Download presentation
Presentation is loading. Please wait.

1
PRESENTING INFORMATION PEOPLE UNDERSTAND AND USE Kathleen Cook, BSN Information & Fiscal Manager

2
CHALLENGE and STRATEGY

3
CHALLENGE Produce easy to understand and timely information Demands from public, decision-makers, political leaders, program staff and managers, funders and stakeholders, grantors Pressure to show evidence-based practice outcomes More data and data sources are available with little guidance for interpretation Limited resources and staff to do the work

4
GOAL

5
STRATEGY Principles to Guide Investments Support work at point of service Use standard, off-the-shelf technology Look for potential scalability Document for future Key Elements Systematic Replicable Easy to Use Meaningful Reliable, consistent and on- going sources of data Comparable Bench-marked Related to Department mission, goals, objectives Make the time to develop strategic guide for IT investments and development

6
Report Forms / Policies Planning Staff Stakeholders Decision makers Citizen portal Electronic medical / dental applications Permitting and inspection applications Financial system Personnel System Document management Network / database management City Enterprise Support Department— Daily Activities Web-based hub for technology services to staff DASHBOARD Health Department IT Strategy

7
MANAGING THE DATA PRACTICAL AND STRUCTURED APPROACH

8
TYPES OF DATA PRESENTATION Static Data Periodic updates BRFSS / YRBS Hospital Discharge Vital Statistics Dynamic and Calculated Data Near real time updates (Dynamic) Collection of data, organized and pre-calculated Point of service software (electronic medical/dental record; permit & inspection records) Syndromic surveillance Measures Benchmarks Performance indicators Population health indicators Process indicators Analytics Data / process mining Statistical / predictive analysis Reporting Visualization Graphs/charts Dashboards Alerts
 Collection of data, organized and pre-calculated Point of service software (electronic medical/dental record; permit & inspection records) Syndromic surveillance Measures Benchmarks Performance indicators Population health indicators Process indicators Analytics Data / process mining Statistical / predictive analysis Reporting Visualization Graphs/charts Dashboards Alerts")
9
Managing Static Data Standardize the process for each data source Create scripts and routines that can be run automatically Modify only when the data itself changes We are saving at least 500 hours of Epidemiology staff per data source Raw data Analysis and Weighting – Survey data must be weighted based on sample size and demographics – Event data (e.g. births, deaths) must be adjusted when used for rates—particularly if cell size is less than 30 After analysis and weighting, data are stored in SQL data base If data change, new fields are created in the database Staff gets new information in less than two weeks From 1-2 datasets per year to 10 data sets
 must be adjusted when used for rates—particularly if cell size is less than 30 After analysis and weighting, data are stored in SQL data base If data change, new fields are created in the database Staff gets new information in less than two weeks From 1-2 datasets per year to 10 data sets.")
10
Comparable Managing Dynamic and Calculated Data Collaboration is critical Report Developers must work with Front end users who generate the data Managers who determine what is useful and or interpret the data Report Developers must also collaborate with Users of the Data Public Health leaders Stakeholders Partners Decision-makers Managers and Supervisors Create a Structured approach to identifying and testing data to produce usable information Identify routine process for linking data source to dashboard Recognize and follow requirements from data owners related to privacy and access Produce calculated data through routines Replicable Reliable Systematic

11
Dashboard Development and Deployment Our Health Department uses Dashboard Reporting Software from Logi Analytics

12
REPORT PROCESS All work starts with the Users: Managers and Frontline staff Identify Division / Program needs, indicators, benchmarks and other performance measures Collect Data Extract, Transfer and Load (ETL) the data to appropriate database Build Reports, dashboard and applications Verify that reports accurately represent the indicator or measure Publish
 the data to appropriate database Build Reports, dashboard and applications Verify that reports accurately represent the indicator or measure Publish")
13
Updating Dashboard Applications Updating the dashboard usually involves adding new data to the database The dashboard is updated automatically. Time spent on the initial design of the rules for Analysis, Weighting, Selection, Extraction, Transfer, and Load of data from each type of data source is the most intensive and important. Assuring that the rules can replicated Assuring that the rules can be automated Assuring the rules can be systematically applied Each additional use of the rules th

14
Using Dashboards Easy to Use Improving Public Health Web-based deployment No special software or training required Users control what information they want to see, follow or monitor Assure Quality Service & Performance Promote Healthy Behaviors—Use of data to support and reinforce change Monitor Community Health Status /Risks Benchmark performance and measure outcomes

