Download presentation
Presentation is loading. Please wait.

2
2 Ataei.B, MD. MPH. Associate professor of Infectious Diseases Isfahan University of Medical Sciences ( IUMS) ( IUMS)
 ( IUMS).")
3
Acute viral hepatitis is a systemic infection affecting the liver predominantly. Almost all cases of acute viral hepatitis are caused by one of five viral agents: Hepatitis A virus (HAV) Hepatitis B virus (HBV) Hepatitis C virus (HCV) HBV-associated delta agent or hepatitis D virus (HDV) Hepatitis E virus (HEV). Transfusion-transmitted agents, e.g., "hepatitis G" virus and "TT" virus, have been identified but do not cause hepatitis. 3
 Hepatitis B virus (HBV) Hepatitis C virus (HCV) HBV-associated delta agent or hepatitis D virus (HDV) Hepatitis E virus (HEV). Transfusion-transmitted agents, e.g., hepatitis G virus and TT virus, have been identified but do not cause hepatitis. 3.")
4
Minor agents: EBV,CMV HSV,VZV Rubella,Measles Coxsackie B Adenovirus 4

5
All these human hepatitis viruses are RNA viruses, except for hepatitis B, which is a DNA virus. all types of viral hepatitis produce clinically similar illnesses. These range from asymptomatic and inapparent to fulminant and fatal acute infections common to all types 5

6
from subclinical persistent infections to rapidly progressive chronic liver disease with cirrhosis and even hepatocellular carcinoma, common to the bloodborne types (HBV, HCV, and HDV). 6

7
7

8
Hepatitis A Hepatitis A virus is a non enveloped 27-nm, heat-, acid-, and ether-resistant RNA virus in the hepatovirus genus of the picornavirus family. Inactivation of viral activity can be achieved by boiling for 1 min, by contact with formaldehyde and chlorine, or by ultraviolet irradiation. 8

9
Its replication is limited to the liver, but the virus is present in the liver, bile, stools, and blood during the late incubation period and acute preicteric phase of illness 9

10
Hepatitis A: transmitted almost exclusively by the fecal-oral route. Person-to-person spread of HAV is enhanced by poor personal hygiene and overcrowding; 10

11
large outbreaks as well as sporadic cases have been traced to contaminated food, water, milk, frozen raspberries and strawberries, green onions and shellfish. Intrafamily and intrainstitutional spread are also common. 11

12
Early epidemiologic observations supported a predilection for hepatitis A to occur in late fall and early winter. Although hepatitis A is rarely bloodborne, several outbreaks have been recognized in recipients of clotting factor concentrates. Age preference Children, young adults 12

14
Hepatitis B: Hepatitis B virus is a DNA virus with a remarkably compact genomic structure; hepadnaviruses (hepatotropic DNA viruses), Hepatitis B isolates fall into one of at least eight subtypes and eight genotypes (A–H). 14

