Download presentation
Presentation is loading. Please wait.

1
Diabetes, a weighty issue: do recent insights inform clinical management?” Naveed Sattar Professor of Metabolic Medicine BHF GCRC, University of Glasgow & Hon Consultant Clinical Biochemistry Glasgow Royal Infirmary

2
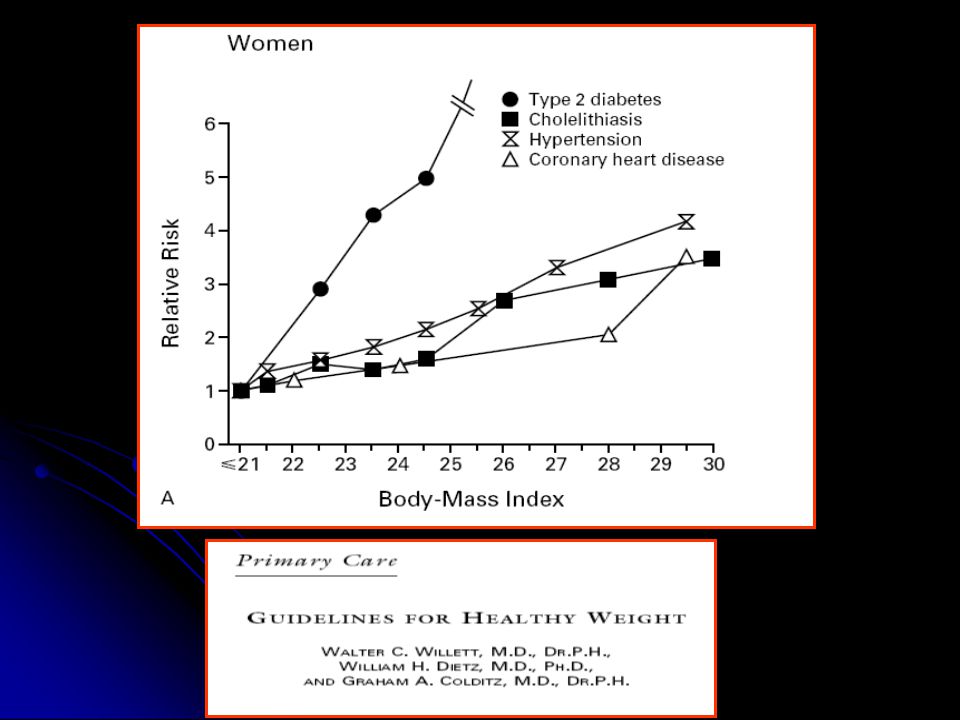
Which disease process is more closely linked to obesity?

4
Chan JM et al. Diabetes Care 1994; 17: 961–969. BMI Risk of Type 2 diabetes 60 23–23.9 < 23 24–24.925–26.927–28.929–30.931–32.933–34.9 > 35 0 50 40 30 20 10 OVERWEIGHTOBESE Weight gain pulls trigger

5
Yearly diabetes prevalence 1995-2005 Ontario Canada Lipscombe & Hux Lancet 2007

6
1. UKPDS Group. Diabetes Res 1990; 13: 1–11. 2. The Hypertension in Diabetes Study Group. J Hypertens 1993; 11: 309–317. Type 2 diabetes – the microvascular burden at diagnosis a decade or so ago Erectile dysfunction 1 20% Retinopathy 1 21% Neuropathy 1 12% Nephropathy 2 18%

7
How does obesity alter presentation of Diabetes?

8
Age of onset of type 2 Diabetes Adapted from Hillier & Pedula, 2001

9
Less well known risks of Obesity?

10
Medical Complications of Obesity Phlebitis venous stasis Coronary heart disease Pulmonary disease abnormal function obstructive sleep apnea hypoventilation syndrome Gall bladder disease Gout Diabetes Osteoarthritis Nonalcoholic fatty liver disease steatosis steatohepatitis cirrhosis Hypertension Dyslipidemia Cataracts Skin Pancreatitis Idiopathic intracranial hypertension Cancer breast, uterus, cervix, prostate, kidney colon, esophagus, pancreas, liver Gynecologic abnormalities abnormal menses/ infertility polycystic ovarian syndrome Numerous pregnancy comps. Stroke

