Download presentation
Presentation is loading. Please wait.

1
Pregnancy & Cardiovascular diseases
By Mohammad H. soliman (MSc. Cardiology)
")
2
Expected cardiovascular changes in pregnancy
Measurement Normal value Change in pregnancy (%) Heart rate bpm + 10%–20% Stroke volume mL + 30% Cardiac output L/min + 30%–50% Blood volume 5 L + 20%–50% Systemic vascular resistance 1, dyne/cm/sec - 20% Mean arterial pressure mm Hg Not significant Oxygen consumption 250 mL/min + 20%–30% Source: Clark SL, et al.1 and Elkayam U, Gleicher N. Hemodynamics and cardiac function during normal pregnancy and the puerperium. In: Elkayam U, Gleicher N, eds. Cardiac Problems in Pregnancy. 3rd ed. New York, NY: Wiley-Liss, Inc; 1998:3-19.
 Heart rate bpm. + 10%–20% Stroke volume mL. + 30% Cardiac output L/min. + 30%–50% Blood volume. 5 L. + 20%–50% Systemic vascular resistance. 1, dyne/cm/sec. - 20% Mean arterial pressure mm Hg. Not significant. Oxygen consumption. 250 mL/min. + 20%–30% Source: Clark SL, et al.1 and Elkayam U, Gleicher N. Hemodynamics and cardiac function during normal pregnancy and the puerperium. In: Elkayam U, Gleicher N, eds. Cardiac Problems in Pregnancy. 3rd ed. New York, NY: Wiley-Liss, Inc; 1998:3-19.")
3
Figure 1 Physiological changes in pregnancy.8 Systemic and
pulmonary vascular resistance fall during pregnancy. Blood pressure may fall in the second trimester, rising slightly in late pregnancy. Note that cardiac output and stroke volume peak by 16 weeks gestation.

4
PRE-PREGNANCY COUNSELLING
To estimate maternal mortality as well as morbidity Join antenatal care with a high risk pregnancy obstetric team. Minimising maternal risk: e,g if necessary by catheter or surgical intervention before conception Estimation and minimising fetal risk e,g maternal drug treatment may need changing before conception or once pregnant