15
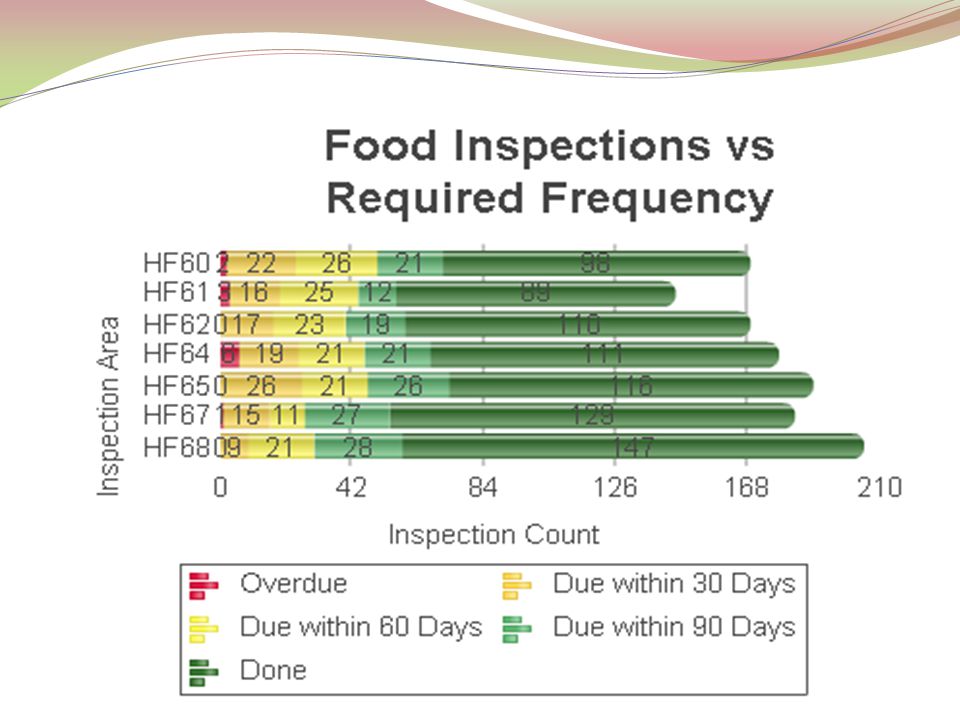
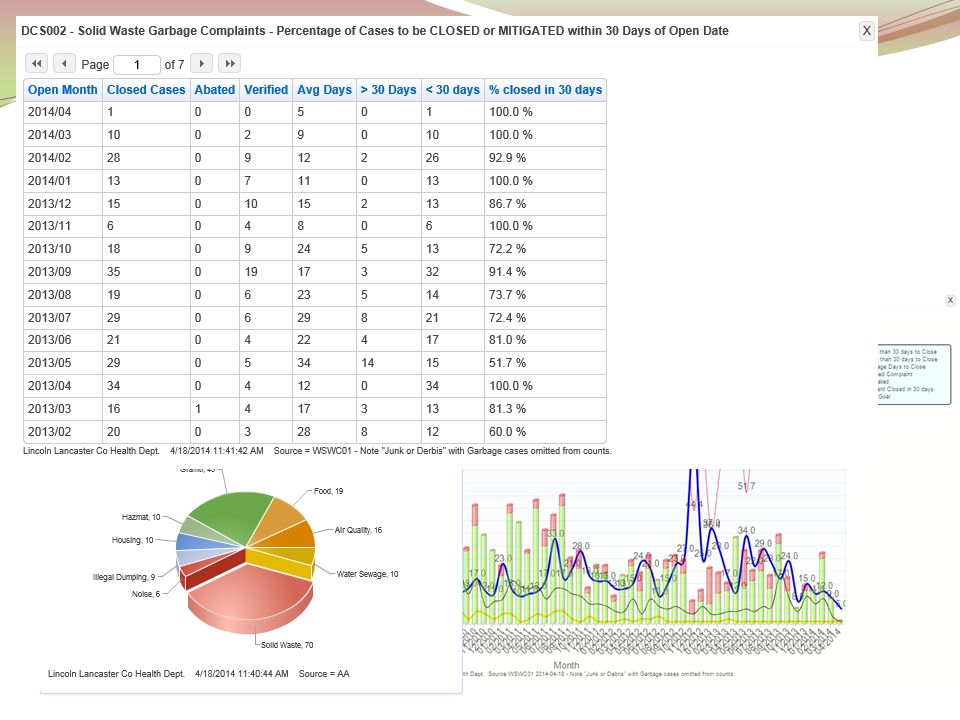
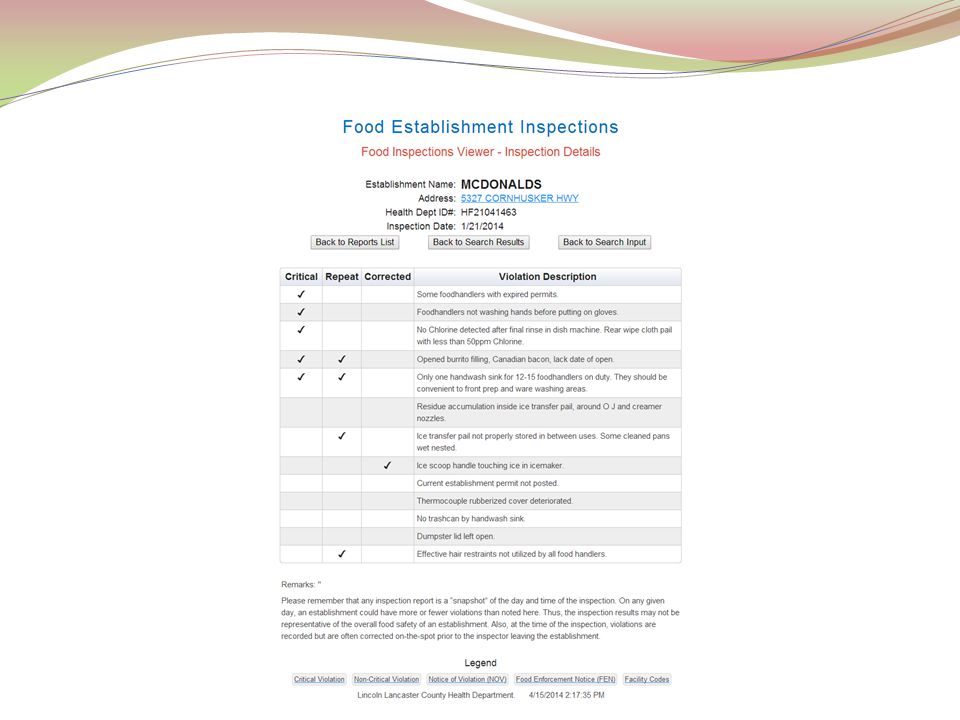
Assure Quality Service & Performance