11
Populations more susceptible to adverse effects of weight gain?

12
Razak et al (2007) Circulation Glucose, 2 hr glucose, insulin, HBA1c, FFAs
 Circulation Glucose, 2 hr glucose, insulin, HBA1c, FFAs")
13
Mukhopadhyay*, Forouhi*, Fisher, Kesson, Sattar. Diab Med 2005 Whites n=1557 South Asians n=210 Age at diagnosis 57 46 BMI 30 28.7

14
Case 1 Pakistani Male, Pakistani Male, Non-smoker Non-smoker Trigs 3.2, chol 6.0, HDL-chol 0.8, FBG 5.9 Trigs 3.2, chol 6.0, HDL-chol 0.8, FBG 5.9 HBA1c 6.4% HBA1c 6.4% OGTT = type 2 DM OGTT = type 2 DM Aged 31, 70Kg = BMI 23 Aged 31, 70Kg = BMI 23 “Sattar family history” “Sattar family history” Gun well and truly loaded! Gun well and truly loaded!

15
Obesity to Diabetes – concept of ectopic fat…. Or “fat in wrong places”

16
Most fat is healthy Who has most fat? Who has most fat? Women Women More SC fat More SC fat Lower CHD & T2DM risk Lower CHD & T2DM risk Consider 100kg man Consider 100kg man Total fat ~35kg Total fat ~35kg 70-75% will be Subcutaneous 70-75% will be Subcutaneous 10-15% Visceral fat 10-15% Visceral fat 10-15% elsewhere (E) 10-15% elsewhere (E)
 10-15% elsewhere (E).")
17
Subcutaneous GOOD But if storage capacity exceeded Or diminished VF E (0.5-6kg) Waist size up Ethnicity Genes/ Programming Illness These sites empty quicker 5% weight loss (100kg man) ~ 30% VF loss Ectopic fat Liver, muscle Elsewhere
 Waist size up Ethnicity Genes/ Programming Illness These sites empty quicker 5% weight loss (100kg man) ~ 30% VF loss Ectopic fat Liver, muscle Elsewhere")
18
Glucose Output Glucose GlucoseUptake VF Excess fat also accumulates in liver and muscle When safe stores overwhelmed Glucose Insulin Excess calories SC stores full 1 2 3 4 IR

19
glucose Production (FBG) fat cells larger Fat accumulation in liver – what signs? LiverEnzymesALTGGT trigs Sattar et al (2007) Diabetes Overweight Exapanding waist Insulin resistance Calorie excess
 Diabetes Overweight Exapanding waist Insulin resistance Calorie excess.")
20
Conc.U/L No.of Metabolic Abnormalities P = 0.27 P = <.0001 waist >102cm, high trig, low HDL-C Blood pressure, glucose>6.1 20 21 22 23 24 25 26 27 28 29 ASTALT 0 1 2 3 >= 4 Sattar et al, Diabetes (2004)
")
21
Liver fat vs. alcohol ALT > AST ALT > AST GGT high GGT high Overweight Overweight Glucose high normal Glucose high normal HDL-C often low HDL-C often low AST>ALT AST>ALT MCV high MCV high HDL-C higher than expected! HDL-C higher than expected! Not necessarily overweight or high glucose Not necessarily overweight or high glucose Preiss & Sattar Clinical Science 2008

22
Unselected population (100%) NASH (2-3% of total) Steatosis (20-30% of all) Cirrhosis ?% HCC ?% 12% may progress over 8 years [7] 1-2% may progress over 15-20 years The spectrum of NAFLD Preiss & Sattar Clinical Science 2008
![Unselected population (100%) NASH (2-3% of total) Steatosis (20-30% of all) Cirrhosis % HCC % 12% may progress over 8 years [7] 1-2% may progress over years The spectrum of NAFLD Preiss & Sattar Clinical Science 2008](http://images.slideplayer.com/13/4103756/slides/slide_22.jpg "Unselected population (100%) NASH (2-3% of total) Steatosis (20-30% of all) Cirrhosis % HCC % 12% may progress over 8 years [7] 1-2% may progress over years The spectrum of NAFLD Preiss & Sattar Clinical Science 2008")
23
How does excess fat in tissues lead to higher glucose levels? Basic mechanisms