5
Signs and symptoms of normal pregnancy versus heart failure

6
A risk index to predict complications
1. A prior cardiac event (including stroke, transient ischemic attack, or arrhythmia). 2. Cyanosis or poor functional class. 3. Left heart obstruction. 4. Systemic ventricular dysfunction. One point was assigned for each risk factor present. No pregnancy received more than 3 points. Women with 0 points had an estimated risk of a cardiac event of 5% (low risk), those with 1 point had a risk of 27% (intermediate risk), and those with more than 1 point had a 75% risk of having a cardiac event (high risk). All three deaths in the study of 562 women occurred in pregnancies with more than one point.
. 2. Cyanosis or poor functional class. 3. Left heart obstruction. 4. Systemic ventricular dysfunction. One point was assigned for each risk factor present. No pregnancy received more than 3 points. Women with 0 points had an estimated risk of a cardiac event of 5% (low risk), those with 1 point had a risk of 27% (intermediate risk), and those with more than 1 point had a 75% risk of having a cardiac event (high risk). All three deaths in the study of 562 women occurred in pregnancies with more than one point.")
7
Maternal mortality risk associated with pregnancy
Group I: Minimal risk of complications (mortality <1%) -Pulmonic/tricuspid disease, ASD ,VSD ,PDA -Bioprosthetic valve ,mild AR, mild PS -Mitral stenosis, NYHA Class I or II Group II: Moderate risk of complications (mortality 5% to 15%) - Mitral stenosis with AF -Artificial valve -Mitral stenosis, NYHA Classes III or IV -mild to mod AS,sever PS -Previous myocardial infarction Group III: Major risk of complications or death (mortality >25%) - Sever Pulmonary hypertension - Eisenmenger syndrome - Complex cyanotic heart disease - Sever AS or NYHA class III IV with any valvular disease
 -Pulmonic/tricuspid disease, ASD ,VSD ,PDA. -Bioprosthetic valve ,mild AR, mild PS. -Mitral stenosis, NYHA Class I or II. Group II: Moderate risk of complications (mortality 5% to 15%) - Mitral stenosis with AF. -Artificial valve. -Mitral stenosis, NYHA Classes III or IV. -mild to mod AS,sever PS. -Previous myocardial infarction. Group III: Major risk of complications or death (mortality >25%) - Sever Pulmonary hypertension. - Eisenmenger syndrome. - Complex cyanotic heart disease. - Sever AS or NYHA class III IV with any valvular disease.")
8
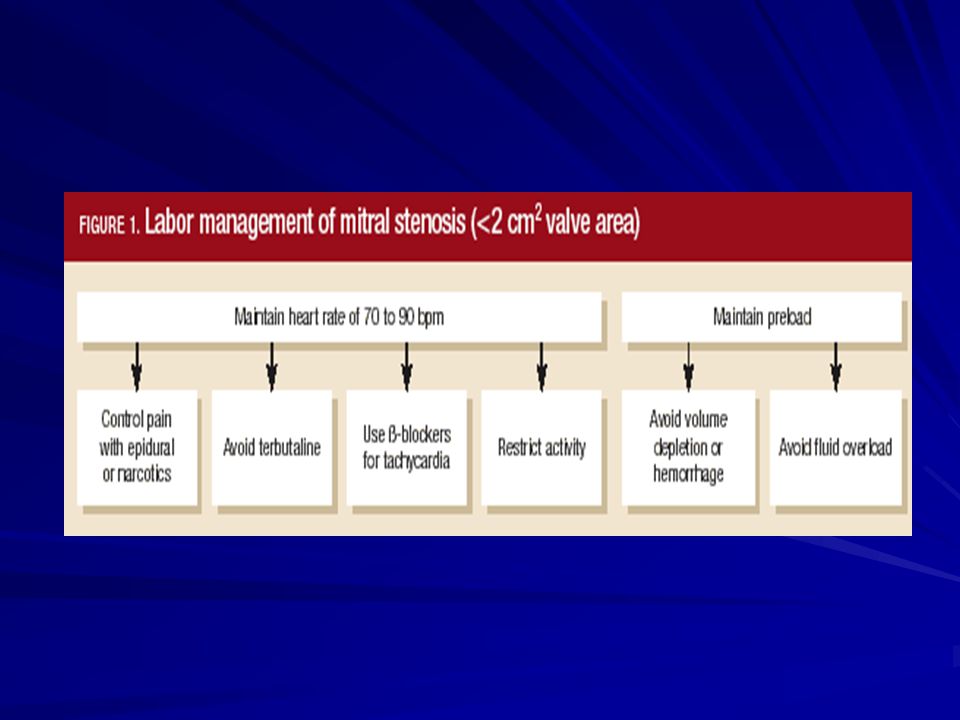
Valvular heart disease and pregnancy 1- mitral stenosis
The most common rheumatic valvular lesion in pregnancy When the valve area falls below 1.5 cm2 filling of the left ventricle during diastole is severely limited, resulting in a fixed cardiac output The pressure gradient across narrowed valve may increase greatly seconadry to increase in HR and blood volume Increased left atrial pressure can result in arrhythmia Decrease serum coloid osmotic pressure and excessive peripartum fluid administration predispose to pulm edema

9
Changes in NYHA class between 1st visit and follow up during pregnancy

10
Theraputic approach Aiming to: reduce heart rate
Decrease left atrial pressure 1- restriction of physical activity 2- drugs as B blockers and digoxin used to control HR 3- cautious use of diuretics Vaginal delivery is permitted in most patients with MS In symptomatic patients with moderate to sever MS continuous monitoring and use of IV dugs like diuretics digoxine BB and nitrates

11
Mitral valve repair or replacement
Should be considered only in sever cases of MS refractory to optimal medical therapy Or when close follow up during pregnancy and labour is not possible Risk of foetal death during surgery is % VS 2-12% in PBMV Epidural anesthesia is the most apprpriate form of analgesia for both vaginal and abdominal delivery

13
2-Mitral regurgitation
Most common causes is rheumatic and myxomatous degeneration MR is well tolerated during pregnancy New AF or sever hypertension can precipitate homodynamic deterioration Women with sever MR are advised to under go surgical repair before conception

