Download presentation
Presentation is loading. Please wait.

1
Keri T. Holmes-Maybank, MD Medical University of South Carolina June 18, 2013

2
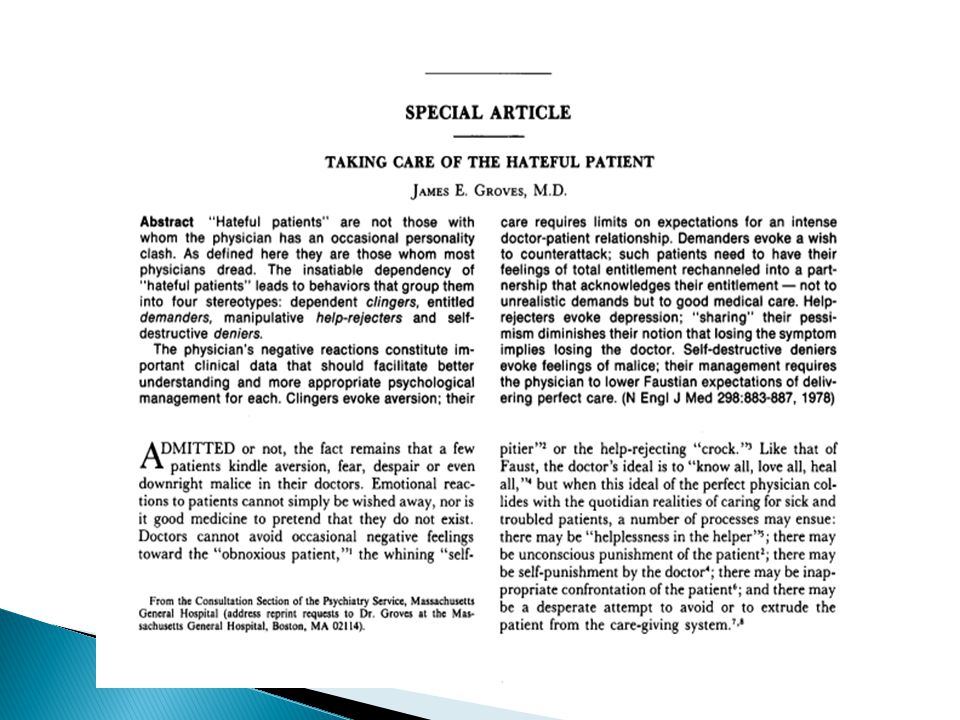
Review the famous Groves article “Taking care of the hateful patient.” Recognize physician characteristics that lead to a greater perception of a patient as “difficult.” Recognize patient characteristics and patterns of behavior classified as “difficult.” Practice the collaboration, appropriate use of power, and empathy approach recommended for managing conflict by Elder.

3
Illness can alter the patient’s psyche leading to uncharacteristic behavior. Acknowledge and accept emotional responses to patients. Physician awareness and acceptance of personal emotions may improve emotional intelligence and physician-patient relationships. Most important is how the physician behaves toward the patient, not the emotion she is experiencing. Empathy and collaboration are the keys to effective conflict management.

5
Dependent Clinger Entitled Demander Manipulative Help Rejecter Self Destructive Denier

6
Appropriate need for reassurance Escalates to unreasonable, BOTTOMLESS need for explanation, affection, and attention Constant reassurance Increasing dependency See MD as inexhaustible resource Warning signs: Extreme gratitude MD feels special

7
MD becomes exhausted, patient feels rejected, ramp up needy behavior with more desperate attempts at contact Repugnance Dislike AVERSION

8
Empathy Set limits early without feeling inhuman, without patient feeling deceived or disappointed Difficult to refer to psychiatrist Interpret as abandonment/rejection Reassure you will still see them

9
Overtly hostile, superior Intimidation, devaluation, induce guilt Control by threatening punishments ◦ Withholding payment, demands for more tests/consults, or litigation Lack of control Compensation for MD power/knowledge Ultimately fear abandonment Entitlement = faith and hope in well-adjusted

10
Fear Depression Wish to counterattack

11
Do NOT debate or belittle Acknowledge entitlement to have realistic good care Very respectfully and non-confrontationally to explain how behavior may compromise health Cooperative decision-making process Rechannel energy into following the regimen

