Download presentation
Presentation is loading. Please wait.

1
Fundamentals of Healthcare Reform Walter Coleman WV/PA HFMA September 25, 2014

4
How about efficiency?

5
Waste in the System

6
Industry Tipping Point 6 Revenue Time How do local market conditions impact timing considerations? Can market-changing events create an urgent paradigm shift? What is my step-change business model risk? Do I have the financial tools to adequately analyze relevant states?

7
Healthcare Performance Program Umbrella Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Bundled Payment Hospital Inpatient Quality Reporting Program ACO Medicare Shared Savings Program

9
VALUE BASED PURCHASING Mandatory Element of Reform

10
Value Based Purchasing Overview MANDATORY – we have no choice

11
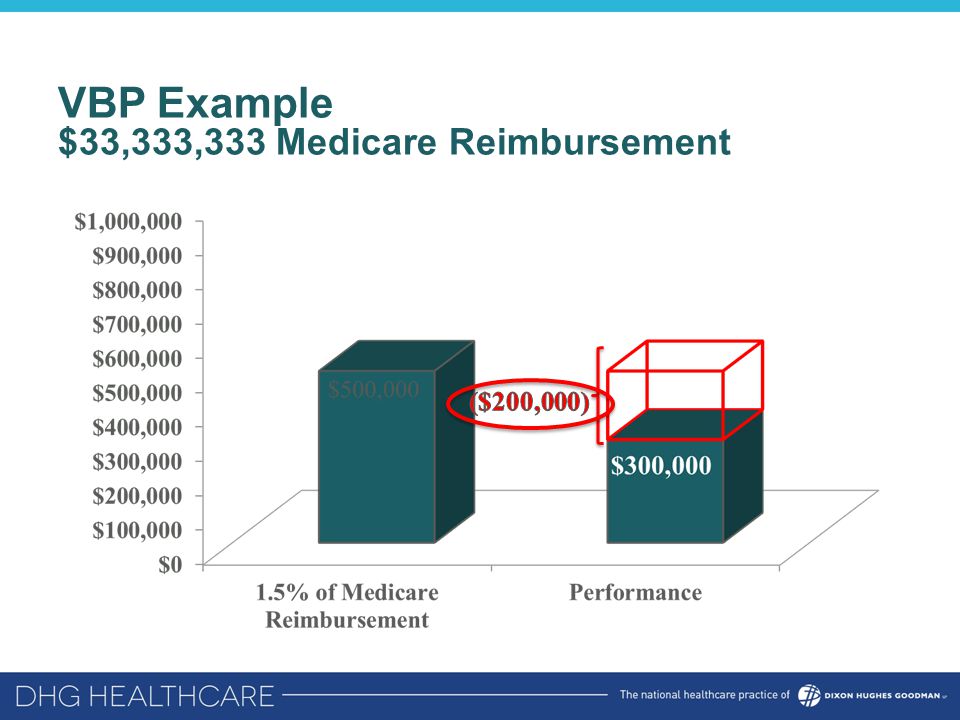
VBP Example $33,333,333 Medicare Reimbursement Amount mandated to pay for participation

12
VBP Example $33,333,333 Medicare Reimbursement

14
Amount mandated to pay for participation

15
VBP Example $33,333,333 Medicare Reimbursement

17
Value Based Purchasing Outcomes = Income Mandatory Pay for Performance Program –3,500 hospitals are included in this program across the country Reimbursement Determine Two Ways: –Achievement How we compare to National Top Decile (350 Hospitals) –Improvement How we measure against ourselves Did we do better than a previously measured baseline period
 –Improvement How we measure against ourselves Did we do better than a previously measured baseline period")
18
Value Based Purchasing Percent of Medicare Reimbursement at Risk FY 2013 – 1.00% FY 2014 – 1.25% FY 2015 – 1.50% FY 2016 – 1.75% FY 2017 – 2.00% FY 2018 – 2.00% FY 2019 – 2.00% FY 20xx – refers to the Federal Fiscal Year (Oct. 1 – Sep. 30) when DRG payments will be affected
 when DRG payments will be affected.")
19
NEW MEASURES Value Based Purchasing

20
VBP FY 2016 – New Measures Patient Experience –No Change – Same HCAHPS Measures Core Measures –5 Dropped; 1 New Outcomes –3 New Measures Efficiency –No Change