14
3-Mitral valve prolapse

15
4-Aortic stenosis AS is far less frequent than MS and most cases are congenital Delivery is safe in patients whose functional tolerance is good Valve repair or termination of pregnancy considered only after Appearance of symptoms like dyspnea, syncope or pulm. Oedema resistant to medical treatment

17
5-Aortic regurgitation
It may be due to bicuspid aortic valve, rheumatic,or infective endocardities It is well tolerated during pregnancy In symptomatic patients diuretics,digoxine and hydralazine can be safely used

18
6-Prothetic valves and pregnant woman
The risk of PV. related to increase in heamodynamic burden and increase incidence of thromboembolism Selection of type of prosthesis should be individualized as The bileaflet mechanical valves more durable, excellent hemodynamic profile, and relatively small risk of thromboembolic and bleeding complications with careful anticoagulation

19
In women who are not interested in anticoagulation or for whom close follow-up is not possible, a tissue valve is preferred In the aortic position, homografts, pericardial valves, and stentless porcine xenografts have not been extensively used in pregnancy The pulmonary autograft (Ross procedure) is an excellent elternative but associated more with structural valve deterioration
 is an excellent elternative but associated more with structural valve deterioration.")
20
Thromboembolic complications Valve thrombosis (%) Emboli (%)
Outcome of pregnancy in women with mechanical or biological prostheses Study No. of pregnancies Live births (%) Thromboembolic complications Valve thrombosis (%) Emboli (%) Mechanical valves Hanania 95 53 11 9 Sbarouni 151 73 5 Born 35 63 8 3 Bioprosthetic valves 60 80 83 25 100 Adapted from Baughman (7).
 Thromboembolic complications. Valve thrombosis (%) Emboli (%) Mechanical valves. Hanania Sbarouni Born Bioprosthetic valves Adapted from Baughman (7).")
21
Conditions warranting anticoagulation during pregnancy
Mechanical prosthetic valve History of venous thromboembolism Acute deep venous thrombosis Antiphospholipid antibody syndrome Inherited deficiency of naturally occuring anticoagulant Chronic AF Eisenmger’s syndrome

22
ACC/AHA Recommendation for Anticoagulation During Pregnancy in Patients With Mechanical Prosthetic Valves 1. The decision whether to use heparin during the first trimester or to continue oral anticoagulation throughout pregnancy should be made after full discussion with the patient and her partner. 2. High-risk women who choose not to take warfarin during the first trimester should receive continuous unfractionated heparin intravenously in a dose to prolong the mid-interval (6 h after dosing) activated PTT time to 2 to 3 × control value. Transition to warfarin can occur thereafter. 3. In patients receiving warfarin, the INR should be maintained between 2.0 and 3.0 with the lowest possible dose of warfarin, and low-dose aspirin should be added. 4. Women at low risk might be managed with adjusted-dose SC heparin (17,500 to 20,000 U twice daily to prolong the mid-interval (6 h after dosing) activated PTT time to 2 to 3 × control value. 5. Warfarin should be stopped no later than week 36 and heparin substituted in anticipation of labor. 6. If labor begins during treatment with warfarin, a cesarean section should be performed. 7. In the absence of significant bleeding, heparin can be resumed 4–6 h after delivery, and warfarin begun orally.
 activated PTT time to 2 to 3 × control value. Transition to warfarin can occur thereafter. 3. In patients receiving warfarin, the INR should be maintained between 2.0 and 3.0 with the lowest possible dose of warfarin, and low-dose aspirin should be added. 4. Women at low risk might be managed with adjusted-dose SC heparin (17,500 to 20,000 U twice daily to prolong the mid-interval (6 h after dosing) activated PTT time to 2 to 3 × control value. 5. Warfarin should be stopped no later than week 36 and heparin substituted in anticipation of labor. 6. If labor begins during treatment with warfarin, a cesarean section should be performed. 7. In the absence of significant bleeding, heparin can be resumed 4–6 h after delivery, and warfarin begun orally.")
25
Anticoagulation options during pregnancy

