Download presentation
Presentation is loading. Please wait.

2
PATIENT HISTORY: A 15-year-old girl presented with an ovarian mass.
On exploratory laparotomy, twisted ovarian cyst with appendiceal adhesions was noted. The fallopian tube was dilated with multiple nodules on the surface. She was treated by right oophorectomy followed by chemotherapy (Bleomycin, Etoposide & Cisplatin). After a disease-free interval of 14 months, she presented with a recurrent abdominal mass. She underwent a second exploratory laparotomy for the excision of pelvic soft tissue mass, sigmoid epiploica and portion of the sigmoid colon.
. After a disease-free interval of 14 months, she presented with a recurrent abdominal mass. She underwent a second exploratory laparotomy for the excision of pelvic soft tissue mass, sigmoid epiploica and portion of the sigmoid colon.")
3
GROSS DESCRIPTION: The enlarged ovary measured 16 X 14 X 8 cm and weighed 1020 grams. The cut surface was variegated, with multicystic and solid areas. The cystic areas contained gelatinous dark brown material. The solid areas showed focal areas of necrosis and hemorrhage. The fallopian tube was dilated with numerous cystic nodules, up to 1 cm, on the surface.

4
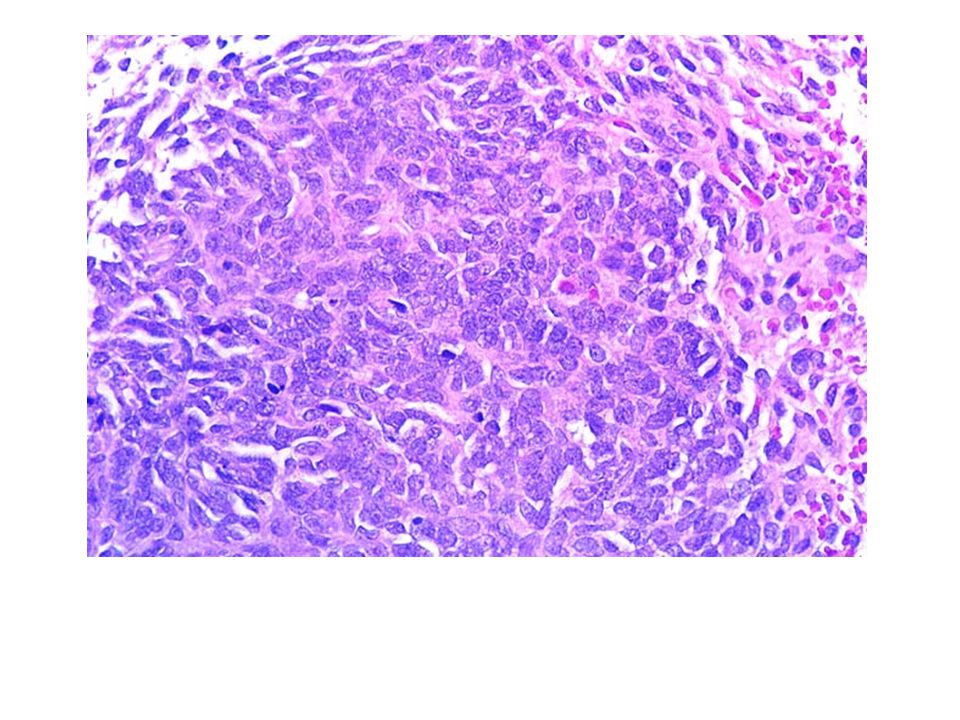
Figure 1 Ovary, focal lobulation of stromal cells with alternate myxoid and edematous areas and occasional tubules

5
Figure 2 Ovary, spindle to small round-oval cells with occasional tubular and trabecular pattern

6
Figure 3 Ovary, round to oval cells in vague trabecular pattern with angular hyperchromatic nuclei and high mitotic activity. Note frequent atypical and abnormal mitotic figures