21
VBP FY 2016 – New Measures Patient Experience –No Change – Same HCAHPS Measures Core Measures –5 Dropped; 1 New Outcomes –3 New Measures Efficiency –No Change

22
VBP – FY 2016 – Patient Experience HCAHPS –Hospital Consumer Assessment of Healthcare Providers Survey –An engagement survey CMS has mandated each hospital give to every discharged inpatient –Consists of 27 questions that lead to the 8 categories assessed for VBP –Patients score each question on scale of 4 –For answers to count, patients must give hospitals a score of 4 or “Always”

23
VBP FY 2016 – Patient Experience Communication with Nurses Communication with Doctors Responsiveness of Hospital Staff Pain Management Communication about Medicines Cleanliness and Quietness of Hospital Discharge Information Overall Rating of Hospital

24
VBP FY 2016 – New Measures Patient Experience –No Change – Same HCAHPS Measures Core Measures –5 Dropped; 1 New Outcomes –3 New Measures Efficiency –No Change

25
VBP FY 2015 – Core Measures AMI-7a AMI-8a HF-1 PN-3b PN-6 SCIP-Inf-1 SCIP-Inf-2 SCIP-Inf-3 SCIP-Inf-4 SCIP-Inf-9 SCIP-Card-2 SCIP-VTE-2

26
VBP FY 2016 – Core Measures AMI-7a PN-6 SCIP-Inf-2 SCIP-Inf-3 SCIP-Inf-9 SCIP-Card-2 SCIP-VTE-2 IMM-2 Note: IMM-2 Performance Period is only 6 MONTHS (Two 3 Month Periods) January 1, 2014 – March 31, 2014 AND October 1, 2014 – December 31, 2014
 January 1, 2014 – March 31, 2014 AND October 1, 2014 – December 31, 2014")
27
VBP FY 2016 – Core Measures Measure IDBenchmark AMI-7a100% IMM-298.875% PN-6100% SCIP-Inf-2100% SCIP-Inf-3100% SCIP-Inf-9100% SCIP-Card-2100% SCIP-VTE-2100%

28
VBP FY 2016 – Core Measures AMI-7a PN-6 SCIP-Inf-2 SCIP-Inf-3 SCIP-Inf-9 SCIP-Card-2 SCIP-VTE-2 IMM-2

29
VBP FY 2017 – Clinical Care: Process AMI-7a IMM-2 PC-01 PC-01 = Elective Delivery Prior to 39 Completed Weeks Gestation

30
VBP FY 2016 – New Measures Patient Experience –No Change – Same HCAHPS Measures Core Measures –5 Dropped; 1 New Outcomes –3 New Measures Efficiency –No Change

31
VBP FY 2015 – Outcomes 30 Day Mortality – AMI 30 Day Mortality – HF 30 Day Mortality – PN AHRQ – PSI-90 CLABSI

32
VBP FY 2016 – Outcomes 30 Day Mortality – AMI 30 Day Mortality – HF 30 Day Mortality – PN AHRQ – PSI-90 CLABSI CAUTI SSI – Colon SSI – Abdominal Hysterectomy

33
VBP FY 2016 – Outcomes Measure IDBenchmark CAUTI0.000 CLABSI0.000 Surgical Site Infection Colon0.000 Abdominal Hysterectomy 0.000

34
VBP FY 2016 – Outcomes Outcomes 30 Day Mortality – AMI 30 Day Mortality – HF 30 Day Mortality – PN AHRQ – PSI-90 CLABSI CAUTI SSI-Colon SSI-Abdominal Hyster.

35
VBP FY 2017 – Clinical Care and Safety Clinical Care- Outcomes 30 Day Mortality – AMI 30 Day Mortality – HF 30 Day Mortality – PN AHRQ – PSI-90 CLABSI CAUTI SSI-Colon SSI-Abdominal Hyster. Safety MRSA C. Diff

37
Outcomes – 30 Day Mortality Currently in 3 Performance Periods FY 2016 ended June 30, 2014 FY 2019 began July 1, 2014 30 Day Mortality Measures –Assess deaths: AMI, HF, and PN that occur within 30 days after admission; which, depending on the length of stay, may occur post- discharge….