12
Smugly satisfied with failure Do not want cure, want unending relationship with MD No regimen will help Pessimism increases with MD’s efforts and enthusiasm Manipulation Want MD close but keep them at significant distance - fear Relationship will not end if they have symptoms Deny assistance/advice while spiraling into poor health

13
Anxiety treatable illness being missed, then irritation, then depression and self-doubt Guilty Inadequate Demoralized Depression Unproductive, time-consuming, exhausting

14
Don’t accuse of manipulation = doctor shopping Share pessimism – say treatment may not be curative Consistent, firm limitations – unrealistic expectations or demands Regular follow-up Patient’s fear of abandonment put to rest

15
Simple explanations Hard to refer to psychiatrist Make sure they have follow-up with MD Empathy Patient education Encouragement and support

16
Unconscious self-murderous/injurious behaviors Spiral of self-destruction while requesting assistance Glory own destruction Pleasure in defeating MD attempts to preserve life Profoundly dependent Self-hate, project hate through the MD

17
MD caught between ideal of saving patient and unwanted wish for patient to die Malice Objectivity challenged by hatred, or indifference (protects MD emotionally)
")
18
MD limited because patient will only allow so much care All reasonable care for patient Compassion – terminal illness Do not abandon Recognize without shame the feelings the patient provoke in MD Cannot give perfect care

19
Physician develops positive or negative feelings toward patient based upon personal experiences in her life Use it to gain knowledge about where patient is coming from

20
Patient feels threatened = behavioral regression Projects these feelings onto MD Patient feels relieved when these feelings are reflected by MD Example: Patient feels helpless = complains incessantly = MD feels helpless If MD recognizes can react supportively

21
Patient autonomy Patients more educated Boundaries are being crossed by email and info about physicians on internet Defensive medicine

22
Productivity pressures Changes in health care financing Fragmentation of visits Interrupted visits Outside information sources challenge the physicians authority Less trust in their physicians Feel rushed or ignored may repeat themselves or prolong visit 18% of encounters classified as “difficult”

23
Greater perceived workload/overwork Lower job satisfaction Lack of training in communication/poor communication skills Inexperience Discomfort with uncertainty Poor attitude

24
Professional identity ◦ I am unable to make better *** ◦ Conflicts with my professional standards Personal qualities ◦ Feel taken advantage of ◦ Difficulty making relationship with patient Time management ◦ Takes too much time Comfort with patient autonomy ◦ Patient sets the agenda Confidence in skills ◦ Too hard to solve Trust in patient ◦ Lose trust in patient

25
Increased dissatisfaction with services Become more demanding Repeated visits without medical benefit Seemingly endless complaints Unmet expectations Insatiable dependency Report worsening symptoms

26
Do not seem to want to get well Power struggles Focus on issues seemingly unrelated to medical care Worried every symptom represents a serious illness Reported greater symptom severity Chronic pain (+/- narcotics)
")
27
Psychiatric ◦ Axis II ◦ Depression ◦ Somatization (alcohol, borderline) ◦ Mood d/o (insist on physical cause) ◦ Anxiety (multi complaints, think cardiac, not enough being done) Lower social class Female Thick clinical records Older More medical problems Greater use of health care services Poor functional status
 ◦ Mood d/o (insist on physical cause) ◦ Anxiety (multi complaints, think cardiac, not enough being done) Lower social class Female Thick clinical records Older More medical problems Greater use of health care services Poor functional status")
28
Cluster A (odd or eccentric, fears social relations) ◦ Paranoid ◦ Schizoid ◦ Schizotypal Cluster B (dramatic, emotional erratic disorders) ◦ Antisocial ◦ Borderline ◦ Histrionic ◦ Narcissistic Cluster C (anxious or fearful disorder) ◦ Avoidant ◦ Dependent ◦ Obsessive-compulsive Appendix B ◦ Depressive ◦ Passive-aggressive (negativistic)
 ◦ Paranoid ◦ Schizoid ◦ Schizotypal Cluster B (dramatic, emotional erratic disorders) ◦ Antisocial ◦ Borderline ◦ Histrionic ◦ Narcissistic Cluster C (anxious or fearful disorder) ◦ Avoidant ◦ Dependent ◦ Obsessive-compulsive Appendix B ◦ Depressive ◦ Passive-aggressive (negativistic)")
29
DissatisfactionDifficult patients Not- difficult Physician's technical competence9%1%P<.001 Bedside manner7%0.7%P<.001 Time spent with clinician13%3%P=.002 Explanation of what was done12%3%P<.001 Higher number of visits42P=.004 Jackson, JL, Kroenke K. Difficult Patient Encounters in the Ambulatory Clinic: Clinical Predictors and Outcomes Arch Intern Med. 1999;159(10):1069-1075.
:")
30
Helpless Inadequacy Frustration Anger Guilt Dislike