26
Mode of delivery Vaginal delivery is safe in most cases with PV using epidural anesthesia Invasive heamodynamic monitoring indicated only in sever valve stenosis or HF Heparin should be withdrawn 4 hours before CS or at onset of labor and resumed 6-12 h after In high risk patient with previous endocarditis or heart valve prosthesis prophylactic antibiotics should be given

27
Congenital heart diseases
1- high risk patients Any patient reaches NYHA III,IV is at high risk The situations carries high risk as follow 1- sever pulm. HTN with or without septal defects (maternal mortality 30-50%) 2-sever left ventricular outflow obstruction 3- cyanotic heart diseases with maternal mortality about 2%and incidence of complications of 30% Such as infective endocardities , arrhythmias and CHF
 2-sever left ventricular outflow obstruction. 3- cyanotic heart diseases with maternal mortality about 2%and incidence of complications of 30% Such as infective endocardities , arrhythmias. and CHF.")
28
Treatment of high risk patients
Pregnancy is not recommended If pregnancy occurs termination of pregnancy is advised Physical activity is restricted and bed rest The patient should be hospitalized at the end of 2nd trimester LMWH is given subcutaneous against thromboembolism In sever aortic stenosis balloon valvotomy can relief symptoms it is done in the 2 nd trimester In sever cyanotic heart disease :oxygen sturation,,heamatocrite,and HB monitoring is important

29
2-Low risk patients Patients with small or moderate shunts without pulm, HTN Patients who have had cardiac surgery early in life without prothesis Patients with mild , mod valve regurg. With mild or mod LV out flow tract obstruction Follow up done every trimester

30
Specific conditions 1- pulm stenosis
RVOT obstruction tend to be well tolerated during pregnancy No deaths and low maternal complications 15% have been reported In cases of sever RT ventricular failure balloon valvotomy is the method of choice

31
2- Tetralogy of Fallot Pregnancy in non-operated patient carries a risk for mother and fetus The risk is high when O2 stauration below 85% Close monitoring of BP and gases with avoidance of any further systemic dilatation The risk in good repaired patient is very low All patients with TF should have genetic counseling before conception

32
3- Coarctation of aorta Should be repaired prior to pregnancy
The management of hypertension is difficult in non-operated patient Toxemia doesn’t occur but treatment may cause very low pressure in distal segment This may result in abortion or foetal death Rupture of aorta is the commonest cause of death BB should be prescribed with avoidance of volume excess and CO

33
4-Eisenmenger syndrome
associated with a high risk of maternal morbidity and mortality It is also associated with a poor fetal outcome, with a high incidence of fetal loss, prematurity, intrauterine growth retardation, and perinatal death patients with Eisenmenger syndrome should be advised against pregnancy and early abortion should be recommended

34
Because of increased incidence of peripartum thromboembolism, anticoagulant therapy seems indicated in the third trimester of gestation and for 4 weeks post partum Spontaneous labor is preferred to induction and should lower the chance of prematurely or the need for cesarean section an attempt should be made to shorten the 2nd stage of labor by the use of forceps or vacuum extraction with good oxygenation

35
ANTIBIOTIC PROPHYLAXIS
for vaginal delivery in all patients with CHD (except those with an isolated secundum type of ASD or surgical ligation and division of PDA) seems reasonable
 seems reasonable.")
36
Cardiovascular disorders aquired during pregnancy 1- peripartum cardiomyopathy
(modified criteria for diagnosis ) 1-Development of cardiac failure during pregnancy or within 6 months of delivery 2-Absence of a determinable cause for cardiac failure 3-Demonstrable impairment in left ventricular systolic function
 1-Development of cardiac failure during pregnancy or within 6 months of delivery. 2-Absence of a determinable cause for cardiac failure. 3-Demonstrable impairment in left ventricular systolic function.")
37
ETIOLOGY A distinct etiology of PPCM remains unknown
Nutritional deficiences Myocarditis Infections Autoimmune Idiopathic The incidence of peripartum cardiomyopathy is greater in multiparous women and in those with preeclampsia and twin pregnancies

