Download presentation
Presentation is loading. Please wait.

2
Two major areas to cover in the next two weeks: Pandemics Contagion in a very real sense. Threats to global health. Global Health indicators The Double Burden. How are we doing? Throughout, to make the connections to globalization processes.

3
Diseases, communicable or non-communicable, are relatively predictable in their patterns across regions and time. Their ‘burden’ can be estimated and incorporated into development goals. But what about epidemics and pandemics, which are: Chaotic in time and space. Respect no boundaries. Burden is shared: like climate change it is unequally and inequitably distributed - caused by some, felt by all. Epidemics and Pandemics

4
Epidemics are considered to be outbreaks of a disease that far exceed the normal ‘base-line incidence rate’ of that disease. They can be of communicable (infectious) or non- communicable (not infectious). They are usually confined within a larger region or nation. Pandemics are all of the above, but the term is usually reserved for infectious diseases that cross national boundaries. In this sense they a phenomenon of globalization. Epidemics Versus Pandemics
 or non- communicable (not infectious). They are usually confined within a larger region or nation. Pandemics are all of the above, but the term is usually reserved for infectious diseases that cross national boundaries. In this sense they a phenomenon of globalization. Epidemics Versus Pandemics.")
5
Epidemics and Income No correlation between wealth and deaths from epidemics Source: Gapminder

6
Pandemics

7
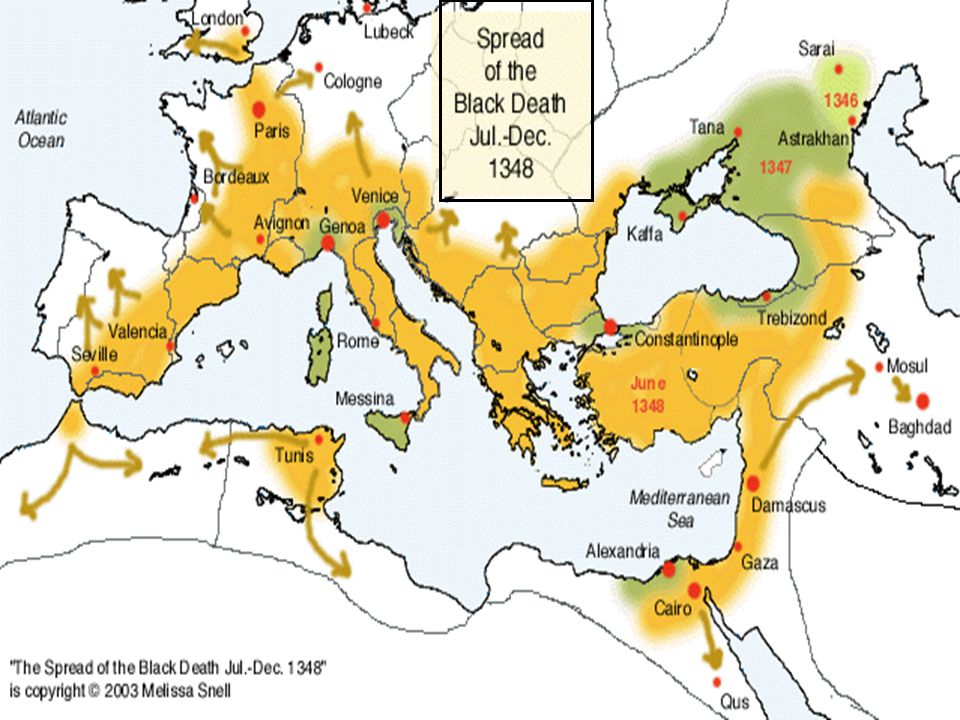
1320s? 1338 1340 1349 1346 Tibetan Plateau & The Himalaya Indochina Rivers: Mekong, Chang Origins of Spread of the Black Death in Asia, 1320s-1350

8
1320s? 1338 1340s? 1349 1346 Tibetan Plateau & The Himalaya Indochina Rivers: Mekong, Chang Spread of the Black Death in Asia, 1320s-1350 Baghdad Hsian Hangzhou Beijing Mecca Saral Samarkand