16
Hepatitis B virus (HBV) Four open reading frames (ORF) : S region: encode HBsAg—major protein C region included pre-c and C gene:encode HBeAg and HBcAg X region :encoded HBxAg P region: encoded DNA polymerase 16
 Four open reading frames (ORF) : S region: encode HBsAg—major protein C region included pre-c and C gene:encode HBeAg and HBcAg X region :encoded HBxAg P region: encoded DNA polymerase 16")
17
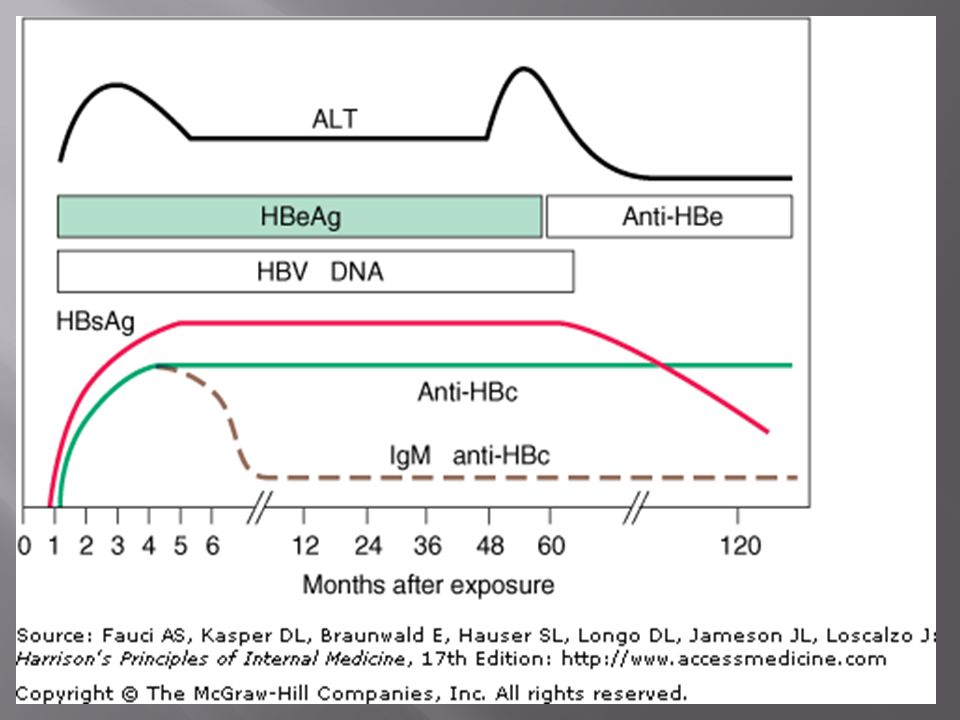
After a person is infected with HBV, the first virologic marker detectable in serum within 1–12 weeks, usually between 8–12 weeks, is HBsAg. In typical cases, HBsAg becomes undetectable 1–2 months after the onset of jaundice and rarely persists beyond 6 months. 17

18
Because HBcAg is intracellular. Therefore, HBcAg is not detectable routinely in the serum of patients with HBV infection 18

19
Occasionally, in 10–20% of patients with chronic hepatitis B, low-level, low-affinity anti-HBs can be detected. This antibody is directed against a subtype determinant different from that represented by the patient's HBsAg; These patients with HBsAg and such non neutralizing anti-HBs should be categorized as having chronic HBV infection. 19

20
Hepatitis B antigens and HBV DNA have been identified in extrahepatic sites, including: Lymph nodes, Bone marrow, Circulating lymphocytes Spleen, Pancreas 20

21
Although the virus does not appear to be associated with tissue injury in any of these extrahepatic sites, its presence in these "remote" reservoirs has been invoked to explain the recurrence of HBV infection after orthotopic liver transplantation. 21

22
Hepatitis B: Transmission 1. Percutaneous contact 2. Mucous membrane contact 3. Sexual contact 4. Perinatal contact :third trimester and early postpartum 22

23
although ~10% of infections may be acquired in utero. likelihood of perinatal transmission of HBV correlates with the presence of HBeAg; 90% of HBeAg-positive mothers but only 10–15% of anti- HBe-positive mothers transmit HBV infection to their offspring. In most cases, acute infection in the neonate is clinically asymptomatic, but the child is very likely to become an HBsAg carrier. 23

24
Fulminant : 0.1–1% Progression to chronicity : Occasional (1–10%) (90% of neonates) Carrier : 0.1–30% The >350 million HBsAg carriers in the world constitute the main reservoir of hepatitis B in human beings 24
 (90% of neonates) Carrier : 0.1–30% The >350 million HBsAg carriers in the world constitute the main reservoir of hepatitis B in human beings 24")
26
Hepatitis D The delta hepatitis agent, or HDV, is a defective RNA virus that coinfects with and requires the helper function of HBV (or other hepadnaviruses) for its replication and expression. HDV can either infect a person simultaneously with HBV (co-infection) Superinfect a person already infected with HBV (superinfection); 26
 Superinfect a person already infected with HBV (superinfection); 26.")
27
In chronic HDV infection, anti-HDV circulates in high titer, and both IgM and IgG anti-HDV can be detected. HDV antigen in the liver and HDV RNA in serum and liver can be detected during HDV replication. 27