7
Figure 4 Immunoperoxidase stain
Figure 4 Immunoperoxidase stain. The neoplastic cells stain with Inhibin

8
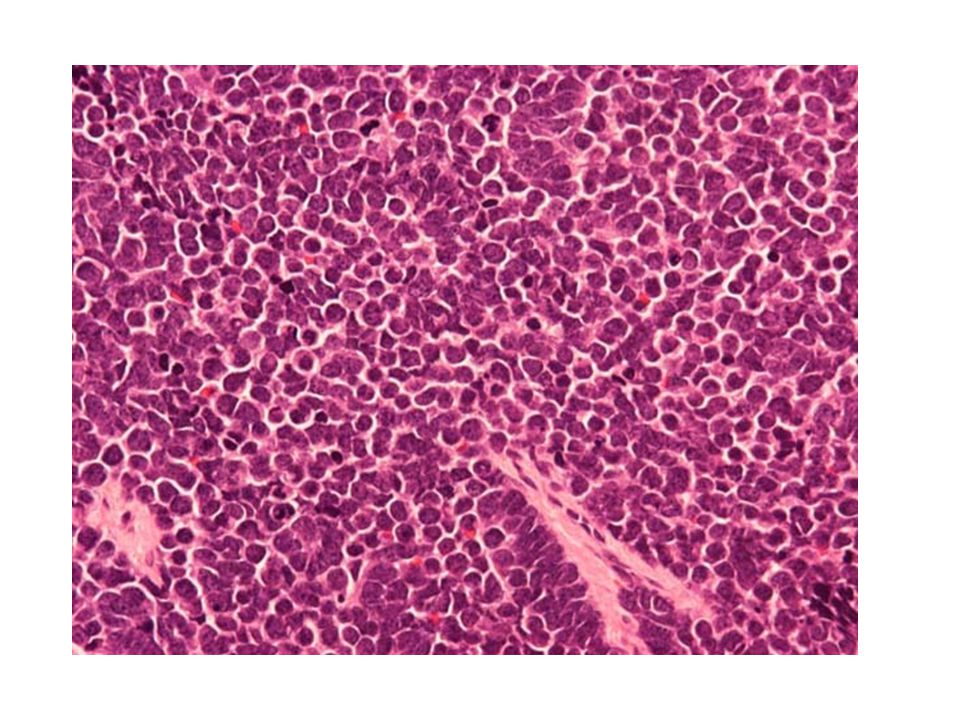
Figures 5 & 6 Recurrent omental lesion
Figures 5 & 6 Recurrent omental lesion. The cells in diffuse to vague storiform and fascicular pattern with alternate myxoid and edematous areas. Neoplastic cells are round or elongated with hyperchromatic nuclei. Significant mitotic activity (>10 / 10 HPF) is evident. Sertoli-like tubular structures or Leydig cell nests are not seen, as seen in original ovarian tumor.
 is evident. Sertoli-like tubular structures or Leydig cell nests are not seen, as seen in original ovarian tumor.")
10
Final Diagnosis?