9
Kaffa

11
Yersinia pestis Bubonic plague bacilli Rattus rattus Black rat Xenopsylla cheopis Oriental flea

12
Debate About The Great Plague Some researchers believe the Great Plague was either a viral hemorrhagic fever or bacillus based anthrax and not caused by Yersinia pestis. But excavation of a plague pit in London, England in 2011 demonstrated that it was Yersinia pestis. The plague is actually three diseases: Bubonic or lymph system infection Mortality: 1-15% with treatment, 70-80% without Septicemia or blood infection Mortality: 40-60% with treatment, 100% without Pneumonic or lung infection Mortality: 100%

13
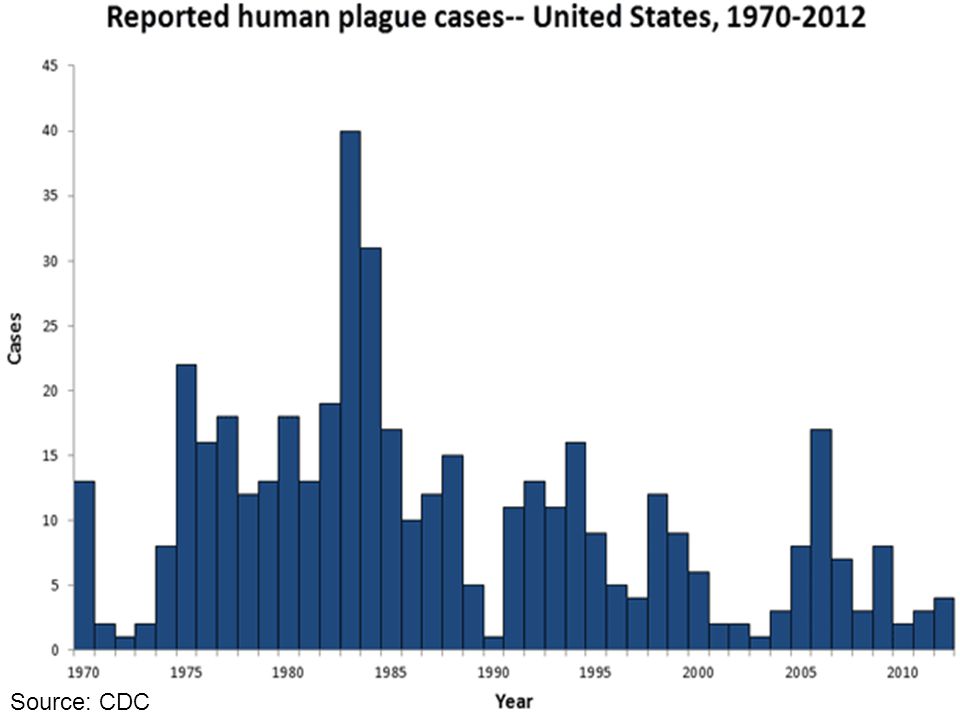
Nursery Rhymes Ring around the rosy A pocketful of posies "Ashes, Ashes" We all fall down! This delightful nursery rhyme came into being around 1665 with the Black Death hit London, England, and it details symptoms, ‘treatment’, and outcomes of the disease. There are still about 1,000 to 3,000 cases each year around the world, and since 1990 there have been 134 cases reported in the U.S., 65 of them in New Mexico. Chance of dying from plague today is about 1 in 30 million. In the 14 th century it was 1 in 2.

14
Source: CDC

16
CDC

17
The 1918 Flu Pandemic Camp Funston, Fort Riley, Kansas Killed 40 million in just 24 weeks Killed over 100 million in two years Killed mostly 15-35 year old cohort “They were doubly dead in that they died so young.” Dr. Harvey Cushing, prominent surgeon of the day. An estimated 8-10% of the cohort died

18
Started at Camp Funston, February 1918 By March 1,100 sick, 237 pneumonia, 37 died Starting June 1918 troops ship out to Europe Hundreds of troops transfer between hundreds of camps Sept to November 1918 the peak deaths period Pandemic lasted for three years 1918, 1919, 1920 In those 12 weeks over 20 million died Over that period 60 to 100 million died