24
Glycogen glucose release Petersen & Shulman Am J Med 2006 gluconeogenesis gluconeogenesis X X

25
Case one - Mr RB Age 42, BMI 32 Referred lipid disorder risk factor clinic Abnormal LFTs (ALT> AST) 2 0 to statin therapy? Prior Hx – type 2 DM, Tg 3.95, Chol 6.65, HDL-C 0.70, Previously erectile dysfunction & sleep apnoea clinics

26
LFTs ALT 137, AST 69 (TGs, low HDL-C, obese) ALT 137, AST 69 (TGs, low HDL-C, obese) Pattern and Hx not c/w alcohol Pattern and Hx not c/w alcohol Liver US 2 years before – echogenicity of parenchymal liver Liver US 2 years before – echogenicity of parenchymal liver Fatty liver – Confirmed – cautiously restart statin Fatty liver – Confirmed – cautiously restart statin
 ALT 137, AST 69 (TGs, low HDL-C, obese) Pattern and Hx not c/w alcohol Pattern and Hx not c/w alcohol Liver US 2 years before – echogenicity of parenchymal liver Liver US 2 years before – echogenicity of parenchymal liver Fatty liver – Confirmed – cautiously restart statin Fatty liver – Confirmed – cautiously restart statin")
27
Mr RB - some recent improvement Increased activity Increased activity Plays football twice per week; walks dog Plays football twice per week; walks dog 2 inches from waist 2 inches from waist Feels better, sleep pattern improved Feels better, sleep pattern improved

28
Case History #2 Mrs Smith Mrs Smith BMI 28, T2DM BMI 28, T2DM ALT 45, AST 24, GGT 66 ALT 45, AST 24, GGT 66 Trigs 4.5 mmo/l, HDL-C 1.0 mmol/l, TC 5.6 mmol/l Trigs 4.5 mmo/l, HDL-C 1.0 mmol/l, TC 5.6 mmol/l ALTs beyond ~20 U/l in women – potentially abnormal ALTs beyond ~20 U/l in women – potentially abnormal

29
Evidence for role of liver fat in conversion to diabetes? Forwards Forwards Backwards Backwards Major weight loss Major weight loss

30
WHICH PARAMETERS ACCOMPANY SHORT CONVERSION TO DIABETES? * * -5% 0% 5% 10% 15% 20% 25% 30% 35% Glucose ALT AST Chol Trig HDL -C Weight SBP DBP Albumin WCC 5.9 to 7.7 mmol/l SUSTAINED but not transient ALT elevations associated with incident T2DM Sattar et al (2007) Diabetes
 Diabetes.")
31
Keeping liver fat down? Petersen et al Diabetes. 2005 N=8 subjects with diabetes - Hypocaloric low fat diet (3%) Wt 86 to 78 kg Glucose 8.8 to 6.6 mmol/l Insulin 174 to 66 pmol/l Percent fat 12% to ~2%
 Wt 86 to 78 kg Glucose 8.8 to 6.6 mmol/l Insulin 174 to 66 pmol/l Percent fat 12% to ~2%.")
32
High fibre strongly predictive of lower diabetes risk via lower ALT (liver fat) levels (unpublished data)
 levels (unpublished data)")
33
Ectopic fat summary Diabetes unmasked by excess weight gain Diabetes unmasked by excess weight gain if family Hx, South Asian, at lower BMI if family Hx, South Asian, at lower BMI weight leads to ectopic fat weight leads to ectopic fat Expanding waist good sign of ectopic fat Expanding waist good sign of ectopic fat Earlier in susceptible (at risk) individuals Earlier in susceptible (at risk) individuals Ectopic fat makes organs insulin resistant Ectopic fat makes organs insulin resistant Signs of excess ‘ectopic’ liver fat common Signs of excess ‘ectopic’ liver fat common
 individuals Earlier in susceptible (at risk) individuals Ectopic fat makes organs insulin resistant Ectopic fat makes organs insulin resistant Signs of excess ‘ectopic’ liver fat common Signs of excess ‘ectopic’ liver fat common")
34
Diabetes risk scores QDS – risk scores for T2DM (2009) BMJ QDS – risk scores for T2DM (2009) BMJ Age, BMI, family history T2DM, ethnicity, hypertension, SES. Age, BMI, family history T2DM, ethnicity, hypertension, SES. Excellent risk prediction Excellent risk prediction Diagnosis of T2DM may alter…. Diagnosis of T2DM may alter…. Add HbA1c to those with high non-lab based diabetes risk score Add HbA1c to those with high non-lab based diabetes risk score