11
Sex Cord Stromal Tumor

12
DISCUSSION: Sex cord stromal tumors represent approximately 8% of all ovarian tumors (1). They may be composed of cells of ovarian origin (e.g. granulosa - stromal cells) or testicular origin (Sertoli - stromal cells). At times the neoplastic cells are immature and show no further differentiation with morphology intermediate between testicular and ovarian cell types or architectural patterns non-specific to either the testis or the ovary (1). In such cases it may be impossible to determine the category of the tumor, whether it belongs to the Granulosa - stromal or Sertoli - stromal category. In such circumstances the term sex cord - stromal tumor, unclassified introduced by WHO can be used (1). This case is interesting because initial ovarian tumor had combined poorly differentiated juvenile granulosa cells and Sertoli Leydig cell differentiation. However when it recurred, the tumor was less differentiated and showed mostly monotonous arrangements of small cells without Sertoli like tubular structures or Leydig cell nests (Figures 5 &6). This can be a diagnostic dilemma, if the tumor presents as an undifferentiated sex cord stromal tumor, with no definitive features of granulosa stromal cells or Sertoli stromal cells. Most of the sex cord stromal tumor of the ovary can be easily classified. However about 10% of the sex cord stromal tumors are difficult to classify (2) especially when they have a low degree of differentiation with an overall feature that prevents their placement in either the Granulosa or Sertoli Leydig category (2).
. They may be composed of cells of ovarian origin (e.g. granulosa - stromal cells) or testicular origin (Sertoli - stromal cells). At times the neoplastic cells are immature and show no further differentiation with morphology intermediate between testicular and ovarian cell types or architectural patterns non-specific to either the testis or the ovary (1). In such cases it may be impossible to determine the category of the tumor, whether it belongs to the Granulosa - stromal or Sertoli - stromal category. In such circumstances the term sex cord - stromal tumor, unclassified introduced by WHO can be used (1). This case is interesting because initial ovarian tumor had combined poorly differentiated juvenile granulosa cells and Sertoli Leydig cell differentiation. However when it recurred, the tumor was less differentiated and showed mostly monotonous arrangements of small cells without Sertoli like tubular structures or Leydig cell nests (Figures 5 &6). This can be a diagnostic dilemma, if the tumor presents as an undifferentiated sex cord stromal tumor, with no definitive features of granulosa stromal cells or Sertoli stromal cells. Most of the sex cord stromal tumor of the ovary can be easily classified. However about 10% of the sex cord stromal tumors are difficult to classify (2) especially when they have a low degree of differentiation with an overall feature that prevents their placement in either the Granulosa or Sertoli Leydig category (2).")
14
A Female in Her 70s With Pelvic Masses http://path. upmc
CLINICAL HISTORY: The patient is a female in her 70s with pelvic masses and ascites. Her preoperative CA-125 increased to 130 units/ml, but CA19-9 and CEA were normal. She underwent total abdominal hysterectomy, bilateral salphingo-oophorectomy, omentectomy as well as cul-de-sac excisional biopsy. The left ovary and fallopian tube were distorted by multiple tan-white firm nodules with homogenous cut surface. The right adnexa were completely replaced by tumor masses which were fused with a tubular structure resembling vermiform appendix

15
The nodules were made up of trabeculae, ribbons and nests of medium to large size polygonal tumor cells, with organoid growth pattern in some areas and pallisading in other areas

16
The tumor cells had relatively uniform oval to round, finely granular nuclei, with eosinophilic and granular cytoplasm

18
In the part that was labeled "right adnexa", there was no recognizable ovarian tissue or fallopian tube. Instead, the vermiform appendix was embedded in the tumor masses. There was a luminal, mural and serosal involvement of the appendix by the tumor

20
Mesentery sigmoid colon involvement.

21
Pelvic sidewalls, cul-de-sac and omentum involvement.

22
Synaptophysin (+)
")
23
CK 7 (+)
")
24
CK 20 (-)
")
25
CDX2 (-)
")
26
TTF-1 (+)
")
27
IMMUNOHISTOCHEMICAL STAININGS:
Chromogranin + Calcitonin - Synaptophysin CD5 CK 7 HCG CK 20 ER CDX2 PR TTF-1 Her2/Neu Thyroglobulin GCDFP