31
Leads to: ◦ Unconscious punishment of the patient ◦ Self-punishment by the doctor ◦ Inappropriate confrontation ◦ Desperate attempt to avoid patient ◦ Errors in diagnosis or treatment ◦ Decreased quality of care ◦ Work burdensome ◦ Burnout

32
Disproportionate emotional energy can be spent dealing with negative feelings Strong negative emotional reaction is important clinical data about patient’s psychology (personality d/o) Sensitivity to MD feelings ◦ Improved physician well being ◦ Less destructive patient behavior ◦ Lower risk of litigation
 Sensitivity to MD feelings ◦ Improved physician well being ◦ Less destructive patient behavior ◦ Lower risk of litigation")
33
Collaboration Appropriate use of MD power Empathy

34
Priority setting ◦ Prioritize patient concerns Diagnostic skills ◦ Thorough history, physical, and testing Decision making ◦ Explain ◦ Be consistent and objective ◦ Be honest and fair ◦ Facilitate patient decision making Team approach ◦ Use referrals (mental health, pain, etc.) ◦ Enlist/see family ◦ Provide quality care Coaching ◦ Set small, achievable goals ◦ Short term symptom relief
 ◦ Enlist/see family ◦ Provide quality care Coaching ◦ Set small, achievable goals ◦ Short term symptom relief")
35
Encourage patient to start taking responsibility Think of their care as a team effort Adjust expectations of what can be accomplished Patient education Collaboration has most impact on clinical interaction

36
Set clinical management rules ◦ Schedule patient frequently, longer visits ◦ Clinic time management ◦ Good documentation Set boundaries and limits ◦ Set general limits ◦ Make explicit rules when necessary ◦ Limit number of patient concerns ◦ Limit time at each visit

37
Understand patients psyche Focus on patient emotions Compassionate and firm Patient centered Reinforce positives Keep professional distance

38
Protects MD from developing negative responses to difficult and challenging behavior Allows insight into patient issues and why patient has resorted to negative response patterns ◦ Illness can alter patients – uncharacteristic, childlike Creates an environment conducive to more suitable health care delivery, a healthier lifestyle, better work satisfaction

39
Point person - may get conflicting info from consultants Tactful assessment of patient’s distress/emotion LISTEN Interrupt less Regular, brief summaries of patient’s concerns Reconcile conflicting views of diagnosis/illness

40
Acknowledge problem Both parties may contribute to difficulty Use communication skills You can discuss that have poor relationship: “How do you feel about the care you are receiving from me?” “It seems to me we sometimes don’t work together very well.” Use “I” statements ◦ “I feel it’s difficult for me to listen to you when you use that kind of language.”

41
1. ***Does my patient prioritize health?*** ◦ Not if patient works with MD to prevent and treat disease. ◦ Unpleasantness alone is not grounds. 2. Is confrontation of my patient ethically permissible? ◦ If patients self-corrosive decisions come with expectations of accommodation. ◦ If MD bearing majority of burden in failing treatment. ◦ If health deteriorating from patient action or inaction. 3. What if confronting my patient is emotionally gratifying? ◦ Recognize countertransference v. projective identification. ◦ Assess motives and emotions in real time and discuss with a peer.