39
Echocardiography

40
TREATMENT Non-pharmacological Pharmacological Salt restriction (4gm/d)
Water restriction (2 L/D) Pharmacological Pre-load reduction (diuretics, nitrates) After-load reduction (hydralazine, nitrates, amlodipine) ACE-I contraindicated during pregnancy + ionotropes (digoxin, dopamine, dobutamine) Beta-blockers
 Pharmacological. Pre-load reduction (diuretics, nitrates) After-load reduction (hydralazine, nitrates, amlodipine) ACE-I contraindicated during pregnancy. + ionotropes (digoxin, dopamine, dobutamine) Beta-blockers.")
41
Con. TREATMENT Immunosuppressive agents
May be initiated in patients with PPCM and biopsy-proven myocarditis, but efficacy is unclear Empiric immunosuppression, in the absence of evidence of myocarditis, is not currently recommended

42
Figure 3 Cardiac causes of maternal deaths in the UK: confidential enquiry into maternal deaths 1997–99 (total maternal deaths = 409, cardiac deaths = 41).
.")
43
2-Hypertension in Pregnancy
Classification Chronic hypertension Preeclampsia-eclampsia Preeclampsia Superimposed upon chronic hypertension or Renal Disease Gestational hypertension (only during pregnancy) Transient hypertension (only after pregnancy)
 Transient hypertension (only after pregnancy)")
44
A.Chronic Hypertension
Defined as hypertension diagnosed Before pregnancy Before the 20th week of gestation During pregnancy and not resolved postpartum

45
B.Gestational Hypertension
Diagnosis of gestational hypertension: Detected for first time after midpregnancy Gestational Hypertension: Systolic >140 Diastolic>90 No proteinuria If preeclampsia does not develop and BP returns to normal by 12 weeks postpartum, diagnosis is transient hypertension. BP remains high postpartum, diagnosis is chronic hypertension. Proteinurea develops Preeclampsia is diagnosed (25% incidence)
")
46
Drug Therapy of Hypertension in Pregnancy
Example Comment α2-adrenergic blockers Methyldopa Most commonly used. Safety well established. Drug of choice. Beta-blockers Atenolol, Metoprolol Appear safe. Case reports of fetal bradycardia, growth retardataion. α, β blockers Labetolol Appears effacious. Very scant safety data. Arteriolar vasodilators Hydralazine Effacacious and safe during pregnancy and lactation. ACE inhibitors Captopril Absolutely contraindicated during pregnancy due to fetal toxicity. Calcium channel blockers Diltiazem Appear safe, but not as much data to support their use. Diuretics Furosemide Appears safe, but limited efficacy. Sodium nitroprusside Avoid in pregnancy due to potential for fetal thiocyanate toxicity Magnesium sulfate Treatment of choice for prevention of ecclamptic seizures. Adapted from reference 7.

47
Treatment of Acute Severe Hypertension in Pregnancy
SBP > 160 mm Hg and/or DBP > 105 mm Hg Parenteral hydralazine is most commonly used. Parenteral labetalol is second-line drug (avoid in women with asthma and CHF.) Oral nifedipine used with caution. (Short-acting nifedipine is not approved by FDA for managing hypertension.) Sodium nitroprusside may be used in rare cases.
 Oral nifedipine used with caution. (Short-acting nifedipine is not approved by FDA for managing hypertension.) Sodium nitroprusside may be used in rare cases.")
48
C.Preeclampsia-Eclampsia
Diagnosis Gestational Hypertension: Systolic >140 Diastolic>90 Proteinuria is defined as urinary excretion 0.3 g protein or greater in a 24-hour +2 or greater on urine dip specimen

49
Criteria for Severe Preeclampsia
(one or more) Blood Pressure: >160 systolic, >110 diastolic Proteinurea: >5gm in 24 hours, over 3+ urine dip Oligurea: less than 400ml in 24 hours CNS: Visual changes, headache, scotomata, mental status change Pulmonary Edema Epigastric or RUQ Pain: Usually indicates liver involvement
 Blood Pressure: >160 systolic, >110 diastolic. Proteinurea: >5gm in 24 hours, over 3+ urine dip. Oligurea: less than 400ml in 24 hours. CNS: Visual changes, headache, scotomata, mental status change. Pulmonary Edema. Epigastric or RUQ Pain: Usually indicates liver involvement.")
50
Indications for Delivery in Preeclampsia
Gestational age 38 weeks Platelet count < 100,000 cells/mm3 Progressive deterioration in liver and renal function Suspected abruptio placentae Persistent severe headaches, visual changes, nausea, epigastric pain, or vomiting

