Download presentation
Presentation is loading. Please wait.

1
Persistent Pulmonary Hypertension of the Newborn John Salyer RRT-NPS, MBA, FAARC Director Respiratory Therapy Seattle Children’s Hospital and Research Institute

2
Sense and Sensibility??!? Of the deaths in England in 1859, no less than 184,264 -- two in every five of the deaths of the year -- were of children under five years of age Above half of these -- 105,629 -- had scarcely seen the light, and never saw one return of their birthday.” 43 to 45 infant deaths take place in every 100 births -- 45 per cent! Almost half of the children who are born, die -- perish miserably! And this is far from representing the whole mass of pain and suffering, which it is the calamity of children to endure.” M.A. Barnes 1862: Excessive Infant Mortality: How Can It Be Stayed? British Social Science Association

3
Respiratory Care Service-CHRMC

5
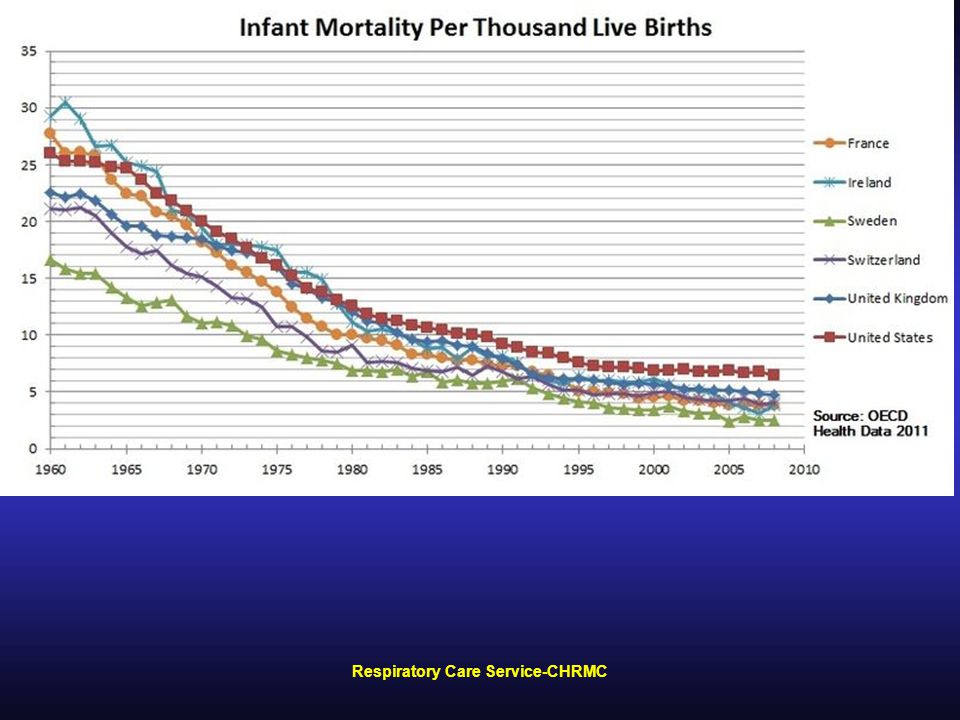
It’s the Best Time to Be Alive (So Far) Respiratory Care Service-CHRMC
 Respiratory Care Service-CHRMC")
6
Fetal Circulation

7
PPHN Pathophysiology Pulmonary hypertension is a normal and necessary state for the fetus In utero, only 5 -10% of the combined ventricular output is directed to the pulmonary vascular bed. 80% of drop in pulmonary artery pressure occurs in 1st 24 h, by local vasodilatation Neonatal vessels greater vasoconstrictive response Oxygen vasodilates vessels Hypoxemia may release vasoconstrictive mediators, perpetuating vasospasm

8
PPHN Pathophysiology At Birth –Rapid PVR and in pulmonary artery pressure –10-fold rise in pulmonary blood flow. –Signals for these transitional changes mechanical distension of the lung, PaCO 2, PaO 2

9
Respiratory Care Service-CHRMC

10
Epidemiology Severe PPHN has been estimated to occur in 2 out of 1000 live-born term infants, and Some degree of pulmonary hypertension complicates the course of more than 10% of all neonates with respiratory failure.respiratory failure Respiratory failure and hypoxemia in the term newborn results from a heterogeneous group of disorders, and the therapeutic approach and response often depend on the underlying disease. Idiopathic pulmonary hypertension is responsible for 10-20% of all infants with PPHN.

