Download presentation
Presentation is loading. Please wait.

1
Body Fluids Total Body Water = Extracellular Fluid (ECF) + Intracellular Fluid (ICF) ECF = Plasma + Interstitial Fluid Total Body Water expressed in terms of % body weight (adolescent or adult): ICF (30-40%) Interstitial(15%) Plasma5% & Infants- 8%
 + Intracellular Fluid (ICF) ECF = Plasma + Interstitial Fluid Total Body Water expressed in terms of % body weight (adolescent or adult): ICF (30-40%) Interstitial(15%) Plasma5% & Infants- 8%")
3
Change in Body Composition

5
dehydration Child: Mild- 5% weight loss Moderate 10 15-severe or shock 3%/6%/9% old child & adults

6
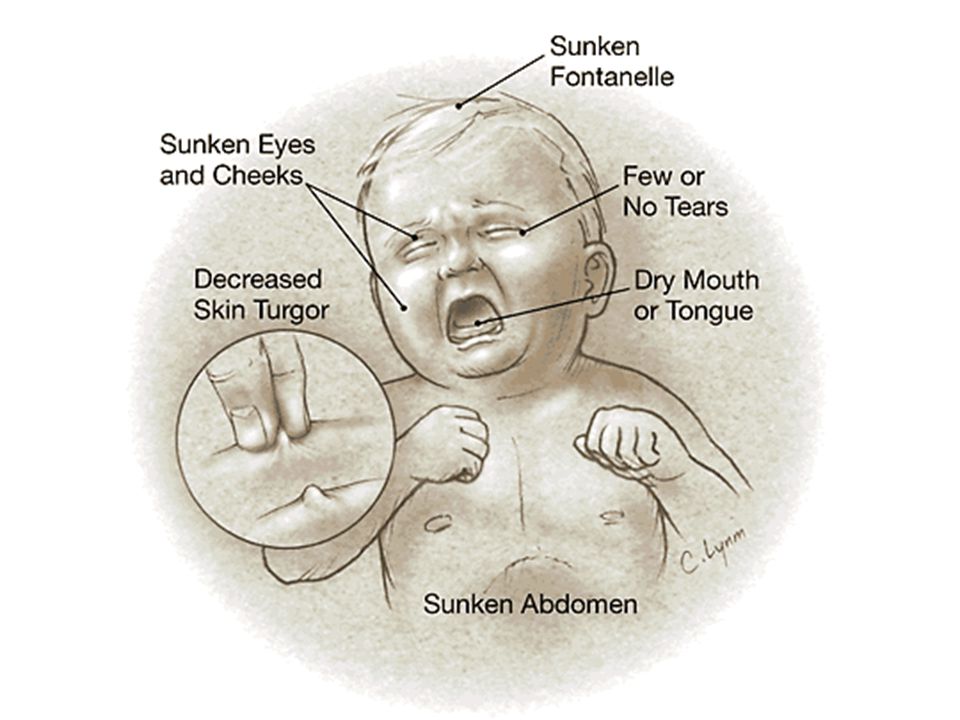
dehydration Mild: thirsty, minimal clinical picture Moderate: tachycardia, sunken eyes, dry mucous membranes, depressed fontanel, decreased urination (???- only 20% of "oliguric" patients have dehydration!), ± prolonged capillary refill Severe: blood pressure drop
, ± prolonged capillary refill Severe: blood pressure drop")
10
dehydration Isotonic dehydration hypertonic (Na≥150) hypotonic (Na≤130)
 hypotonic (Na≤130)")
12
dehydration Acute< 3 days 75-100% of fluids losses is from ECF (primarily Na loss, less K loss) Subacute or chronic> 3 days 65-70% of losses from ECF and 30% from ICF with greater level of potassium loss
 Subacute or chronic> 3 days 65-70% of losses from ECF and 30% from ICF with greater level of potassium loss")
13
Treatment of dehydration Fluids!!!!! Etiologic treatment

14
Treatment of dehydration Rout of fluids administration: enteral and parenteral

15
Treatment of dehydration Oral/PZ- preferable & most physiologic type – Hypotonic type: ORS by 40-60meq Na/20 meq K and 2.5D for non choleric patients – Medium type: 70meq Na – High solute type: 60-90Na for cholera 1 cc/kg for mild and 2cc/kg for moderate dehydration for 4 h every 5 minutes

17
Dehydration treatment Oral rehydration contraindications: intractable vomiting impaired consciousness aspirations risk bowel obstruction

18
Treatment of dehydration Parenteral: – Subcutaneous with recombinant hyaluronidase adjuvant – IV/io for failed ORS or Moderate-Severe dehydration