20
Promote Healthy Behaviors Use of data to support and reinforce change

29
Monitor Health Status Community Health Status Indicators Risk Indicators

36
Benchmark performance Measure outcomes Performance Measures and Indicators

39
Medical Home by 2014

40
Lessons Learned Things to Watch Out For….

41
Helping Users understand information We keep these points in mind and include explanations: Taking care when using “percentage change” and rates for data sets with small cells. When comparing years, the starting and ending years may not be reflective of the real change in values. Know if there are breaks in the data: Deaths classified using ICD 9 in 1998; ICD 10 in 1999 Changes in birth certificates in 2005. BRFSS: Changes in sampling as data collection using cell phone numbers increased led us to make a break between 2010 and 2011 data. We don’t display 2011 and 2012 data in direct comparison with 2010 and earlier data

42
Including confidence intervals and meta data Age adjusted data can’t be compared if different standard populations are used (2000 is the usual standard, but sometimes a different year—say 1946 or 1970, is used). Racial and ethnic definitions have changed in Census data for races and persons of Hispanic origin. Don’t be overly precise—survey data have confidence intervals to consider.

43
GIS is powerful but ….. GIS maps often raise more questions than they answer (counties next to each other may appear to have widely differing rates): For cancer incidence, be careful, as cancer is age related and residential care and nursing homes are not located in all counties
: For cancer incidence, be careful, as cancer is age related and residential care and nursing homes are not located in all counties.")
44
Wrap up Best Practices Contacts

45
LLCHD Public Health Informatics Program Model Practice Program Award Winner: July 2011 Best Practices / Model Practice Best Practices we used: Business Process Analysis Requirements Gathering Strategic Mapping and Planning Business Case LHDs and Electronic Health Records Webinar Why should your local health department (LHD) adopt and utilize electronic health records? Webinar that spotlights Lincoln-Lancaster County Health Department and Marion County Health Department use of electronic health records and how it has improved their public health practice.

46
Questions ? / More information? View some of our dashboards: http://data.publichealthne.orghttp://data.publichealthne.org Developed with the Public Health Association of Nebraska for all Nebraska local health districts http://lincoln.ne.gov/cityhttp://lincoln.ne.gov/city Key word: data Raju Kakarlapudi Public Health Epidemiologist Lincoln-Lancaster County Health Department 3140 N Street Lincoln, NE 68510 402-441-6270 rkakarlapudi@lincoln.ne.gov Kathleen Cook Information & Fiscal Manager Lincoln-Lancaster County Health Department 3140 N Street Lincoln, NE 68510 402-441-8092 kcook@lincoln.ne.gov

Similar presentations





















 Health Department.>")
 Betty C. Jung, RN, MPH, CHES.>")




IS?. Purpose of HIS “is to produce relevant information that health system stakeholders can use for making transparent and evidence-based.>")





: Minnesota Project Overview Candy Hanson Program Manager Julie Jacobs HIT Consultant June 13,>")
 For B2C (business to consumer)>")