51
Preeclampsia

52
ARRHYTHMIAS Serious cardiac arrhythmias are uncommon in pregnancy due to the low prevalence of heart disease in women in the reproductive age group Pre-existing arrhythmias may be aggravated and new arrhythmias appear for the first time in pregnancy Arrhythmias occurring in structurally normal hearts are uncommon and usually benign.

53
Tachyarrhythmias such as AF, VT and VF tend to be associated with SHD
DC cardioversion can be safely performed and should not be withheld if the arrhythmia is associated with haemodynamic instability Although no drug is completely safe, digoxin, quinidine, procainamide and adenosine are well tolerated BB are useful agents but use of atenolol, specifically during the first trimester may be associated with intrauterine growth retardation

54
COMPLETE HEART BLOCK it is usually congenital
Patients with CHB may remain asymptomatic during pregnancy and have an uncomplicated labor and delivery without treatment Symptomatic patients with conduction abnormalities treated during pregnancy with either temporary or permanent pacemakers It has been done with electrocardiographic and echocardiographic guidance in some cases to avoid ionizing radiation

55
Coronary artery disease and pregnancy
Familial hyper chlesterolimia, obesity smoking and diabetes is the main factors Acute myocardial infarction during pregnancy is rare, occurring in 0.01 percent of pregnancies Most myocardial infarctions occur during the third trimester in women over age 33 in situ coronary thrombosis, and coronary dissection occur more frequently than classic obstructive atherosclerosis

56
Medical therapy for acute myocardial infarction must be modified in the pregnant patient
Thrombolytic agents increase the risk of maternal hemorrhage substantially to 8% Low dose aspirin and nitrates..BB Short-term heparin generally are safe. (ACE) inhibitors and statins are contraindicated Hydralazine and nitrates may be used as substitutes for ACE inhibitors.
 inhibitors and statins are contraindicated. Hydralazine and nitrates may be used as substitutes for ACE inhibitors.")
57
Drug therapy in pregnancy
Balancing act maternal treatment fetal effects Little scientific evidence

58
Maternal fetal transfer
Placental transfer Drugs & metabolites in fetus Fetal GI absorption Transfer via breastmilk

59
Drug Use Potential Side Effects Safe Use During Breastfeeding
Cardiovascular Drugs In Pregnancy Drug Use Potential Side Effects Safe Use During Breastfeeding Adenosine Arrhythmia None reported Yes No data Amiodarone IUGR, prematurity, hypothyroidism No ACE inhibitors Hypertension Oligohydramnios, IUGR, PDA, prematurity, neonatal hypotension, renal failure, anemia, death, musculoskeletal abnormalities Ok Beta-blockers Hypertension, arrhythmias, MI, ischemia, HCM, hyperthyroidism, mitral stenosis, Marfan syndrome, cardiomyopathy Fetal bradycardia, low birth weight, hypoglycemia, respiratory depression; prolonged labor Digoxin Arrhythmia, CHF Low birth weight, Prematurity Diuretics Hypertension, CHF Reduced utero- placental perfusion Unclear Flecainide ? fetal death; limited data Limited data Lidocaine Arrhythmia, anesthesia Neonatal CNS depression Low Molecular Weight Heparin Mechanical valve, hypercoaguable state, DVT, AF, Eisenmenger syndrome Hemorrhage, unclear effects on maternal bone mineral density Nitrates Fetal distress with maternal hypotension