38
CMS 30 Day Risk-Standardized Mortality Rate Calculation Facility Predicted Deaths Facility Expected Deaths X Measure (AMI, HF, PN) National Crude Rate =
 National Crude Rate =")
39
VBP FY 2016 – New Measures Patient Experience –No Change – Same HCAHPS Measures Core Measures –5 Dropped; 1 New Outcomes –3 New Measures Efficiency –No Change

40
VBP FY 2016 - Efficiency Medicare Spend Per Beneficiary (MSPB) –Captures total Medicare Spending Per Beneficiary relative to a hospital stay, bundling hospital sources (Part A) with post acute care (Part B) –Bundles the cost of care delivered to a beneficiary for an episode across the continuum of care: 3 Days Prior Hospital Inpatient Stay 30 Days post Discharge
 –Captures total Medicare Spending Per Beneficiary relative to a hospital stay, bundling hospital sources (Part A) with post acute care (Part B) –Bundles the cost of care delivered to a beneficiary for an episode across the continuum of care: 3 Days Prior Hospital Inpatient Stay 30 Days post Discharge")
41
PROPOSED MSPB Measures Additional Efficiency Measures proposed to be added Risk Adjusted similarly to MSPB Proposed to facilitate alignment with the Physician Value Based Payment Modifier program Includes Part A and B and 3 days prior to admission and 30 days post discharge 41 MedicalSurgical Kidney/Urinary Tract Infection Hip replacement/revision CellulitisKnee replacement/revision Gastrointestinal hemorrhage Lumbar spine fusion/refusion SOURCE: May 1, 2014 Federal Register

42
VBP Shifting of Domain Weights FY 2013FY 2014FY 2015FY 2016 Core Measures Patient ExperienceEfficiency (MSPB) Outcomes
 Outcomes")
43
VBP – FY13 Domain Weights Performance Period: July 1, 2011 – March 31, 2012 Reimbursement Period: October 1, 2012 – September 30, 2013 Core Measures = 70%

44
VBP – FY14 Domain Weights Performance Period: April 1, 2012 – December 31, 2012 Reimbursement Period: October 1, 2013 – September 30, 2014 Core Measures = 45%Outcomes = 25%

45
VBP – FY15 Domain Weights Performance Period: January 1, 2013 – December 31, 2013 Reimbursement Period: October 1, 2014 – September 30, 2015 HCAHPS = 30% Outcomes = 30% MSPB = 20% One Measure!! Core Measures = 20%

46
VBP – FY16 Domain Weights Performance Period: January 1, 2014 – December 31, 2014 Reimbursement Period: October 1, 2015 – September 30, 2016 HCAHPS = 25% Outcomes = 40% MSPB = 25% Core Measures = 10%

47
47 HCAHPS = 25% Safety = 20% MSPB = 25% Clinical Care - Process = 5% Clinical Care - Outcomes = 25% VBP – FY17 Domain Weights Performance Period: January 1, 2015 – December 31, 2015 Reimbursement Period: October 1, 2016 – September 30, 2017

48
Crosswalk from FY 16 to FY 17 MeasurePrior Domain (FY’16)NQS Domain (FY’17) Core MeasuresClinical Process of CareClinical Care- Process HCAHPSPatient Experience of CarePatient & Caregiver Centered Experience of Care/Care Coordination CAUTI/CLABSI/SSIOutcomesSafety Mortality – 3 diagnosesOutcomesClinical Care- Outcomes PSI- 90OutcomesSafety Medicare Spend Per BeneficiaryEfficiencyEfficiency & Cost Reduction
NQS Domain (FY’17) Core MeasuresClinical Process of CareClinical Care- Process HCAHPSPatient Experience of CarePatient & Caregiver Centered Experience of Care/Care Coordination CAUTI/CLABSI/SSIOutcomesSafety Mortality – 3 diagnosesOutcomesClinical Care- Outcomes PSI- 90OutcomesSafety Medicare Spend Per BeneficiaryEfficiencyEfficiency & Cost Reduction")
49
ANALYZING VALUE BASED PURCHASING PERFORMANCE Fundamentals of Healthcare Reform

50
System was penalized $376,003 in FY’15 VBP Program Must acknowledge the amount UNEARNED Of the programs dollars made available: –System did not capitalize on $6,187,541