19
IV dehydration correction 3 phases – Emergent – Corrections – Maintenance and ongoing losses

20
Emergent phase of fluid replacement correction of perfusion failure and intravascular deficit by bolus of isotonic fluids 0.9 NaCl±D5 or Ringer lactate 20ml/kg (previous mass!) Bolus- within minutes! Repeat boluses until stable

21
Emergent phase Patient with decreased oncotic pressure (nephrotic syndrome, protein-loosing entheropathy, burns, cirrhosis)- may give 5% albumin DKA- start 10 ml/kg Premature and small newborns- 10 ml/kg Suspected cardiogenic shock – 10ml/kg
- may give 5% albumin DKA- start 10 ml/kg Premature and small newborns- 10 ml/kg Suspected cardiogenic shock – 10ml/kg")
22
Second phase- deficits correction Deficits: H 2 O+ Na+ K± Ca

23
Deficits correction Assess degree of dehydration Assess type of dehydration Assess length of dehydration

24
Deficits correction FIRST - calculate the amount of fluid you need NEXT - calculate how much sodium and potassium you need FINALLY - pick a fluid based upon what is commercially available if you can

25
Deficits correction Persistent deficits= previous loss- boluses Most accurate method of water deficit estimation- weight loss Other method: Calculated previous weight- current weight Calculated weight= current+ estimated fluid loss Estimated fluid loss- by percent of dehydration

26
Isotonic dehydration Water deficit- weight loss or estimated weight loss Sodium deficit

27
Isotonic dehydration sodium deficit total body water(normal)*140meq/l- current TBW*current [Na]= Na deficit
![Isotonic dehydration sodium deficit total body water(normal)*140meq/l- current TBW*current [Na]= Na deficit](http://images.slideplayer.com/13/4064127/slides/slide_27.jpg "Isotonic dehydration sodium deficit total body water(normal)*140meq/l- current TBW*current [Na]= Na deficit")
28
Isotonic dehydration Normal TBW= normal body mass*K k~0.75 neonates, 0.65 toddlers, 0.6w &0.5m ??????Really Current TBW~ current mass (k- estimated percent of dehydration/10)
")
29
10 kg infant with 10% dehydration- 1l loss Sodium deficit= 1*140 meq/ml Sodium maintenance= 3meq/100 ml of water*daily fluids

30
Isotonic dehydration Replacement and maintenance by isotonic or ½ NS based fluids Give 100-70% of deficit at 1 st day Give 1 st half of day fluids amount at 1 st 8h and rest at 16h New recommendations- to give NS based fluids to prevent iatrogenic hyponatremia

31
Ongoing Repletion and Maintenance Therapy Once the patient is stable Persistent deficits+ ongoing losses+ maintenance fluids

32
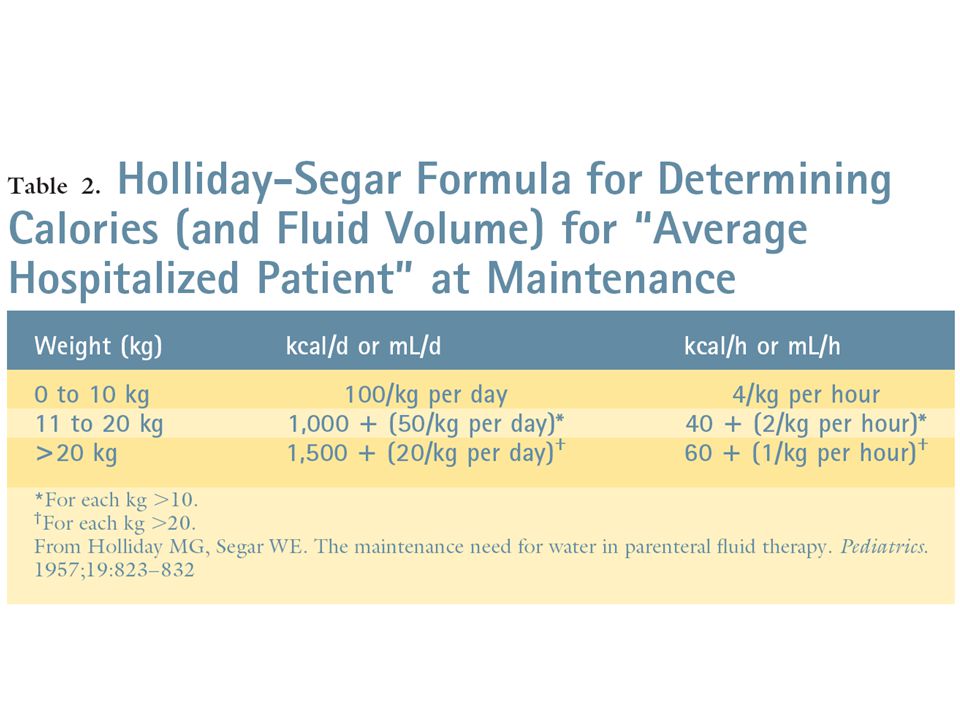
Fluid maintenance: Holliday Segar formula 1 st 10kg- 100 ml/kg 2 nd 10kg- 50ml/kg Others- 20ml/kg ~400 ml/m²/d+ renal sensible loss