11
Clin Perinatol 11: 525, 1984. PPHN: Pathophysiology

12
Respiratory Care Service-CHRMC

14
PO 2 L -> R ductus arteriosus shunt Ventilation Remove Placenta Ductus Venosus Closes Systemic Vascular Resistance Umbilical venous return IVC Return RA pressure Pulmonary venous return LA pressure Foramen Ovale closes Pulmonary Vascular Resistance

15
Effects of lung volume on PVR B Alveolar vessels compress with lung inflation A Extra alveolar vessels have high resistance at low and high lung volumes

16
Hypoxia/low pH Pulmonary problems Endothelin-1 (hypoxia induced) Thromboxane A 2 (hypoxia induced) Leukotrienes C 4 and D 4 Platelet-activating factor Low production of vasodilators (PGI 2 and NO) Overinflation/Underinflation Excessive muscularization Altered mechanical properties of smooth muscle Fetal vasculature opposing vasodilation Hypothermia (pulmonary venous constriction) Polycythemia NO PgI 2 PDE 5 Adenosine ATP Magnesium Bradykinin Atrial natriuretic factor Decreased PVR Vasodilation Oxygen Lung inflation Structural changes in endothelial cells Changes in interstitial fluid and pressure Shear stress Increased PVR Vasoconstriction Transition
 Thromboxane A 2 (hypoxia induced) Leukotrienes C 4 and D 4 Platelet-activating factor Low production of vasodilators (PGI 2 and NO) Overinflation/Underinflation Excessive muscularization Altered mechanical properties of smooth muscle Fetal vasculature opposing vasodilation Hypothermia (pulmonary venous constriction) Polycythemia NO PgI 2 PDE 5 Adenosine ATP Magnesium Bradykinin Atrial natriuretic factor Decreased PVR Vasodilation Oxygen Lung inflation Structural changes in endothelial cells Changes in interstitial fluid and pressure Shear stress Increased PVR Vasoconstriction Transition")
17
1) PPHN mechanisms: Lung disease Abnormally constricted pulmonary vasculature – MAS – Pneumonia – RDS MA S RDSGBS pneumonia
 PPHN mechanisms: Lung disease Abnormally constricted pulmonary vasculature – MAS – Pneumonia – RDS MA S RDSGBS pneumonia")
18
Respiratory Care Service-CHRMC Postulated Pathogenic Mechanisms Repeated intrauterine closure of ductus May occur in Mothers taking high dose Aspirin near term Abnormal responsiveness of pulmonary vasculature to hypoxia with inability to relax after stimulus is removed – birth asphyxia Repeat intrauterine hypoxia = hypertrophy of medial muscles surrounding pulmonary arterioles Pulmonary hypoplasia Alterations in vasoactive mediator levels Mediators participate in transition from fetal to neonatal circulation Nitric Oxide is one mediator Microthrombus formation in pulmonary vascular bed Most often associated with perinatal asphyxia, hypoglycemia, hypocalemia and sepsis

19
PPHN: Diagnosis Suggested by hypoxemia out of proportion to severity of lung disease Swings of oxygenation without ventilator change Inability to maintain PaO 2 > 60 in 100% O 2 Gradient in preductal (right radial) and postductal PaO 2 (>20 mm Hg) or O 2 saturations (> 6%) Oxygenation Index (OI) > 15-20 Echocardiogram: document shunting, PA pressure
 and postductal PaO 2 (>20 mm Hg) or O 2 saturations (> 6%) Oxygenation Index (OI) > Echocardiogram: document shunting, PA pressure")
20
Respiratory Care Service-CHRMC Diagnosis of PPHN Term or near term Cyanosis Respiratory distress Normal X-ray Unless aspiration, Hyaline membrane disease, CDH

21
Respiratory Care Service-CHRMC Three Classifications of PPHN 1.Primary PPHN Radiographically normal lungs, no evidence of parenchymal disease 2.Secondary PPHN Hyaline Membrane Disease Meconium Aspiration Aspiration Pneumonia Transient Tachypnea of the Newborn Sepsis-Group B Strep 3.Associated with Hypoplasia of the Lungs Most often Congenital Diaphragmatic Hernia