19
Week of Sept 28, 1918 Week of Dec 14, 1918 Deaths Per Thousand

20
Age Specific Death Rates Per 100,000 Before and During the Pandemic Crude death rates in US before and after 1918 pandemic Year191219131914191519161917191819191920192119221923 Rate10.012.38.915.727.017.4301.899.070.511.331.044.1 Average crude death rate before and after 1918 = 21 Average crude death during the flu years = 157

21
Death Rates Per 100,000 Before and During the Pandemic Crude death rates per 1000 in US before and after 1918 pandemic Year191219131914191519161917191819191920192119221923 Rate10.012.38.915.727.017.4301.899.070.511.331.044.1 Average crude death rate before and after 1918 = 21 Average crude death during the flu years = 157

22
Excess Mortality by Age and Gender Age cohort 14-40

23
Number of cases and number of deaths, Switzerland

24
U.S. Life Expectancy 1900 to 1960

26
“The following 72 Inupiat Eskimos are interred in this common grave. Pray, honor and remember these villagers who lost their lives in the short span of five days in the influenza pandemic November 15-20 1918.”

27
In 1997, 71 year old retired pathologist Johan Hultin travels to Alaska and retrieves the lungs of an Inuit victim of the 1918 pandemic. He sends the samples to molecular biologist Jeffery Taubenberger. He discovers that the 1918 virus was a mutated bird virus. Taubenberger uses the lung tissue and tissue from army victims to reconstruct the 1918 virus.

28
The pathogen of 1918 was a virus of the genus Orthomyxoviridae. The strain is called H1N1 and is a close relative to the current Avian Flu strain H5N1 - too close a kissing cousin to the virulent 1918 flu for comfort. Normal mortality rates for flu are about 0.5%. The fatality rate of the 1918 flu was between 2% & 20%. In some isolated communities it was 100%. The fatality rate of the recent Avian flu is about 35%. The concern is a new flu with the virulence of the 1918 flu and the mortality rate of the current Avian flu. And both came from birds. The 2009 pandemic was also H1N1 but did not show itself as virulent as the 1918 pandemic. Antibody tests of 40 people born before 1920 show that they are resistant to the 2009 H1N5 strain. That is very scary because it shows how genetically close H1N1 and H1N5 are.

30
Current Avian flu strain first surfaced in Britain in 1959. First human cases occurred in 1997. 18 infected, 6 die, fatality rate of 33%. In 2003 3 more cases and 2 deaths occur in Hong Kong, but disease does not appear to be human to human. Later that year big cats at a Thailand zoo became infected and died. In 2004 a major outbreak occurred among domestic fowl in China and Vietnam, spreading to other South Asian countries, spread through infected wild waterfowl.

31
January 2005, Vietnam kills 150 million chickens. April 2005 – mass die off of migratory waterfowl in Central China. By the end of 2005 mass die-offs in Central and southern Russia. During 2006-2007 mass die-offs of migratory wildfowl continued. Between 2003 and October 2007 there have been 331 cases and 203 deaths for a fatality rate on 63%. If and when H5N1 or even H1N1 strikes again, it will put 1918 in the shade.

33
→ Countries with poultry or wild birds killed by H5N1. → Countries with humans, poultry and wild birds killed by H5N1.

34
Longest Arctic Bird Migration Routes Most of the species that connect North America with Eurasia are not from those known to carry H5N1 or H1N1

35
Chart shows the number of cases and deaths from H5N1 between 2004 and 2007. The apparent slackening of the fatality rate is due to increasing number of cases. Cases Deaths

36
Mortality rate of H5N1 between 2005 and 2007 – thin line actual rate, thick line averaged rate

38
The next pandemic is thought to be from H7N9, which surfaced in 2013 with 100 cases. Morbidity rate is 77%, and mortality rate is 27% - that is 77 out of every 100 will catch it and 27 of them will die. Its only saving grace is that its virulence is low - it does not spread easily - yet. But neither does it make poultry ill so culling infected birds is not possible, but only shutting down poultry markets. Vaccination of poultry would only help the virus mutate, maybe making it more virulent. What’s Next?