28
Hepatitis D Infection with HDV has a worldwide distribution. Two epidemiologic patterns exist. 1) In Mediterranean countries (northern Africa, southern Europe, the Middle East), HDV infection is endemic among those with hepatitis B, and the disease is transmitted predominantly by non percutaneous means, especially close personal contact 28
 In Mediterranean countries (northern Africa, southern Europe, the Middle East), HDV infection is endemic among those with hepatitis B, and the disease is transmitted predominantly by non percutaneous means, especially close personal contact 28.")
29
1) In non endemic areas, such as the United States and northern Europe, HDV infection is confined to persons exposed frequently to blood and blood products, primarily injection drug users and hemophiliacs. 2) HDV infection can be introduced into a population through drug users or by migration of persons from endemic to non endemic areas. 29
 HDV infection can be introduced into a population through drug users or by migration of persons from endemic to non endemic areas. 29.")
31
Hepatitis C Hepatitis C virus, which, before its identification was labeled "non-A, non-B hepatitis, Linear, single-strand, positive-sense, 9600-nucleotide RNA virus, 31

32
HCV is the only member of the genus Hepacivirus in the family Flaviviridae. At least six distinct genotypes, as well as >50 subtypes within genotypes 32

33
Hepatitis C Transmitted by transfusion. Injection drug use. Occupational exposure to blood, and the likelihood of infection is increased in hemodialysis units HCV transmitted sexually and perinatally; however, both of these modes of transmission are inefficient for hepatitis C. 33

34
chances of sexual and perinatal transmission have been estimated to be ~5%, Breast feeding does not increase the risk of HCV infection between an infected mother and her infant 34

35
extraordinarily high prevalences of HCV infection occur in certain countries, such as Egypt, where >20% of the population in some cities is infected. High frequency in Egypt is attributable to contaminated equipment used for medical procedures and unsafe injection practices 35

37
Hepatitis E: Previously labeled epidemic or enterically transmitted non-A, non-B hepatitis, HEV is an enterically transmitted virus Resembling caliciviruses 37

38
Hepatitis E This type of hepatitis, identified in India, Asia, Africa, the Middle East, and Central America, resembles hepatitis A in its primarily enteric mode of spread An epidemiologic feature that distinguishes HEV from other enteric agents is the rarity of secondary person-to-person spread from infected persons to their close contacts. 38

40
Immune complex–mediated tissue damage appears to play a pathogenetic role in the extrahepatic manifestations of acute hepatitis B. The occasional prodromal serum sickness–like syndrome observed in acute hepatitis B appears to be related to the deposition in tissue blood vessel walls of HBsAg-anti-HBs circulating immune complexes, leading to activation of the complement system and depressed serum complement levels. 40

41
In patients with chronic hepatitis B, other types of immune-complex disease may be seen. Glomerulonephritis with the nephritic syndrome is occasionally observed; HBsAg, immunoglobulin, and C3 deposition has been found in the glomerular basement membrane. 41

42
Polyarteritis nodosa develops in considerably fewer than 1% of patients with chronic HBV infection, 20–30% of patients with polyarteritis nodosa have HBsAg in serum. Immune-complex glomerulonephritis is another recognized extrahepatic manifestation of chronic hepatitis C. 42