34
Caloric (energy) maintenance The daily fluid requirement is the same as the daily caloric requirement (e.g., if a child requires 1000 cc fluid, he also requires 1000 Kcalorie In terms of fluids, calories most often provided as dextrose (glucose) Difficult to provide total daily caloric requirement intravenously unless using TPN Most often, it is sufficient to provide 20% of total daily caloric requirement intravenously so as to prevent ketosis
 maintenance The daily fluid requirement is the same as the daily caloric requirement (e.g., if a child requires 1000 cc fluid, he also requires 1000 Kcalorie In terms of fluids, calories most often provided as dextrose (glucose) Difficult to provide total daily caloric requirement intravenously unless using TPN Most often, it is sufficient to provide 20% of total daily caloric requirement intravenously so as to prevent ketosis")
35
Ongoing loses Sensible: diuresis and diarrhea (rectal tube) Insensible: feces, skin, respiration 10ml/kg for each diarrhea Burns- Parkland formula: BSA*4*mass for >20% of TBS of 2 nd degree and > Tachypnea: 5-10ml/kg/10resp> normal Hyperthermia: 5-10 ml/kg/1°>38 Vomiting:5-10 ml/kg/event
 Insensible: feces, skin, respiration 10ml/kg for each diarrhea Burns- Parkland formula: BSA*4*mass for >20% of TBS of 2 nd degree and > Tachypnea: 5-10ml/kg/10resp> normal Hyperthermia: 5-10 ml/kg/1°>38 Vomiting:5-10 ml/kg/event")
36
Decreased maintenance SIADH Ventilated children Inactive/hypothermic children

37
Example of isotonic dehydration 1y boy with moderate dehydration

38
Water and sodium (Na) deficits simple calculation: loss of 1 l of isotonic fluids Water deficit: 10 kg × 10% = 1 L Na deficit: 1 L × 140 mEq/L = 140 mEq
 deficits simple calculation: loss of 1 l of isotonic fluids Water deficit: 10 kg × 10% = 1 L Na deficit: 1 L × 140 mEq/L = 140 mEq")
39
Emergent fluid repletion with NS or D5% NS 20 mL/kg × 10 kg = 200 mL (200 mL water and ≈30 mEq sodium)
")
40
Ongoing repletion and maintenance requirements Remaining water deficit: 1,000 mL - 200 mL = 800 mL Daily maintenance water requirement: 100 mL/kg/day × 10 kg = 1,000 mL/day 800 mL + 1,000 mL = 1,800 mL/24 h = 75 mL/h Remaining Na deficit: 140 mEq - 30 mEq = 110 mEq Maintenance sodium requirement: 3 mEq/100 mL water × 1,000 mL/day = 30 mEq/day 110 mEq + 30 mEq = 140 mEq/24 h 140 mEq/1,800 mL ≈ 0.45% sodium chloride (½ NS)
")
41
Maintenance potassium requirement: 3 mEq/100 mL water × 1,000 mL/day = 30 mEq/day 30 mEq/1,800 mL ≈15–20 mEq/L Intravenous fluid based upon deficit calculations: D5% 1/2 NS with 20 mEq/L KCl at 75 mL/h

42
Ongoing losses Extrarenal losses should be replaced mL-for-mL if volumes are significant. The sodium content of the fluid lost should be estimated or measured in order to select the appropriate replacement fluid.