39
Cholera

40
From first symptoms to death through hypotensive shock can be as short as 2-4 hours but more usually 4-16 hours. Families would wake up normal and be dead by evening. The pathogen is a bacterium called Vibrio cholera. Its natural hosts are humans and its vector is through human fecal contamination of the water supply. There have been at least 7 major pandemics in the last 200 years, the first of these starting in Bengal in 1816. About 10 million people died from the disease over this period. Endemic to the Indian sub continent, with its major reservoir being the Ganges River.

41
In 2010 470,000 cases of Cholera occurred in Haiti just after the earthquake, and caused over 6,600 deaths. Globally there are still 2-5 million cases each year, resulting in 100,000 to 200,000 deaths. Between 1991 and 1994 in South America, cholera infected over one million people and killing 10,000. Caused by a ballast discharge from an Indian cargo ship.

42
Early Epidemiology - Dr. John Snow’s Map of cholera deaths and the Broad Street Pump

44
Smallpox is a horrifying and deadly disease that had plagued humanity for thousands of years. It is also the villain of a success story – the only one that has resulted in the eradication of a disease. SMALLPOX ERADICATION – A GLOBAL SUCCESS STORY Caused by a pox family virus called Variola – v. major and v. minor. Both cause disease but v. major is deadly – 35% mortality. A vaccine for the disease was first discovered in 1796 by Edward Jenner who found that milkmaids with cowpox - a milder cousin - did not contract smallpox. By injected people with extracts from cowpox sores he thus prevented them from getting smallpox. Hence the term vaccine – from the latin word for cow – vacca. But it is what happened between 1958 and 1974 that is of interest.

45
SMALLPOX ERADICATION – A GLOBAL SUCCESS STORY Before 1958 smallpox infected 50 million people a year in over 30 countries, killed about 2 million, and left millions more with horrifying disfigurements. At the instigation of the Soviet Union, in 1958 the World Health Authority (later to become the WHO) commenced campaign to eradicate smallpox from the earth. What makes smallpox a disease that could be eradicated? 1.No sub-clinical infections (you caught it, you showed it). 2. No non-human reservoirs or vectors. 3. Victims infectious for only 5 days. 4. Effects severely debilitating limiting mobility. 5. Clearly recognizable symptoms. 6. Cheap, effective, easily transported vaccine available. 7. Once vaccinated, always protected. A campaign of (1) identify cases, (2) surround and buffer outbreak, (3) immunize everyone was started in 1967.
 commenced campaign to eradicate smallpox from the earth. What makes smallpox a disease that could be eradicated. 1.No sub-clinical infections (you caught it, you showed it). 2. No non-human reservoirs or vectors. 3. Victims infectious for only 5 days. 4. Effects severely debilitating limiting mobility. 5. Clearly recognizable symptoms. 6. Cheap, effective, easily transported vaccine available. 7. Once vaccinated, always protected. A campaign of (1) identify cases, (2) surround and buffer outbreak, (3) immunize everyone was started in")
46
SMALLPOX ERADICATION – A GLOBAL SUCCESS STORY While no naturally occurring smallpox virus is alive today, both the U.S. and Russia keep samples in case the other uses it as a weapon. It is reported that Russia currently has several tons of freeze dried genetically engineered hemorrhagic smallpox virus stored. In 1978 a photographer working at a government lab in England was accidentally infected and died – the last case to do so. On May 8 th 1980 the WHO declared the earth smallpox free. By 1975 the last case of v. major was cured in Bangladesh, and by 1977 the last case of v. minor was cured in Somalia. U.N. has voted several times to destroy these samples but the U.S. and Russia refuse. Genome has been sequenced so no reason to keep the actual virus around.

47
HIV Prevalence Rates 25 million dead since 1981 About 3.1 million deaths per year, of which 577,000 are children Sixty four percent of all people with AIDS live in Sub Saharan Africa Seventy-seven percent of all women with AIDS live in Sub Saharan Africa

48
Absolute Number of People Living With AIDS

49
Sub Saharan Africa

50
The Current Ebola Pandemic Ebola virus budding from dead cell

51
Ebola Overreaction? Ebola is a disease that has been in the news due to the recent pandemic in West Africa. Two things make this epidemic interesting to us: The direct effect of globalisation on its spread. The reaction of authorities and people to it. Because the Ebola epidemic is not one that should have elicited such a response.