35
Interlude

36
Low down on intensive glucose control

37
Non-fatalMI

38
Summary of findings The mean HbA1C 0·9% Intensive glycaemic control resulted in: 17% non-fatal MI (OR 0·83, 0·75–0·93), 15% CHD events (0·85, 0·77–0·93) No change stroke (0·93, 0·81–1·06) No change total mortality (1·02, 0·87–1·19)
, 15% CHD events (0·85, 0·77–0·93) No change stroke (0·93, 0·81–1·06) No change total mortality (1·02, 0·87–1·19)")
39
All Cause Mortality

40
Risks ACCORD & VADT mortality, but: patients had longest duration since diabetes diagnosis at baseline (≥10 years) had highest baseline HbA1c concentrations greater risk of hypoglycaemia ACCORD – drop of 1.5% in 6 months ADVANCE - drop of 0.5% in 6 months
 had highest baseline HbA1c concentrations greater risk of hypoglycaemia ACCORD – drop of 1.5% in 6 months ADVANCE - drop of 0.5% in 6 months")
41
Benefit of different interventions per 200 diabetic pts treated for 5 years Per 0.9% lower HbA1c Per 4mmHg lower SBP Per 1mmol/ L lower LDL-C Ray et al Lancet 2009

42
Back to obesity

43
Reality: incredibly hard to lose AND sustain weight loss Very hard to lose weight by physical activity alone

44
“Most do not wish to be overweight” Up to half who are obese will not lose weight by any medical method Lean, Gruer, Alberti, Sattar (2006) BMJ
 BMJ")
45
Stanley S et al. Physiol Rev 2005; 85: 1131 Appetite/satiety signals impaired when obese

46
Lean, Gruer, Alberti, Sattar (2006) BMJ
 BMJ")
47
Obesity – public health issue – prevention must be priority Limit “energy dense” foods sat fat, refined sugar Fruit & Veg. fibre…. Snacking – eat more fruit…. Chew etc Less smoothies / fruit juices