53
READMISSION REDUCTION PROGRAM Mandatory Element of Reform

55
Readmission Reduction Program 9% of Current and Future Medicare Reimbursement at Risk –3% penalty of Medicare Reimbursement at risk each program year –Measured Populations 30 days from DISCHARGE AMI, HF, PN, COPD, THA & TKA August 2014: CABG Added to FY 2017 Performance Periods: 3 Year Rolling Program –FY’15: July 1, 2010 – June 30, 2013 – 3% –FY’16: July 1, 2011 – June 30, 2014 – 3% –FY’17: July 1, 2012 – June 30, 2015 – 3% –FY’18: July 1, 2013 – June 30, 2016 – 3% –FY’19: July 1, 2014 – June 30, 2017 – 3% Currently participating in 3 performance periods simultaneously

56
How are Readmissions Measured? Scoring Index based at 1.0 Calculate Excess Readmission Ratio Excess Readmission Ratio > 1 = BAD Excess Readmission Ratio < 1 = GOOD Facility Predicted Value Facility Expected Value

57
HOSPITAL ACQUIRED CONDITIONS Mandatory Element of Reform

58
Hospital Acquired Conditions (1% at Risk*) 12 Hospital Acquired Conditions Identified –Divided in to 2 Domains If a hospital is in the BOTTOM QUARTILE (worst performing 25% in the country), it will be penalized a FULL 1% of Medicare Reimbursement Penalties will begin FY’15 (beginning October 1, 2014) *1% After DSH, Uncompensated Care, and IME
 12 Hospital Acquired Conditions Identified –Divided in to 2 Domains If a hospital is in the BOTTOM QUARTILE (worst performing 25% in the country), it will be penalized a FULL 1% of Medicare Reimbursement Penalties will begin FY’15 (beginning October 1, 2014) *1% After DSH, Uncompensated Care, and IME")
59
Hospital Acquired Conditions: FY 2015 First Domain: PSIs Performance Period: 7/1/11-6/30/13 Second Domain: CDC Performance Period: CY 2012 & 2013 Pressure Ulcer RateCLABSI Iatrogenic Pneumothorax RateCAUTI Central Venous Catheter-Related Bloodstream Infections Postoperative Hip Fracture Postoperative Pulmonary Embolism and Deep Vein Thrombosis Rate Postoperative Sepsis Postoperative Wound Dehiscence

60
HAC Domain Weightings: FY’15 DOMAIN 1: 35% DOMAIN 2: 65%

61
Hospital Acquired Conditions: FY 2016 First Domain: PSIs 25% Second Domain: CDC 75% Pressure Ulcer RateCLABSI Iatrogenic Pneumothorax RateCAUTI Central Venous Catheter-Related Bloodstream Infections SSI Following Colon Surgery (FY 2016) Postoperative Hip FractureSSI Following Abdominal Hysterectomy (FY 2016) Postoperative Pulmonary Embolism and Deep Vein Thrombosis Rate Postoperative Sepsis Postoperative Wound Dehiscence
 Postoperative Hip FractureSSI Following Abdominal Hysterectomy (FY 2016) Postoperative Pulmonary Embolism and Deep Vein Thrombosis Rate Postoperative Sepsis Postoperative Wound Dehiscence")
62
HAC Domain Weightings: FY’15 DOMAIN 1: 25% DOMAIN 2: 75%

63
Hospital Acquired Conditions: FY 2017 First Domain: PSIs 25% Second Domain: CDC 75% Pressure Ulcer RateCLABSI Iatrogenic Pneumothorax RateCAUTI Central Venous Catheter-Related Bloodstream Infections SSI Following Colon Surgery (FY 2016) Postoperative Hip FractureSSI Following Abdominal Hysterectomy (FY 2016) Postoperative Pulmonary Embolism and Deep Vein Thrombosis Rate Methicillin-Resistant Staphylococcus Aureus (MRSA) Bacteremia (FY 2017) Postoperative SepsisClostridium Difficile (FY 2017) Postoperative Wound Dehiscence
 Postoperative Hip FractureSSI Following Abdominal Hysterectomy (FY 2016) Postoperative Pulmonary Embolism and Deep Vein Thrombosis Rate Methicillin-Resistant Staphylococcus Aureus (MRSA) Bacteremia (FY 2017) Postoperative SepsisClostridium Difficile (FY 2017) Postoperative Wound Dehiscence")
64
Duplicate Measures 64