52
Ebola Factoids No doubt that this is a scary pathogen: Ebola prevents clotting so when it buds from a cell the cell disintegrates and you bleed out internally, leaking from your orifices and other breaches in the dermis. Mortality Rate is very high - 40-90%. It is extremely infectious (as few as a single virion can infect you) but not very contagious (it’s hard to catch since its not airborne). It’s not very virulent (doesn’t spread easily) but is lethal (you likely will die and quickly).
 but not very contagious (it’s hard to catch since its not airborne). It’s not very virulent (doesn’t spread easily) but is lethal (you likely will die and quickly)..")
53
Ebola Factoids Reservoir is thought to be fruit bats (that remain asymptomatic), and it also effects other primates such as gorillas and especially chimps. Spread by direct contact with infected body fluids. Cultural actions such as corpse washing, kissing, touching spread the disease. Incubation about 8-10 days, symptoms in last 4-6 days of incubation period, death within 2-4 days of symptoms presenting. Corpses remain infectious for as long as there are cells to colonise, but recovered victims do not remain infectious.

54
Ebola History First came to light in 1976 in villages along the Ebola River in Zaire (formerly DR Congo). Several other outbreaks in Zaire, Sudan, Ivory Coast between 1976 and the 2014 outbreak, the most significant being one that was started by Belgian nuns at a medical mission who used infected needles. Outbreaks have been caused in most cases by the butchering of infected chimps as bush meat. Historically the disease is controlled by its lethality – it incapacitates and kills too quickly for it to spread. So what happened in 2014?

55
Ebola 2014 Globalisation happened. Population densities increased greatly, especially in cities. Free trade agreements opened cross border work options for people so they moved further, quicker. Speed of travel increased due to more and different modes and mediums of travel. Inadequate governance could not control the infection once it started to spread: inadequate health facilities and knowledge, corrupt and incompetent officials, poor communication.

56
Ebola 2014 Global Village echoed what was happening around the world, media show up, people see the disease and its victims, along with the poor response from their governments on their TVs and internet. Misinformation about the disease spreads through available channels such as TV, internet, cell phones, resulting in: Proper prevention information is ignored or lost in the noise. People shy away from what few (and later better) facilities exist. People hiding sick relatives because they think hospitals are killing them. Continue with cultural burial practices that spread the disease.
 facilities exist. People hiding sick relatives because they think hospitals are killing them. Continue with cultural burial practices that spread the disease..")
57
RECORDED EBOLA CASES, 1976-2014 (Source: CDC) DateCountry Number of human cases Number of deaths % Fatality Rate 2014Multiple Countries, incl. DR Congo 23,472 9,506 40.5% 2013Uganda 6 3 50.0% 2012DR Congo, Uganda 44 17 38.6% 2011Uganda 1 1 100.0% 2008Congo, Philippines, Uganda 187 52 27.8% 2007Uganda, DR Congo 413 224 54.2% 2004Russia, South Sudan 18 8 44.4% 2003DR Congo 178 157 88.2% 2002Gabon, DR Congo 122 96 78.7% 2001Uganda 425 224 52.7% 1996S. Africa, USA, Philippines, Russia, Gabon 10068 68.0% 1995DR Congo 31525079.4% 1994Gabon, Ivory Coast 5331 58.5% 1990Philippines, USA 7 - 0.0% 1979South Sudan 342264.7% 1977Zaire (now DR Congo) 11 100.0% 1976Sudan, Zaire (now DR Congo) 602431 71.6% Total Number of Ebola Cases: 25,978 Total Number of Deaths: 11,091 Fatality Rate: 42.7%
 % 1976Sudan, Zaire (now DR Congo) % Total Number of Ebola Cases: 25,978 Total Number of Deaths: 11,091 Fatality Rate: 42.7%.")
58
Current Ebola 2014-2015 Pandemic As of February 1, 2015: Guinea – 2,975 cases, 1,944 deaths Liberia – 8,745 cases, 3,746 deaths Mali - 8 cases, 6 deaths Nigeria - 20 cases, 8 deaths Senegal - 1 case, 0 deaths (infection originated in Guinea) Sierra Leone – 10,740 cases, 3,276 deaths DR Congo – 66 cases, 49 deaths Spain - 1 case, 0 deaths United Kingdom - 1 case, 0 deaths United States - 4 cases, 1 death (two infections originated in the United States, one in Liberia and one in Guinea) Source: World Health Organization and CDC.
 Sierra Leone – 10,740 cases, 3,276 deaths DR Congo – 66 cases, 49 deaths Spain - 1 case, 0 deaths United Kingdom - 1 case, 0 deaths United States - 4 cases, 1 death (two infections originated in the United States, one in Liberia and one in Guinea) Source: World Health Organization and CDC.")
59
Ebola Range