43
Hyponatremic (125) dehydration example Water and sodium deficits Water deficit: 10 kg × 10% = 1 L Sodium deficit: [TBW(n) × 140 mEq/L] - [TBW(c) × 125 mEq/L] TBW(n) = 10 kg × 0.65 = 6.5 L TBW(c) = TBW(n) - water deficit = 6.5 L - 1 L = 5.5 L Sodium deficit: (6.5 L × 140 mEq/L) - (5.5 L × 125 mEq/L) ≈ 220 mEq
![Hyponatremic (125) dehydration example Water and sodium deficits Water deficit: 10 kg × 10% = 1 L Sodium deficit: [TBW(n) × 140 mEq/L] - [TBW(c) × 125 mEq/L] TBW(n) = 10 kg × 0.65 = 6.5 L TBW(c) = TBW(n) - water deficit = 6.5 L - 1 L = 5.5 L Sodium deficit: (6.5 L × 140 mEq/L) - (5.5 L × 125 mEq/L) ≈ 220 mEq](http://images.slideplayer.com/13/4064127/slides/slide_43.jpg "Hyponatremic (125) dehydration example Water and sodium deficits Water deficit: 10 kg × 10% = 1 L Sodium deficit: [TBW(n) × 140 mEq/L] - [TBW(c) × 125 mEq/L] TBW(n) = 10 kg × 0.65 = 6.5 L TBW(c) = TBW(n) - water deficit = 6.5 L - 1 L = 5.5 L Sodium deficit: (6.5 L × 140 mEq/L) - (5.5 L × 125 mEq/L) ≈ 220 mEq")
44
Emergent fluid repletion with NS or D5%NS 20 mL/kg × 10 kg = 200 mL (200 mL water and ≈30 mEq sodium)
")
45
Ongoing repletion and maintenance requirements Remaining water deficit: 1,000 mL - 200 mL = 800 mL Daily maintenance water requirement: 100 mL/kg/day × 10 kg = 1,000 mL/day 800 mL + 1,000 mL = 1,800 mL/24 h = 75 mL/h Remaining Na deficit: 220 mEq - 30 mEq = 190 mEq Maintenance Na requirement: 3 mEq/100 mL water × 1,000 mL/day = 30 mEq/day 190 mEq + 30 mEq = 220 mEq 220 mEq/1,800 mL ≈120 mEq/L

46
Maintenance potassium requirement: 3 mEq/100 mL water × 1,000 mL/day = 30 mEq/day 30 mEq/1,800 mL ≈15–20 mEq/L KCl Intravenous fluid based upon deficit calculations: D5% with 120 mEq/L Nacl and 20 mEq/L KCl at 75 mL/h D5%NS with added potassium could be provided for the initial half of the total volume and completed with D5%1/2 NS with added potassium

47
Hypernatremic dehydration example Total Fluids loss= free water losses+ isotonic fluids losses FreeH2O deficit = TBW(c) × [(serum Na/140) - 1] Total fluid deficit- free water deficit= isotonic losses
![Hypernatremic dehydration example Total Fluids loss= free water losses+ isotonic fluids losses FreeH2O deficit = TBW(c) × [(serum Na/140) - 1] Total fluid deficit- free water deficit= isotonic losses](http://images.slideplayer.com/13/4064127/slides/slide_47.jpg "Hypernatremic dehydration example Total Fluids loss= free water losses+ isotonic fluids losses FreeH2O deficit = TBW(c) × [(serum Na/140) - 1] Total fluid deficit- free water deficit= isotonic losses")
48
Water and sodium deficits Total water deficit: 10 kg × 10% = 1 L TBW(c) = TBW(n) - 1L = (10 kg × 65%) - 1 L = 5.5L Free water deficit: TBW(c)[(155/140) - 1] = 5.5[(155/140) - 1] = 0.59 L Isotonic deficit = total water deficit - free water deficit = 0.41 L Sodium deficit: 0.41 L × 140 mEq/L ≈ 60 mEq
![Water and sodium deficits Total water deficit: 10 kg × 10% = 1 L TBW(c) = TBW(n) - 1L = (10 kg × 65%) - 1 L = 5.5L Free water deficit: TBW(c)[(155/140) - 1] = 5.5[(155/140) - 1] = 0.59 L Isotonic deficit = total water deficit - free water deficit = 0.41 L Sodium deficit: 0.41 L × 140 mEq/L ≈ 60 mEq](http://images.slideplayer.com/13/4064127/slides/slide_48.jpg "Water and sodium deficits Total water deficit: 10 kg × 10% = 1 L TBW(c) = TBW(n) - 1L = (10 kg × 65%) - 1 L = 5.5L Free water deficit: TBW(c)[(155/140) - 1] = 5.5[(155/140) - 1] = 0.59 L Isotonic deficit = total water deficit - free water deficit = 0.41 L Sodium deficit: 0.41 L × 140 mEq/L ≈ 60 mEq")
49
Emergent fluid repletion with NS or D5%NS 20 mL/kg × 10 kg = 200 mL (200 mL water and ~30 mEq sodium)
")
50
Ongoing repletion and maintenance requirements Remaining total water deficit: 1,000 mL - 200 mL = 800 mL, plan to replace over 36–48 h or 400 mL/day × 2 days Daily maintenance water requirement: 100 mL/kg/day × 10 kg = 1,000 mL/day 1,000 mL + 400 mL = 1,400/24 h or ≈60 mL/h Remaining sodium deficit: 60 mEq - 30 mEq = 30 mEq Maintenance sodium requirement: 3 mEq/100 mL of water intake × 1,000 mL/day = 30 mEq/day Total sodium requirement: 30 mEq + 30 mEq = 60 mEq 60 mEq/1,400 mL or ≈0.225% sodium chloride