65
Penalties & Your DRG Payment

66
CURRENT DOLLARS AT RISK SAMPLE $50,000,000 FACILITY Mandatory Elements of Reform

67
VBP FY 2016 – Sample Current $$ at Risk

68
VBP – Sample Total Current $$ at Risk

69
All Reform – Sample Total Current $$ at Risk

70
OPPORTUNITIES Mandatory Elements of Reform

71
New NQS Based Domains for FY 2017 71 HCAHPS = 25% Safety = 20% MSPB = 25% Clinical Care - Process = 5% Clinical Care - Outcomes = 25%

72
50% of VBP is Mortality and MSPB 72 Clinical Care - Outcomes = 25%

73
Opportunities – VBP: Outcomes 73 Top 50 th = Δ1 Patient Top 10 th = Δ3 Patient Top 50 th = Δ1 PatientTop 50 th = Δ8 Patients Top 10 th = Δ11 PatientsTop 10 th = Δ3 Patient

74
VBP – CMS Proposed Future Measures FY 2018 Program (Performance Period: CY 2016) –Patient Experience: Care Transition FY 2019 Program (Performance Period: CY 2017) –Surgical Complication: Total Hip and Total Knee Arthroplasty
 –Patient Experience: Care Transition FY 2019 Program (Performance Period: CY 2017) –Surgical Complication: Total Hip and Total Knee Arthroplasty")
75
VBP – Other Possible Metrics to Follow Emergency Department Care Preventative Care –Pneumonia Vaccine Children’s Asthma Care Stroke Care –Blood Clot Prevention Care –Preventative Care

76
FY 19 New Measure Added THA/TKA for 30 month performance period. –January 1, 2015-June 30, 2017 –Baseline of July 1, 2010-June 30, 2013 Risk standardized measure for complications after Total Hips and Knees surgeries for up to 90 days post surgery –One of eight complications: AMI, pneumonia, sepsis, SSI, PE, death, mechanical complication or periprosthetic joint infection/wound infection. –Each has a defined time frame –Each is a ‘Yes’ or ‘No –Risk adjusted for patient age, sex and comorbidities 76 SOURCE: August 2014 Proposed Rules Federal Register

77
Readmissions – Proposed Future Measures Percutaneous Coronary Intervention (PCI) Stroke
 Stroke")
78
Opportunities – HAC SSI Following Colon Surgery (FY’16) SSI Following Abdominal Hysterectomy (FY’16) MRSA (FY’17) C Diff (FY’17)
 SSI Following Abdominal Hysterectomy (FY’16) MRSA (FY’17) C Diff (FY’17)")
79
BPCI BUNDLED PAYMENTS

80
Description of Models 1 - 4 80

81
Medical Homes Acute Care Bundling Acute Care Episode with Post Acute Care Bundling Post Acute Care Bundling ©2010 Kaufman Hall & American Hospital Association. 81 Bundled Payments

82
Advantages of Participation Improved quality of care for patients –Reduced complications, readmissions, and cost Improved ability to work with hospitals, physicians, nursing homes, home health, rehab centers, and other providers to improve overall care quality and service Potential competitive advantage within market with physicians and post-acute care Opportunity to receive payment aligned with these goals and based on outcomes 82

83
http://innovation.cms.gov/initiatives/bundled-payments/ 83 MEDICARE: Cohort 1 COMMERCIAL as of July 2014 Where are the Bundled Payments?

84
Early Results of BPCI Cohort 2 Tremendous increase in the number of applications in the most recent open enrollment in April 2014: Nearly Triple! Models 2,3,4 were open for enrollment Currently in the Phase 1 period which is the non risk, decision making period. Phase 2 is when the Episode Initiator starts to accept risk

85
Changes In the Cohort 2 Timeline: 7/31/14 EventOriginal DateRevised Date Historical Claims & Target Pricing Late Summer 2014October 2014 Go/No Go Decision to Participate November 1, 2014January 1, 2015 Go Live with RiskJanuary 1, 2015April 1, 2015 Other significant changes: ADDITION OF EPISODES: You can now add episodes in July 2015 and October 2015: only 1 episode is required for April 1, 2015. Phase 1 ends in October 2015 B-CARE: B-CARE quality data wont be collected until Spring 2015 Option for Delayed Reconciliation: Will offer a 4 quarter timeline for reconciliation.