60
Malaria Range

61
Malaria: According to WHO data about 3.2 billion people – almost half of the world's population – are at risk of malaria. In 2013, there were about 198 million malaria cases and an estimated 584,000 malaria deaths. That’s about 7,622 times more cases, and 52 times more deaths than Ebola. World Bank Estimates of Ebola Pandemic Treating the Ebola pandemic so far: $518 million. Cost of recovery packages: $450 million. Loss to economies: $1.6 billion. Putting Things Into Perspective

62
Cost of Treating Malaria: $60 per case. $20,547 per death. Cost of Treating Ebola: $19,939 per case. $46,704 per death. Putting Things Into Perspective

63
And Lest We Forget – The Current Measles Epidemic This one is close to home and speaks to the complacency of the majority and the scientific ignorance and irresponsibility of the anti-vaccine group. The so called “anti-vaxxers” continue to spread discredited and unfounded rumours and misinformation that is dangerous to everyone and not just them. Let’s look at some of their claims.

64
The Current Measles Epidemic - Anti-vaxxer Claim #1 The vaccine (as do all) causes autism: This myth came from a completely discredited but published study by a UK ex-doctor called Wakefield who was later struck off the register for using fraudulent data, incompetent statistics and dangerous claims. The problem here is partly society’s. We don’t publish papers that don’t find anything. Its called negative results bias. Wakefield still wanders the world being paid by anti- vaxxers to talk about his “results” and is seen as a folk hero to some of them.

65
The Current Measles Epidemic - Anti-vaxxer Claim #2 Thimerosal causes autism: Thimerosal is a mecury containing preservative occasionally used in vaccines, and a crackpot organization known as Generation Rescue, which appears bent among other things on “saving” people from vaccinations, along with Robert F. Kennedy Jr. started rumours that it caused autism. There had been no studies either way to support of deny the claim, so they were done and found zero correlation between the thimerosal and autism. And the mercury? There’s more in a tuna fish sandwich – or an Advil.

66
The Current Measles Epidemic - Anti-vaxxer Claim #3 Cases have been decreasing long before vaccines. This is just wishful thinking on the part of anti-vaxxers. Yes the number of cases of just about every major infectious disease have been decreasing through better prophylactic care and public health knowledge. BUT: The population is not immune from these diseases. The fact that the number of cases decreases does not mean that the disease has gone – it hasn’t. There is no herd immunity – diseases still sits waiting for an outbreak. Lower is not the same as zero. Decreasing numbers of cases is not the same as zero cases. Some people, mostly kids, still die and the disease still lives in the host population.

67
The Current Measles Epidemic - Anti-vaxxer Claim #4 Your own immune system is good enough. Well, would that it was but if it were we wouldn’t need vaccines to start with. Your immune system will not protect you against measles, which is just about the most contagious disease in the world, or any other infectious disease. Walk into a doctor’s waiting room two hours after an infected person had been in there and there is a high probability you will catch the disease. If you are vaccinated, you are safe unless: You are in chemotherapy. You are pregnant. You have an otherwise compromised immune system.