43
essential mixed cryoglobulinemia (EMC), was reported initially to be associated with hepatitis B & C o The disorder is characterized clinically by arthritis, cutaneous vasculitis (palpable purpura), and occasionally with glomerulonephritis and serologically by the presence of circulating cryoprecipitable immune complexes of more than one immunoglobulin class 43
, was reported initially to be associated with hepatitis B & C o The disorder is characterized clinically by arthritis, cutaneous vasculitis (palpable purpura), and occasionally with glomerulonephritis and serologically by the presence of circulating cryoprecipitable immune complexes of more than one immunoglobulin class 43")
44
Infiltration of mononuclear cells Hepatic cells necrosis Kupfer cells hyperplasia Variable degrees of cholestasis In more severe cases; Bridging necrosis 44

45
45

47
Clinical Stages Incubation period Prodromal (preicteric) phase Icteric phase convalescence 47
 phase Icteric phase convalescence 47")
48
Asymptomatic Anicteric Fulminant Chronic 48

49
HAV:15-45 days(30) HBV: 30-180 days(60-90) HCV: 15-160 days(50) HDV: 30-180 days(60-90) HEV: 14-60 days(40) 49
 HBV: days(60-90) HCV: days(50) HDV: days(60-90) HEV: days(40) 49")
50
prodromal symptoms of acute viral hepatitis are systemic and quite variable. Constitutional symptoms of anorexia, nausea and vomiting, fatigue, malaise, arthralgias, myalgias, headache, photophobia, pharyngitis, cough, and coryza may precede the onset of jaundice by 1–2 weeks. 50

51
The nausea, vomiting, and anorexia are frequently associated with alterations in olfaction and taste. A low-grade fever between 38° and 39°C (100°–102°F) is more often present in hepatitis A and E than in hepatitis B or C, 51
 is more often present in hepatitis A and E than in hepatitis B or C, 51.")
52
except when hepatitis B is heralded by a serum sickness–like syndrome; rarely, a fever of 39.5°–40°C (103°–104°F) may accompany the constitutional symptoms. Dark urine and clay-colored stools may be from 1–5 days before the onset of clinical jaundice. 52

53
With the onset of clinical jaundice, the constitutional prodromal symptoms usually diminish, Some patients mild weight loss (2.5–5 kg) is common and may continue during the entire icteric phase 53
 is common and may continue during the entire icteric phase 53")
54
Liver becomes enlarged and tender Right upper quadrant pain and discomfort 54

55
55

56
56

57
57

58
Splenomegaly and cervical adenopathy are present in 10–20%. Rarely, a few spider angiomas appear during the icteric phase and disappear during convalescence. 58

59
constitutional symptoms disappear but usually some liver enlargement and abnormalities in liver biochemical tests are still evident. Duration of the post icteric phase is variable, ranging 2–12 weeks, Usually more prolonged in acute hepatitis B and C. 59

60
Complete clinical and biochemical recovery is: 1–2 months after all cases of hepatitis A and E 3–4 months after the onset of jaundice in three- quarters of uncomplicated, self-limited cases of hepatitis B and C Healthy adults, acute hepatitis B is self-limited in 95–99% while hepatitis C is self-limited in only ~15% 60

61
AST and ALT (SGOT and SGPT)=400– 4000 IU. Serum bilirubin =85–340 mol/L (5–20 mg/dL). Total bilirubin is equally divided between the conjugated and unconjugated fractions. 61

62
G6PD deficiency and sickle cell anemia, a high serum bilirubin level is common, resulting from superimposed hemolysis. Bilirubin levels >30 mg/dL have been observed and are not necessarily associated with a poor prognosis. 62

63
Neutropenia and lymphopenia are transient and are followed by a relative lymphocytosis. Atypical lymphocytes (varying between 2 and 20%) are common during the acute phase. 63
 are common during the acute phase. 63.")
64
Prothrombin time (PT) is important in patients with acute viral hepatitis. prolonged PT reflect a severe hepatic synthetic defect, extensive hepatocellular necrosis, and indicate a worse prognosis 64

65
hypoglycemia (Prolonged nausea and vomiting, inadequate carbohydrate intake, and poor hepatic glycogen ). Serum alkaline phosphatase may be normal or only mildly elevated. 65