28
Non-small Cell Neuroendocrine Carcinoma
Final Diagnosis : Non-small Cell Neuroendocrine Carcinoma

29
DISCUSSION: The microscopic features of this epithelial neoplasm are consistent with a non-small cell neuroendocrine carcinoma, which was supported by the positive chromogranin and synaptophysin stainings. This is a very challenging case with respect to determining the primary site of origin for this neoplasm. As revealed in the immunohistochemical panel, the carcinoma expresses TTF-1 and CK7; it fails to express all other markers specific to other potential primary sites of origin including CDX2 and CK20. TTF-1 is a nuclear homeodomain transcription factor that is thought to be expressed in pulmonary and thyroid neoplasms. Particularly, neuroendocrine tumors of the lung, including typical and atypical carcinoids and large cell neuroendocrine carcinomas, show > 90% positivity with TTF-1 (Folpe et al., 1999). TTF-1 is rarely expressed in extrapulmonary neuroendocrine tumors except for small cell carcinomas that can have as high as 44-80% positivity (Agoff, et al., 2000; Kaufmann and Dietel, 2000). For a non-small cell neuroendocrine carcinoma staining positive with TTF-1, the most likely site of origin is lung. Moreoever, a TTF-1+ / CK7+/CK20- immunopanel (as in this case) has been suggested to be moderately sensitive and highly specific for a diagnosis of pulmonary origin in carcinoid tumors (Cai, et al., 2001). However, no discrete pulmonary mass was present on CT scan in this case. Without a pulmonary lesion, one must strongly consider other potential sites of origin. In fact, Kaufmann and Dietel demonstrated positive TTF-1 expression in 1 of 4 extrapulmonary large cell neuroendocrine carcinomas, and concluded that TTF-1 should not be used as a marker for pulmonary carcinomas before excluding small cell carcinoma as well as large cell neuroendocrine carcinoma. They also demonstrated rare cases of positive TTF-1 staining in genitourinary and gastrointestinal neuroendocrine tumors. In the absence of a pulmonary mass, the most likely original site would be gastrointestinal tract, particularly in the clinical picture of this case. In the "right adnexa", there is a luminal, mural and serosal involvement of the appendix by the neuroendocrine tumor although the appendiceal mucosa itself appears to be largely intact. The most common appendiceal malignancy is carcinoid tumor and it is the most common neuroendocrine neoplasm in the abdomen outside of pancreas. Although the appendix as a primary site is relatively uncommon, primary malignant GI tract tumors metastasizing to ovaries is a well described clinicopathologic condition such that any time one has bilateral tumor involvements of the ovary it directs the clinician to exclude metastases (McBroom, et al., 2000). As for the immunohistochemical markers, carcinoids of GI tract unfortunately have low frequencies of positive CDX2 staining, unlike other GI neoplasms (We rling, et al., 2003). In addition, GI neuroendocrine tumors including carcinoids have low incidence of CK20 expression, despite the high frequency of CK20 positivity in colorectal carcinomas (Chu, et al., 2000).
. TTF-1 is rarely expressed in extrapulmonary neuroendocrine tumors except for small cell carcinomas that can have as high as 44-80% positivity (Agoff, et al., 2000; Kaufmann and Dietel, 2000). For a non-small cell neuroendocrine carcinoma staining positive with TTF-1, the most likely site of origin is lung. Moreoever, a TTF-1+ / CK7+/CK20- immunopanel (as in this case) has been suggested to be moderately sensitive and highly specific for a diagnosis of pulmonary origin in carcinoid tumors (Cai, et al., 2001). However, no discrete pulmonary mass was present on CT scan in this case. Without a pulmonary lesion, one must strongly consider other potential sites of origin. In fact, Kaufmann and Dietel demonstrated positive TTF-1 expression in 1 of 4 extrapulmonary large cell neuroendocrine carcinomas, and concluded that TTF-1 should not be used as a marker for pulmonary carcinomas before excluding small cell carcinoma as well as large cell neuroendocrine carcinoma. They also demonstrated rare cases of positive TTF-1 staining in genitourinary and gastrointestinal neuroendocrine tumors. In the absence of a pulmonary mass, the most likely original site would be gastrointestinal tract, particularly in the clinical picture of this case. In the right adnexa , there is a luminal, mural and serosal involvement of the appendix by the neuroendocrine tumor although the appendiceal mucosa itself appears to be largely intact. The most common appendiceal malignancy is carcinoid tumor and it is the most common neuroendocrine neoplasm in the abdomen outside of pancreas. Although the appendix as a primary site is relatively uncommon, primary malignant GI tract tumors metastasizing to ovaries is a well described clinicopathologic condition such that any time one has bilateral tumor involvements of the ovary it directs the clinician to exclude metastases (McBroom, et al., 2000). As for the immunohistochemical markers, carcinoids of GI tract unfortunately have low frequencies of positive CDX2 staining, unlike other GI neoplasms (We rling, et al., 2003). In addition, GI neuroendocrine tumors including carcinoids have low incidence of CK20 expression, despite the high frequency of CK20 positivity in colorectal carcinomas (Chu, et al., 2000).")
31
PATIENT HISTORY: A 36-year-old Gravida 3 Para 2 woman experienced intrauterine loss of twin B at 14 weeks gestational age. The twin B fetus was retained. At 39+ weeks twin A was delivered as a 3141 gram liveborn male infant with Apgar scores of 9 at one minute and 9 at 5 minutes. No abnormalities were noted.