60
Hypertension, aortic dissection Fetal thiocyanate toxicity
Procainamide Arrhythmia None reported Yes Ok Sodium nitroprusside Hypertension, aortic dissection Fetal thiocyanate toxicity Potentially unsafe No data Sotalol Fetal bradycardia, IUGR Limited data Unfractionated Heparin Mechanical valve, hypercoagulable state, DVT, AF, Eisenmenger syndrome Maternal osteoporosis, hemorrhage, thrombocytopenia, thrombosis Warfarin Warfarin embryopathy, fetal CNS abnormalities, hemorrhage Yes—after the 12th week of gestation IUGR = intrauterine growth retardation, ACE = angiotensin converting enzyme, PDA = patent ductus arteriosus, MI = myocardial infarction, HCM = hypertrophic cardiomyopathy, CHF = congestive heart failure, CNS = central nervous system, DVT = deep venous thrombosis, AF = atrial fibrillation

61
Infective endocarditis
although it is rare complication in pregnancy, causes mortality in 10–30% of those affected The development of a new cardiac murmur is common in pregnancy and can make the diagnosis of endocarditis difficult predisposing factors in young women include MVP, CHD and intravenous drug abuse The use of antibiotic prophylaxis during uncomplicated deliveries remains controversial prophylaxis only for women who are at high risk is recommended

62
Antibiotic prophylaxis is recommended for the following:
High-risk category Prosthetic cardiac valves, including bioprosthetic and homograft valves Previous bacterial endocarditis Complex cyanotic congenital heart disease (e.g., single ventricle states, transposition of the great arteries, tetralogy of Fallot) Surgically constructed systemic pulmonary shunts or conduits
 Surgically constructed systemic pulmonary shunts or conduits.")
63
Moderate-risk category
Most other congenital cardiac malformations (other than above and below) Acquired valvular dysfunction (eg, rheumatic heart disease) Hypertrophic cardiomyopathy Mitral valve prolapse with valvular regurgitation and/or thickened leaflets Endocarditis prophylaxis is not recommended for the following: (no greater risk than the general population) Isolated secundum atrial septal defect
 Acquired valvular dysfunction (eg, rheumatic heart disease) Hypertrophic cardiomyopathy Mitral valve prolapse with valvular regurgitation and/or thickened leaflets. Endocarditis prophylaxis is not recommended for the following: (no greater risk than the general population) Isolated secundum atrial septal defect")
64
Surgical repair of ASD, VSD, or PDA
Previous coronary artery bypass graft surgery MVP without valvular regurgitation Physiologic, functional, or innocent heart murmurs Previous Kawasaki disease without valvar dysfunction Previous rheumatic fever without valvar dysfunction Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
 and implanted defibrillators.")
65
High-risk patient who has penicillin allergy
Recommended antibiotic prophylaxis for high-risk women undergoing genitourinary or gastrointestinal procedures Category Drug and dosage High-risk patient Ampicillin, 2 g IM or IV, plus gentamicin sulfate (Garamycin), 1.5 mg/kg IV 30 min before procedure; ampicillin, 1 g IV, or amoxicillin (Amoxil, Trimox, Wymox), 1 g 6 hr after procedure High-risk patient who has penicillin allergy Vancomycin HCl (Vancocin, Vancoled), 1 g IV over 2 hr, plus gentamicin sulfate, 1.5 mg/kg IV 30 min before procedure
, 1.5 mg/kg IV 30 min before procedure; ampicillin, 1 g IV, or amoxicillin (Amoxil, Trimox, Wymox), 1 g 6 hr after procedure. High-risk patient who has penicillin allergy. Vancomycin HCl (Vancocin, Vancoled), 1 g IV over 2 hr, plus gentamicin sulfate, 1.5 mg/kg IV 30 min before procedure.")
66
Anaesthesia during pregnancy
The choice of anesthesia depends on circumstances of the delivery and maternal cardiac status Epidural anesthesia is well tolerated and provides effective analgesia. -It minimize HR and BP changes associated with inadequate pain relief. With cautious fluid preloading, gradual increments in drug dosages and positioning in the lateral position, -It should still be used with extreme caution in those with restricted cardiac output or right-to-left shunts.

67
summary Women at low risk are those who have few or no symptoms and good LV function Those of high risk need to be managed within or from a cardiac center The mode and time of delivery should be discussed and vaginal delivery usually advised Antibiotic prophylaxis is not advised for a normal delivery

68
Thank you

Similar presentations










 Blood pressure ↓ Fall in TM 1 and 2, returns to baseline.>")











 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C Designed At A.V. Dept. F.J.M.C. By.>")