86
MD Home Health SNF IRF Outpt. Rehab Readmission Home $3,207$10,129$8,965$616 + + + = $22,927 x98% $22,468 DRG Inpatient and PACS Fee for Service Model $22,468 Bundled Episodic Model DRG 470 Total Joint Replacement w/out CC Model 2 Note: any CMI aggregate charges lower than $22,468 can be shared with providers via gain sharing model Episodic period for model 2: 3 days prior to admission to 90 days post discharge from hospital

87
BPCI Multiple Bonus Payments: Physicians 2 opportunities for Physicians to be awarded Bonuses 1.Internal Cost Savings Pool 2.Bundled Payment Savings Pool Both have required Quality Metrics and Cost Savings to be met Cost Savings MUST be directly attributed to Quality Improvement and Care Redesign 87

88
BPCI Multiple Bonus Payments: Physicians 2 opportunities for Physicians to be awarded Bonuses 1.Internal Cost Savings Pool 2.Bundled Payment Savings Pool Both have required Quality Metrics and Cost Savings to be met Cost Savings MUST be directly attributed to Quality Improvement and Care Redesign 88

89
Internal Cost Savings DHG Healthcare has one of very few, if not the only, Internal Cost Savings Gainshare models to have been submitted and approved by CMS at this time APPROVEDAPPROVED

90
In February 2014, CMMI issued a Request for Information on a new bundled payment program to expand to outpatient. Focus is Specialty Physicians and on (1)Procedures and (2) complex chronic care Highlighted colonoscopy, cataract surgery, & radiation therapy for procedural options. Regarding the chronic care, “CMS is considering development of a model that would incentivize specialists to more efficiently manage the care provided to beneficiaries with complex or chronic medical conditions over the period of time that corresponds to the specialty practitioner’s long term involvement with managing the beneficiary’s care.” Was seeking responses until March 13 Outpatient Bundling…coming soon?
Procedures and (2) complex chronic care Highlighted colonoscopy, cataract surgery, & radiation therapy for procedural options. Regarding the chronic care, CMS is considering development of a model that would incentivize specialists to more efficiently manage the care provided to beneficiaries with complex or chronic medical conditions over the period of time that corresponds to the specialty practitioner’s long term involvement with managing the beneficiary’s care. Was seeking responses until March 13 Outpatient Bundling…coming soon .")
91
Outpatient Bundling Referred to by CMS as: “Comprehensive Ambulatory Payment Classification (APC)” Finalized in the CY 2014 OPPS/ASC Final Rule Affect payments to 4,000 hospitals and 5,300 ASC’s Delayed implementation to January 1, 2015 instead of the traditional outpatient October 1 implementation date –Extra time allowed the Agency, hospitals, and physicians more time to evaluate and comment on the policy
 Finalized in the CY 2014 OPPS/ASC Final Rule Affect payments to 4,000 hospitals and 5,300 ASC’s Delayed implementation to January 1, 2015 instead of the traditional outpatient October 1 implementation date –Extra time allowed the Agency, hospitals, and physicians more time to evaluate and comment on the policy")
92
Outpatient Bundling – Comprehensive APC’s Single Medicare payment rather than individual APC payments throughout the episode 28 Bundled Outpatient Procedures Proposed Payment could include all hospital services reported on the claim covered under Medicare Part B for up to a proposed 6 Month Period –Few exceptions resulting in a single beneficiary copayment per claim

93
Outpatient Bundling – Proposed Procedures

94
Outpatient Bundling – Summary Comprehensive APC is another step towards CMS establishing a Prospective Payment Model for OPPS Goal: eliminate avoidable costs and increase shared decision making Healthcare stakeholders who have been on the sidelines for recent CMS pilots and existing programs will not have this luxury as CMS expands their delivery and payment reform portfolio in the upcoming calendar year

95
Thank you! Contact Information: Walter Coleman Walter.Coleman@dhgllp.com (804) 474-1248
")
Similar presentations







 Experience of Care Surveys From Design to Implementation>")






 Agency for Healthcare Research and Quality Centers for Medicare and Medicaid Services.>")