66
IgM anti-HAV HBs Ag and IgM anti-HBc HCV Ab, HCV RNA PCR (gold standard) anti-HDV anti-HEV 66
 anti-HDV anti-HEV 66")
68
Symptoms HBeAg anti-HBe Total anti-HBc IgM anti-HBc anti-HBs HBsAg 0481216 20 242832 36 52100 Acute Hepatitis B Virus Infection with Recovery Typical Serologic Course Weeks after Exposure Titre

69
IgM anti-HBc Total anti-HBc HBsAg Acute (6 months) HBeAg Chronic (Years) anti-HBe 048 12 16202428 32 36 52 Years Weeks after Exposure Titre Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course
 HBeAg Chronic (Years) anti-HBe Years Weeks after Exposure Titre Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course")
70
Symptomatic Infection Chronic Infection Age at Infection Chronic Infection (%) Symptomatic Infection (%) Birth 1-6 months7-12 months 1-4 years Older Children and Adults 0 20 40 60 80 100 80 60 40 20 0 Outcome of Hepatitis B Virus Infection by Age at Infection Chronic Infection (%)
 Symptomatic Infection (%) Birth 1-6 months7-12 months 1-4 years Older Children and Adults Outcome of Hepatitis B Virus Infection by Age at Infection Chronic Infection (%)")
71
Symptoms anti-HCV ALT Normal 012345 61234 Hepatitis C Virus Infection Typical Serologic Course Titre Months Years Time after Exposure

72
anti-HBs Symptoms ALT Elevated Total anti-HDV IgM anti-HDV HDV RNA HBsAg HBV - HDV Co-infection Typical Serologic Course Time after Exposure Titre

73
Jaundice Symptoms ALT Total anti-HDV IgM anti-HDV HDV RNA HBsAg HBV - HDV Superinfection Typical Serologic Course Time after Exposure Titre

74
Symptoms ALT IgG anti-HEV IgM anti-HEV Virus in stool 012345678910101 1212 1313 Hepatitis E Virus Infection Typical Serologic Course Titer Weeks after Exposure

75
Liver biopsy is rarely necessary or indicated in acute viral hepatitis. Except when the diagnosis is questionable or when clinical evidence suggests a diagnosis of chronic hepatitis. 75

76
Hepatitis A: Relapsing hepatitis Cholestatic hepatitis Hepatitis B:serum sickness–like syndrome Arthralgia or arthritis, rash, angioedema, and rarely hematuria and proteinuria may develop in 5–10% of patients. Chronicity:HBV,HCV,HDV fulminancy:HAV,HBV,HDV,HEV 76

77
Viral hepatitis by minor agent Gram negative Sepsis Cholangitis,cholecystitis Flare up chronic hepatitis Drug-related hepatitis Ischemic hepatitis 77

78
Acute fatty liver of pregnancy, Cholestasis of pregnancy, Eclampsia, HELLP syndrome (hemolysis, elevated liver tests, and low platelets) 78
 78")
79
Indication of admission: Bilirubin>20 mg/dl Hypoglycemia Abnormal PT Hypoalbuminemia 79

80
Indication of admission : Poor oral intake Mental change,letargy Low compliance Other chronic disease 80

81
CBR is not mandatory Restriction activity No special diet &Therapy(HCV ? ) Drug &Alcohol avoidance Isolation is not necessary except special cases 81
 Drug &Alcohol avoidance Isolation is not necessary except special cases 81.")
82
Regular physical exam Liver size,mental state,icter Check of LFT,BS,PT,BIL Serial check of HBs Ag and HCV Ab 82

83
Hand washing,hygiene Universal percaution No sharing of personal items (razor,toothbrush,nail clipper) Sexual barrier 83
 Sexual barrier 83")
84
HAV: Pre-exposure prophylaxis: Vaccine,SIG:0.02 cc/kg Post-exposure prophylaxis: SIG:0.02 cc/kg ;For day care centers,family members Vaccine ? 84