51
Maintenance potassium requirement: 3 mEq/100 mL water × 1,000 mL/day = 30 mEq/day 30 mEq/1,400 mL ≈20 mEq/L KCl D5% 1/4 NS with 20 mEq/L KCl at 60 mL/h for ~36–48 h

52
Correct sodium 10-12 mEq/l per 24 h Acute states- rate may be higher Chronic state- decrease the rate of correction Estimate the rate of correction by planning of free water deficit replacement

53
Sodium Predominant solute of extracellular space Concentration inversely related to total body water Osmotic gradient Membrane potential Normal measured concentration: 135-145 Measured Na+ (0.016*serum glucose (mg/dL)= Corrected serum Na Other pseudohyponatremias- hyperlipidemia & paraproteinemia
= Corrected serum Na Other pseudohyponatremias- hyperlipidemia & paraproteinemia")
54
sodium Normal intake: 2-3 meq/kg/d

56
Signs of hypernatremia 145- 150-158- mild/moderate signs – Intense thirst – restlessness

57
Severe hypernatremia 158–160 mmol/l severe signs due to rupture of brain vessels especially in rapid developed hypernatremia due to brain volume fall with subsequent brain separation from meninx

58
Severe hypernatremia – Absent thirst – altered mental status – anorexia – muscle weakness – nausea – vomiting – lethargy – irritability – Stupor or coma – vascular rupture with cerebral bleeding and subarachnoid hemorrhages

59
Chronic hyperNa- minimal neurological symptoms due to neuronal adaptation by osmolytes (amino acids and carbohydrates) production within 72 h- don’t repair rapidly to prevent brain edema
 production within 72 h- don’t repair rapidly to prevent brain edema")
60
correction 1 st step- correct intravascular volume depletion by bolus A & B stabilisation For acute hypernatremia- acute correction 1 mmol/h For hypernatremia of longer or unknown duration- slow correction 0.5 mmol/h till145

62
Anorexia Headache Nausea Vomiting Irritability Disorientation Weakness & cramps- rhabdomyolisis Seizures and coma due to cerebral edema in case of rapidly progressive hyponatremia Death

63
1 st tx step- volume replacement by isotonic fluids especially in hemodinamically unstable patient + A& B stabilization including intubation and seizures control

64
Correction: 8–12 mmol/l/d for chronic hyponatremia to prevent demyelination

65
Mechanism of demyelination: rapid osmolarity repair→ fluid efflux from brain blood barrier endothelium→ endotheliocytes constriction→ opening pores in BBB→ plasma inflammatory substances (TNF & interferon) attack of glya Acute tx for acute severe hyponatremia (symptomatic): start after hemodynamic stabilization 4-6 ml/kg NaCl3% bolus
 attack of glya Acute tx for acute severe hyponatremia (symptomatic): start after hemodynamic stabilization 4-6 ml/kg NaCl3% bolus")
66
Water restriction and loop diuretics+ salt supplements in neurologically intact or hypervolaemic patient without fluid resuscitation Water restriction in euvolaemia

68
Signs Muscular: Usually ascending doesn’t involve respiratory muscles- DD with hypo K appears then K>8 Fatigue Weakness Paresthesia muscular paralysis/tetany

69
Cardiac: Peaked T- earliest ECG sign 2 nd - flat P prolonged PR/QRS, BBB, VF, asystole

73
The rapider K rises the severer clinical picture Hyponatremia, acidosis, hypoCa- more rapid and sever clinical picture Pseudo hyperkalemia: serum K- plasma K> 0.3 mmol

74
treatment Ca to prevent arrhythmia Insulin +D Bicarbonate Ventoline Key oxalate diuretics

76
signs Mild 3.0-3.5 mmol/l- arrhythmia in cardiac patients

77
Moderate 3- 2.5: ascending muscle weakness & diaphragmatic paralysis hypertension paralytic ileus flat or inverted T; ST depression prominent U-waves atrial tachycardia± block atrioventricular dissociation VT/F/SVT especially on digitalis

78
Severe< 2.5: Myopathy Rhabdomyolysis ascending paralysis respiratory failure myocardial necrosis constipation urinary retention and voiding dysfunction

Similar presentations