42
Butler CC, Evans M. The “heartsink” patient revisited. Br J Gen Pract. 1999;49:230- 233. Butler CC, Evans M. The “heartsink” patient revisited. Br J Gen Pract. 1999;49:230- 233. Elder N, Ricer R, Tobias B. How respected family physicians manage difficult. J Am Board Fam Med 2006;19:533– 541. Elder N, Ricer R, Tobias B. How respected family physicians manage difficult. J Am Board Fam Med 2006;19:533– 541. Feldman MD, Berkowitz SA. Role of behavioral medicine in primary care. Curr Opin Psychiatry. 2012;25:121-127. Feldman MD, Berkowitz SA. Role of behavioral medicine in primary care. Curr Opin Psychiatry. 2012;25:121-127 Kontos N, et al. Fighting the good fight: Responsibility and rationale in the confrontation of patients. Mayo Clin Proc. 2012;87(1):63-66. Kontos N, et al. Fighting the good fight: Responsibility and rationale in the confrontation of patients. Mayo Clin Proc. 2012;87(1):63-66. Fried TR, Bradley EH, O’Leary J. Prognosis communication in serious illness: Perceptions of older patients, caregivers, and clinicians. J Am Geriatr Soc. 2003;51:1398-1403. Fried TR, Bradley EH, O’Leary J. Prognosis communication in serious illness: Perceptions of older patients, caregivers, and clinicians. J Am Geriatr Soc. 2003;51:1398-1403. Groves JE. Taking care of the hateful patient. N Eng J Med 1978;298:883-887. Groves JE. Taking care of the hateful patient. N Eng J Med 1978;298:883-887. Haas LJ, Leiser JP, Magill MK, Sanyer ON. Management of the difficult patient. American Family Physician. 2005;72(10) Haas LJ, Leiser JP, Magill MK, Sanyer ON. Management of the difficult patient. American Family Physician. 2005;72(10) Jackson, JL, Kroenke K. Difficult Patient Encounters in the Ambulatory Clinic: Clinical Predictors and Outcomes Arch Intern Med. 1999;159(10):1069-1075. Jackson, JL, Kroenke K. Difficult Patient Encounters in the Ambulatory Clinic: Clinical Predictors and Outcomes Arch Intern Med. 1999;159(10):1069-1075 Mathers N, Jones N, Hannay D. Heartsink patients: A study of their general practitioners. Br J Gen Pract. 1995;45:293-296. Mathers N, Jones N, Hannay D. Heartsink patients: A study of their general practitioners. Br J Gen Pract. 1995;45:293-296 O’Dowd TC. Five years of heartsink patients in general practice. BMJ 1988;297:528-530. O’Dowd TC. Five years of heartsink patients in general practice. BMJ 1988;297:528-530. Strous RD, Ulman AM, Kotler M. The hateful patient revisited: Relevance for 21st century medicine. European Journal of Internal Medicine. 2006 (17)6;387-393. Strous RD, Ulman AM, Kotler M. The hateful patient revisited: Relevance for 21st century medicine. European Journal of Internal Medicine. 2006 (17)6;387-393.
: Kontos N, et al. Fighting the good fight: Responsibility and rationale in the confrontation of patients. Mayo Clin Proc. 2012;87(1): Fried TR, Bradley EH, O’Leary J. Prognosis communication in serious illness: Perceptions of older patients, caregivers, and clinicians. J Am Geriatr Soc. 2003;51: Fried TR, Bradley EH, O’Leary J. Prognosis communication in serious illness: Perceptions of older patients, caregivers, and clinicians. J Am Geriatr Soc. 2003;51: Groves JE. Taking care of the hateful patient. N Eng J Med 1978;298: Groves JE. Taking care of the hateful patient. N Eng J Med 1978;298: Haas LJ, Leiser JP, Magill MK, Sanyer ON. Management of the difficult patient. American Family Physician. 2005;72(10) Haas LJ, Leiser JP, Magill MK, Sanyer ON. Management of the difficult patient. American Family Physician. 2005;72(10) Jackson, JL, Kroenke K. Difficult Patient Encounters in the Ambulatory Clinic: Clinical Predictors and Outcomes Arch Intern Med. 1999;159(10): Jackson, JL, Kroenke K. Difficult Patient Encounters in the Ambulatory Clinic: Clinical Predictors and Outcomes Arch Intern Med. 1999;159(10): Mathers N, Jones N, Hannay D. Heartsink patients: A study of their general practitioners. Br J Gen Pract. 1995;45: Mathers N, Jones N, Hannay D. Heartsink patients: A study of their general practitioners. Br J Gen Pract. 1995;45: O’Dowd TC. Five years of heartsink patients in general practice. BMJ 1988;297: O’Dowd TC. Five years of heartsink patients in general practice. BMJ 1988;297: Strous RD, Ulman AM, Kotler M. The hateful patient revisited: Relevance for 21st century medicine. European Journal of Internal Medicine (17)6; Strous RD, Ulman AM, Kotler M. The hateful patient revisited: Relevance for 21st century medicine. European Journal of Internal Medicine (17)6;")
Similar presentations






>")