85
85 Age, yearsNo. of DosesDoseSchedule, months HAVRIX (GlaxoSmithKline) 1–182720 ELU (0.5 mL)0, 6–12 ≥1921440 ELU (1.0 mL)0, 6–12 VAQTA (Merck) 1–18225 units (0.5 mL)0, 6–18 ≥19250 units (1.0 mL)0, 6–18
 1– ELU (0.5 mL)0, 6–12 ≥ ELU (1.0 mL)0, 6–12 VAQTA (Merck) 1–18225 units (0.5 mL)0, 6–18 ≥19250 units (1.0 mL)0, 6–18.")
86
A combination of this hepatitis A vaccine and hepatitis B vaccine, TWINRIX, is licensed for simultaneous protection against both of these viruses among adults (age 18 years). Each 1.0-mL dose contains 720 ELU of hepatitis A vaccine and 20 g of hepatitis B vaccine. These doses are recommended at months 0, 1, and 6. 86

87
HBV: Pre-exposure prophylaxis: Vaccine :months 0,1,6 Booster is not recommended Post-exposure prophylaxis: HBIG:0.06 cc/kg and complete course of vaccine 87

88
Post-exposure prophylaxis in vaccinated person : Responder:No treatment Nonresponder:HBIG+Vaccine(3) OR HBIG (2) in one month Response:anti-HBs>10miu/ml 88
 OR HBIG (2) in one month Response:anti-HBs>10miu/ml 88")
89
Ab response unknown: Check anti-HBs; If adequate:no treatment If inadequate:HBIG(1) +vaccine(1) 89
 +vaccine(1) 89")
90
Target GroupNo. of DosesDoseSchedule, months ENGERIX-B (GlaxoSmithKline) Infants, children (<1–10 years) 3or410µ g (0.5 mL)0, 1–2, 4–6 or 0, 1, 2,12 Adolescents (10–19 years) 3 or 410µ g (0.5 mL)0, 1–2, 4–6 or 0, 12, 24 or 0, 1, 2, 12 Adults (≥20 years)3or420 g (1.0 mL)0, 1, 2, 12 Hemodialysis patients <20 years410 µg (0.5 mL)0, 1, 2, 6 ≥20 years440 µg (2.0mL)0, 1, 2, 6 90
 Infants, children (<1–10 years) 3or410µ g (0.5 mL)0, 1–2, 4–6 or 0, 1, 2,12 Adolescents (10–19 years) 3 or 410µ g (0.5 mL)0, 1–2, 4–6 or 0, 12, 24 or 0, 1, 2, 12 Adults (≥20 years)3or420 g (1.0 mL)0, 1, 2, 12 Hemodialysis patients <20 years410 µg (0.5 mL)0, 1, 2, 6 ≥20 years440 µg (2.0mL)0, 1, 2,")
91
HCV :no treatment HEV: no treatment 91

92
HAV and HEV- ACUTE: SYMPTOMATIC HBV - ACUTE: SYMPTOMATIC severe acute hepatitis B: Nucleoside analogue, such as lamivudine, at the 100-mg/d oral HCV - ACUTE: SYMPTOMATIC interferon monotherapy (3 million units SC three times a week) is beneficial, reducing the rate of chronicity considerably by inducing sustained responses in 30–70% of patients 92
 is beneficial, reducing the rate of chronicity considerably by inducing sustained responses in 30–70% of patients 92")
93
THANK YOU

96
Fecal HAV Symptoms 0123 4561224 Hepatitis A Infection Total anti-HAV TitreALT IgM anti-HAV Months after exposure Typical Serological Course

Similar presentations
















>")

, Hepatovirus Picornavirus, enterovirus 72 27 nm 1 serotype only, although there are 4 genotypes.>")






BB Unit 4 Part 4 Hepatitis A-E Viruses.>")



