a fast hug ( at least) once a day Jean- Louis Vincent, MD, PhD,FFCM [PPT] Care of the ventilated patient: FAST HUG-SBID Critically ill patients need “FAST HUGS BID” ( an update mnemonic) Top 10 Care Essentials for ventilator Patients Evidence-based Interventions and Teamwork are crucial when caring for patients on Mechanical Ventilators, Laura C. Parker,MSN,RN,CCRN
![REFERENCE Give your patient a fast hug ( at least) once a day Jean- Louis Vincent, MD, PhD,FFCM. [PPT] Care of the ventilated patient: FAST HUG-SBID.](http://slideplayer.com/slide/4106493/13/images/78/REFERENCE+Give+your+patient+a+fast+hug+%28+at+least%29+once+a+day+Jean-+Louis+Vincent%2C+MD%2C+PhD%2CFFCM.+%5BPPT%5D+Care+of+the+ventilated+patient%3A+FAST+HUG-SBID..jpg "Critically ill patients need FAST HUGS BID ( an update mnemonic) Top 10 Care Essentials for ventilator Patients. Evidence-based Interventions and Teamwork are crucial when. caring for patients on Mechanical Ventilators, Laura C. Parker,MSN,RN,CCRN.")
80
Thromboembolic prevention
COMPONENT CONSIDERATIONS Feeding Can the patient be fed orally, if not enterally? If no, should we start parenteral feeding? Analgesia The patient should not suffer pain, but excessive analgesia should be avoided Sedation The patient should not experience discomfort but excessive sedation should be avoided; ‘calm, comfortable, collaborative” Thromboembolic prevention Should we give low-molecular weight heparin or use mechanical adjuncts Head of the bed elevated Optimally , 300 to 450 ,unless contraindications e.g. threatened cerebral perfusion pressure Stress ulcer prophylaxis Usually H2 antagonist: sometimes proton pump inhibitors Glucose control Within limits defined in each ICU

Similar presentations













>")
















>")