32
GROSS DESCRIPTION B

33
B

34
B

35
RADIOLOGY DESCRIPTION

37
Fetus A: The villi are small and well developed and contain numerous syncytial knots with good vasculosyncytial membranes

38
There is reactive amnion with moderate meconium containing macrophages.

39
The umbilical cord is unremarkable.

40
Fetus B: There is complete hyalinization of the villi and extensive loss of fetal vessels.

41
Final Diagnosis PLACENTA "A", 420 GRAMS (51-75TH PERCENTILE):
VILLOUS MATURATION APPROPRIATE FOR GESTATIONAL AGE REACTIVE AMNION WITH MODERATE MECONIUM CONTAINING MACROPHAGES UMBILICAL CORD WITH THREE VESSELS, 37.0 CM PLACENTA "B", 50 GRAMS: FETUS PAPYRACEUS COMPLETE HYALINIZATION AND LOSS OF FETAL VESSELS

42
Contributor's Note: The term fetus papyraceus is used to describe a flattened, mummified fetus associated with a viable twin or multiple gestation. Intrauterine fetal demise of a twin after eight weeks gestational age with retention of the fetus for a minimum of 10 weeks results in mechanical compression of the small fetus such that it resembles parchment paper. Prior to eight weeks gestational age the only evidence of an intrauterine death of a twin may be a cyst on the fetal surface of the surviving twin placenta. The reported incidence is 1:12,000 live births and ranges between 1:184 and 1:200 twin pregnancies. In most cases death occurs in the second trimester between the third and fifth month. Virtually all occur before the seventh month allowing enough intrauterine retention time to elapse in order for mummification to occur. In our case the estimated gestational age at the time of fetal demise was 14 weeks. The appearance of a calcified fetus or lithopedion may be evident if maturation is advanced. This can occur if there is retention of the fetus for many months beyond the average gestation. It is important to remember that a lithopedion does not need to be a twin. In one reported case, a 94-year-old woman was found to have a lithopedion, probably present for approximately 61 years. Causative factors have been debated in the literature and in many cases remain unknown. The role of velamentous cord insertion has been postulated. A case of lethal nuchal cord was reported to result in fetus papyraceus. Others have seen this phenomenon occurring more often with monozygotic twin pregnancies versus dizygotic. No association with maternal age, parity nor gravidity has been noted. In our case, a cause was not identified. In many cases of fetus papyraceus there are no complications to the mother or to the surviving twin, as was the situation described in the case presented here. However, multiple reports have shown that complications can and do occur.

43
Another example for FETUS PAPYRACEUS

45
Female, 37 years old with uterine bleeding and no other symptoms of interest.
Sample: Endometrial aspirate. H-E stained.

50
Diagnosis? A total of 29 answers for this case were divided as follows: - 22: Atypical Hyperplasia. - 04: Probable Endometrial Carcinoma. - 02: Normal Secretory Endometrium. - 01: No Diagnostic Opinion because of "not enough clinical information".

51
“Atypical Endometrial Hyperplasia".
The final diagnosis: “Atypical Endometrial Hyperplasia". A curetting biopsy was suggested in order to rule out a posible adenocarcinoma (despite the age of the patient).
.")
53
بیست و یکمین کنفرانس وحدت کشورهای اسلامی

Similar presentations










>")




>")












 Chapter: Neoplasia Definitions Nomenclature Characteristics of benign and malignant neoplasms Epidemiology.>")