22
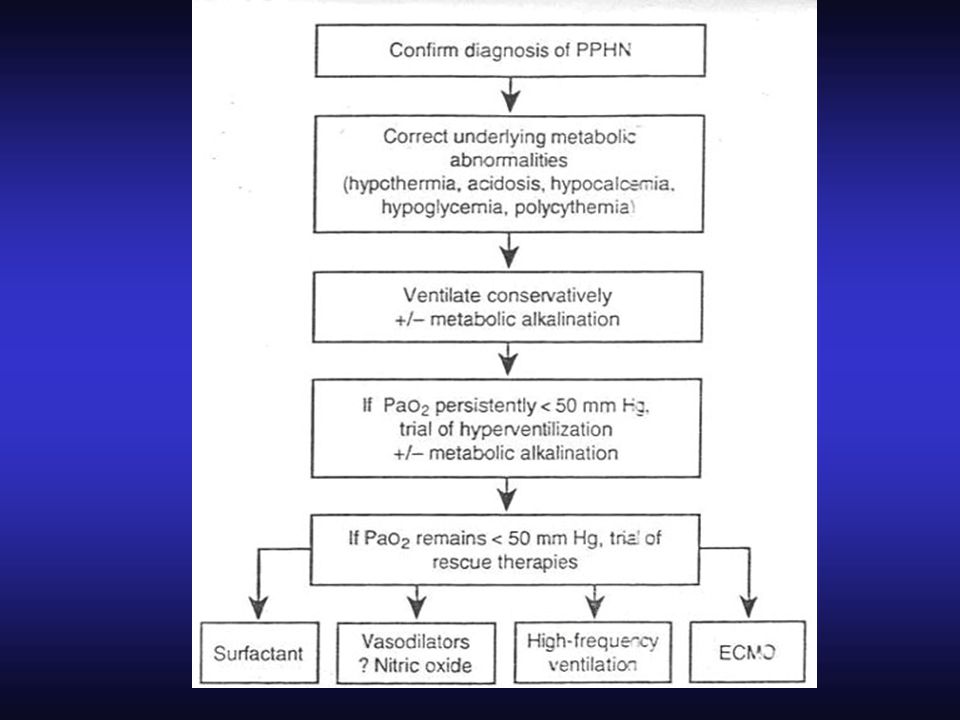
Confirm diagnosis of PPHN (R/O Heart Disease Correct underlying abnormalities: –metabolic (hypocalcemia, hypoglycemia) –acidosis –hypothermia –polycythemia, –sepsis –surfactant Tx for IRDS –evacuate pneumothoraces PPHN: Treatment #1
 –acidosis –hypothermia –polycythemia, –sepsis –surfactant Tx for IRDS –evacuate pneumothoraces PPHN: Treatment #1")
23
Maintain pH 7.35-7.50 Try high frequency ventilation Consider sedation, paralysis Induce metabolic alkalosis Elevate systemic pressure Maximize cardiac output (preload, and Dobutamine) PPHN: Treatment #2 Other StrategiesVentilation strategies Consider NO if OI > 20 Consider ECMO if OI >40
 PPHN: Treatment #2 Other StrategiesVentilation strategies Consider NO if OI > 20 Consider ECMO if OI >40")
24
Respiratory Care Service-CHRMC Treatment of PPHN Early diagnosis Improve alveolar oxygenation Minimize pulmonary vasoconstriction Hyperventilation – CO2 above 25 mmHG Work to reduce pulmonary trauma Consider different forms of ventilation Sedation and paralytics Consider induction of alkalotic state – sodium Bicarbonate Vasoconstriction appears related to intracellular pH rather than CO2 levels End product of sodium bicarbonate is increased CO2

25
Respiratory Care Service-CHRMC Treatment of PPHN Continued Maintain systemic blood pressure and perfusion In theory increasing systemic arterial pressure may result in decreased right to left shunt – improving oxygenation Dopamine and Dobutamine are frequently used Nitric Oxide Free radical gas Increases cyclic GMP in smooth muscles = vascular relaxation Must get to pulmonary capillary bed

26
Respiratory Care Service-CHRMC Treatment of PPHN Continued Vasodialators Tolazoline (Priscoline) Appears to be a alpha-sympathetic blocker = vasodialator Can cause large drops in systemic vascular blood pressure Can be administered through endotracheal tube Prostaglandin 12 Major endogenous vasodialator in lung Normally produced when pulmonary vessels are constriced May be helped if Tolazoline has failed ECMO
 Appears to be a alpha-sympathetic blocker = vasodialator Can cause large drops in systemic vascular blood pressure Can be administered through endotracheal tube Prostaglandin 12 Major endogenous vasodialator in lung Normally produced when pulmonary vessels are constriced May be helped if Tolazoline has failed ECMO")
27
Contraindications for iNO use Congenital heart disease that is dependent on right-to-left shunting across ductus arteriosus Critical Aortic Stenosis Interrupted Aortic Arch Hypoplastic Left Heart Syndrome May worsen pulmonary edema in patients with TAPVR due to the fixed venous obstruction

28
Prostacyclin (PGI 2 ) Analogues Stimulates membrane bound adenylate cyclase, increases cAMP Acutely relaxes vascular smooth muscle Inhibits pulmonary artery smooth muscle cell proliferation in vitro; inhibits platelet aggregation; ameliorates endothelial injury Reverses vascular remodeling Reduces synthesis and clears ET-1 Exerts positive inotropic effects
 Analogues Stimulates membrane bound adenylate cyclase, increases cAMP Acutely relaxes vascular smooth muscle Inhibits pulmonary artery smooth muscle cell proliferation in vitro; inhibits platelet aggregation; ameliorates endothelial injury Reverses vascular remodeling Reduces synthesis and clears ET-1 Exerts positive inotropic effects")
29
Prostacyclin (PGI 2 ) Analogues Continuous i.v. infusion of epoprostenol (Flolan™) Costly, ½ life 3-5 minutes Escalation of dosing is frequently required Acute withdrawal can lead to fatal PH May lower systemic vascular resistance, worsening ductal or atrial level R -> L shunt May worsen intrapulmonary shunts by vasodilating non-ventilated areas of the lung
 Costly, ½ life 3-5 minutes Escalation of dosing is frequently required Acute withdrawal can lead to fatal PH May lower systemic vascular resistance, worsening ductal or atrial level R -> L shunt May worsen intrapulmonary shunts by vasodilating non-ventilated areas of the lung.")
30
Respiratory Care Service-CHRMC Outcomes Before ECMO death rates were above 50%, with ECMO death rates are about 15% Status post ECMO neonates have reported 45% morbidity rates Moderate to severe lung disease With high alkaline states, can have some degree of deafness Right ventricular hypertrophy With CDH, can have many residual complications

Similar presentations