48
Treating obesity?

49
Systematic reviews - SIGN Dietary and lifestyle up to 5kg (2-4 yrs) Dietary and lifestyle up to 5kg (2-4 yrs) Drugs 5-10kg (1-2 yrs) Drugs 5-10kg (1-2 yrs) Surgery ~25-75kg (2-4 years) Surgery ~25-75kg (2-4 years) Surgery -21kg vs wt gain conventional at 8 years* Surgery -21kg vs wt gain conventional at 8 years* Cochrane collaboration* Cochrane collaboration*
 Dietary and lifestyle up to 5kg (2-4 yrs) Drugs 5-10kg (1-2 yrs) Drugs 5-10kg (1-2 yrs) Surgery ~25-75kg (2-4 years) Surgery ~25-75kg (2-4 years) Surgery -21kg vs wt gain conventional at 8 years* Surgery -21kg vs wt gain conventional at 8 years* Cochrane collaboration* Cochrane collaboration*")
50
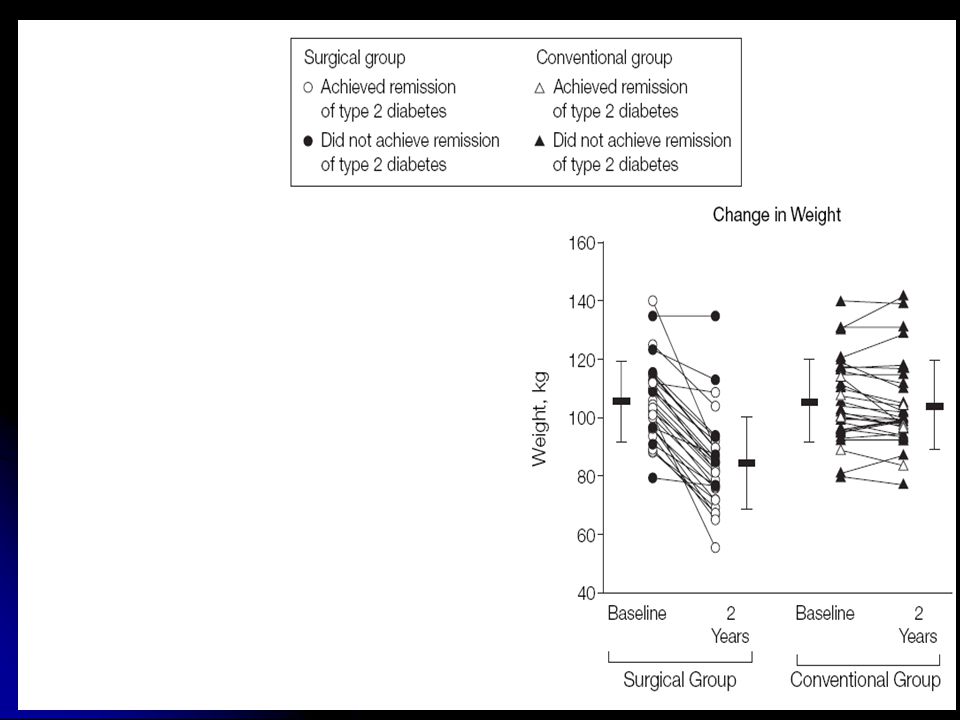
A role for obesity surgery? A new paradigm?

52
“Remission” rates 73% with surgery vs. 13% conventional methods USA: Medicare to cover bariatric surgery for obese patients with type 2 diabetes Feb 2009

53
Personal perspective Wait until obese Wait until obese interventions too late? interventions too late? Serial wt: Serial wt: target rapid gainers much earlier target rapid gainers much earlier Better education at all levels………we all have to try harder in current environment…… Better education at all levels………we all have to try harder in current environment…… time wt

54
Adapted from Rössner, 1992 by U.S. Institute of Medicine, 1995. 1. Sustained weight, no increase. 2. Minor weight loss with dietary change to reduce risk of complications. 3. Weight normalisation: rare Body weight Obese Normal Years of management or intermittent monitoring Overweight Treatment strategies Successes Natural course of further weight gain. What do we tell our patients 50-100kcal per day for weight maintenance

55
Diet, Delusion and diabetes (Jan 2009 Diabetologia) Professional sensitivities add to the confusion, for the diabetes physician, who once knew all there was to be known about diet, is now supremely ignorant about the whole subject. ‘Whereof one cannot speak, thereof one must be silent,’ said the philosopher Wittgenstein Life under communism was once summed up in the wry comment that ‘we pretend to work, and they pretend to pay us’. Our patients might equally complain that we pretend to offer a diet, and they pretend to follow it.

56
Obesity and diabetes clinical pointers Ectopic fat – major feature in T2DM Ectopic fat – major feature in T2DM Try to be sympathetic – most are doing as much as they can….! Try to be sympathetic – most are doing as much as they can….! Patients – emphasise small sustainable changes…or don’t do it at all Patients – emphasise small sustainable changes…or don’t do it at all For some don’t mention weight loss For some don’t mention weight loss Alter trajectory of weight Alter trajectory of weight Future – weight fav. drugs; surgery role? Future – weight fav. drugs; surgery role?

Similar presentations


















![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")