68
The Current Measles Epidemic - Anti-vaxxer Claim #5 Everyone else is vaccinated so what’s the problem. Apart from the selfishness of this claim, it’s ill-informed nonsense. This refers to “herd immunity” which theorizes that if enough people in a population (the herd) are protected, then the disease cannot easily spread. But measles, like any disease, continues to exist because of wild reservoirs of the pathogen – in the case of measles the wild reservoir being unvaccinated people. But measles is so contagious it requires a “herd” approaching 98% of a population, so even a few unvaccinated people form a viable reservoir. As well, you are only protected by herd immunity as long as you stay in the herd. Visit anywhere without herd immunity (such as most of the world) and you can catch the disease.
 are protected, then the disease cannot easily spread. But measles, like any disease, continues to exist because of wild reservoirs of the pathogen – in the case of measles the wild reservoir being unvaccinated people. But measles is so contagious it requires a herd approaching 98% of a population, so even a few unvaccinated people form a viable reservoir. As well, you are only protected by herd immunity as long as you stay in the herd. Visit anywhere without herd immunity (such as most of the world) and you can catch the disease..")
70
The Current Measles Epidemic – The Real Danger Measles is not a harmless disease, but it is not the crippling killers than tuberculosis, polio, diphtheria, rubella, whooping cough, mumps, chickenpox, etc, are. Together these diseases accounted for most of the very high infant mortality rates in pre-vaccination days. More disturbing, antibiotics are getting fewer and less effective, and anti-virals are few and far between or non-existent, so if people do get these diseases, they will have virtually no effective drug interventions. That is why we invented vaccines – the single most effective way to prevent illness and death.

71
Vaccination begins 1963

72
Widespread vaccination begins late 1940s. Pertussis (Whooping Cough) Death Rates 1900-1966
 Death Rates")
73
Diphtheria Death Rates 1900-1966 Vaccination begins 1920.

74
Controlling Death Measles Mortality Rate in the United States 1900-1990 Vaccination begins in 1963, virtually eliminating disease. Lower rates stabilize 1942- 1964 but still happen due to extant disease. Rapidly declining rates 1925- 1942 with better prophylactic care. But the disease is still extant are people still die. Stable high mortality 1900-1925. DEMOGRAPHIC Transition Source: CDC.

75
In the 2000s a backlash against immunization (decrease in vaccination rates), caused a recurrence of and increase in measles until increasing vaccination rates reduced the incidence rates again. Vaccination rate Incidence rate Controlling Death – An Ongoing Battle Measles Incidence and Vaccination Rates, England & Wales 18000 16000 14000 12000 10000 8000 6000 4000 2000 0 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 100% 95% 90% 85% 80% 75% DEMOGRAPHIC Transition

76
Pandemics and Globalisation Fact of life anywhere there is life. Natural control is infection burn-out. The higher the virulence, the faster the burn-out, the smaller the spread. Changes in the speed of transmission now threatens these controls, especially virulence. Resistance to drugs makes pandemics more likely. Eight major links to increased threat of pandemics and globalization…

77
Number of Syphilis Cases, U.S., 2005-2013 Use of online “hook-up” apps such as Tinder, Grindr has led to significant increase in syphilis cases and other STIs. Tinder has about 50 million users since 2012 and makes 15 million matches a day. About 40% of the increase in syphilis is attributed to hook-ups via these apps, and about 40% of the rest from a relaxing of attitudes towards safe sex due to perception that HIV/AIDS is no longer a death sentence. Source: New Scientists, 2015

78
Pandemics and Globalisation 1. Speed of transmission. 2. People’s propensity and means to travel. 3. Trade and volume has provided new vectors. 4. More wild ecosystems in contact with humans. 5. Climate change is increasing insect carrier vector range. 6. Industrial agriculture’s abuse of antibiotics. 7. Industrial agriculture’s abuse of chemical controls (DDT). 8. Environmental concerns limit effective controls (DDT). 9. Cultural memory forgets: because we have not experienced disease due to vaccination, we forget its awful consequences.
. 8. Environmental concerns limit effective controls (DDT). 9. Cultural memory forgets: because we have not experienced disease due to vaccination, we forget its awful consequences..")
79
Global Health Burden of Disease Pandemics Changing Demographics Aging Demographic transition Changing Economics Development Industrialisation Changing Territory Borders More countries Conflict Changing Geography Global village Transportation Communication Summary Changing Culture Changing Environment

80
Now don’t Forget. Wash your hands!

Similar presentations













. Viruses are made of genetic material (DNA or RNA) surrounded.>")












