Download presentation
Presentation is loading. Please wait.

1
Collapsing Trachea Mark Bohling, DVM Diplomate, American College of Veterinary Surgeons Assistant Professor of Surgery University of Tennessee College of Veterinary Medicine

2
What is Tracheal Collapse? Normal airflow dynamics in respiration Inspiration Expansion of chest by muscles of respiration Pressure gradient - chest negative Effect on the air conduit: Thorax - expansion Neck - compression Expiration Reverse effects

3
History of Collapsing Trachea in Veterinary Medicine Described as early as 1960 Review of early treatments Single plastic tube Ventral chondrotomy Modified ventral chondrotomy Dorsal membrane plication

4
Tracheal Collapse in Other Species Tracheal collapse in human beings History Dates to 1930’s Similarities Softening of tracheal cartilage Lateral collapse (same as dorsoventral in dogs) Differences Classification Primary vs secondary collapse Pediatric vs adult collapse
 Differences Classification Primary vs secondary collapse Pediatric vs adult collapse")
5
Tracheal Collapse in Other Species Tracheal collapse in large animals Horses Congenital Secondary to laryngeal paralysis Cattle Acquired neonatal Tracheal collapse in birds Bordetella avium in turkeys

6
Tracheal Collapse in the Dog Miniature breeds Middle aged to older Other risk factors More pronounced in obese individuals

7
Levels of Collapse NormalG1G2G3G4

8
Levels of Collapse

9
Clinical Signs Chronic, dry nonproductive cough (honking) Intermittent dyspnea (worsens with excitement) Cyanosis & syncope in severe cases Inspiratory/ expiratory dyspnea Prone to heat stroke
 Intermittent dyspnea (worsens with excitement) Cyanosis & syncope in severe cases Inspiratory/ expiratory dyspnea Prone to heat stroke")
10
Clinical Signs

11
Pathophysiology Disease causes the trachea rings to weaken Dorsal ligament and trachealis muscle weaken and stretch Trachea changes from oval tube to a flattened conduit

12
Etiology Congenital Nutritional tracheomalacia Obesity Bacterial infection Neurologic Chronic airway disease Idiopathic – “who knows why”

13
Diagnosis Tracheal palpation Radiographs (inspiratory / expiratory ) Fluoroscopy Tracheoscopy
 Fluoroscopy Tracheoscopy")
14
Radiographs

15
Tracheoscopy

16
Medical Management Cough suppression (Hydrocodone, butorphanol) Bronchial dilators (Aminophylline, terbutaline) Sedation (Acepromazine) Weight loss
 Bronchial dilators (Aminophylline, terbutaline) Sedation (Acepromazine) Weight loss")
17
Medical Management Help control symptoms Can not be cured Disease usually progressive

18
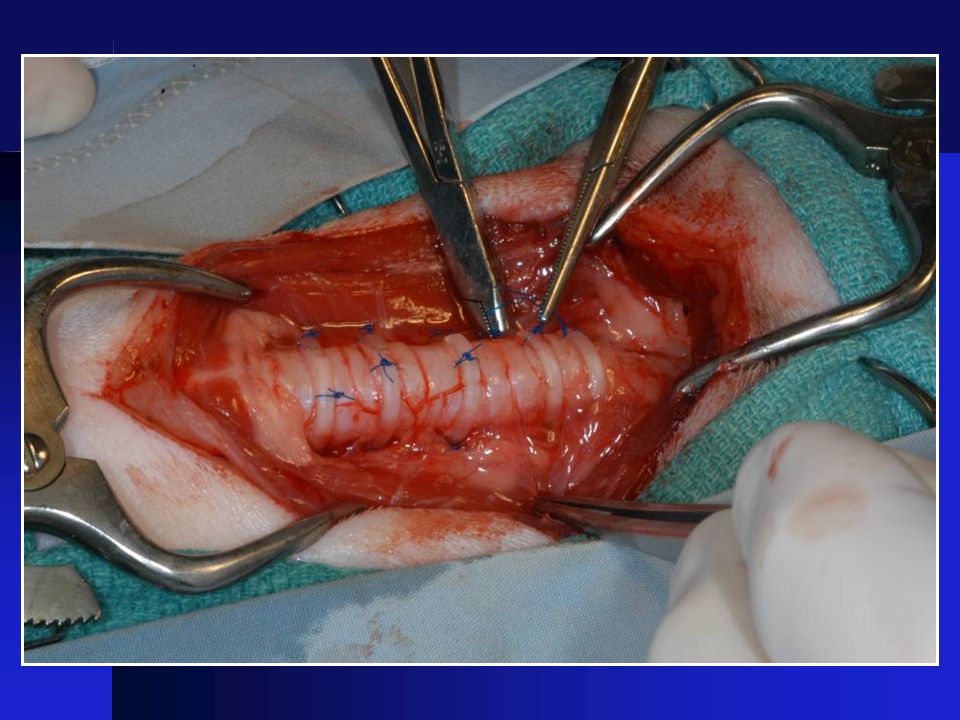
Surgical Correction External stenting with plastic rings

24
BeforeBeforeAfterAfter

25
Surgical Correction External spiral stent

26
Collapse between rings External Stent Complications

27
Damage to recurrent laryngeal nerve External Stent Complications

28
Interruption of tracheal blood supply

29
Internal Stenting What is a stent? History of stenting History of tracheal stenting Modern stents and stent materials Stents in veterinary medicine

30
Ultraflex ® Stent Radiopaque, self-deployed 4 - 8 cm length, 10 - 20mm diameter Made of nitinol (nickel-titanium alloy) Proximal or distal deployment Single strand, open loop knitted design (flexible, contourable) Boston Scientific/ Microvasive.
 Proximal or distal deployment Single strand, open loop knitted design (flexible, contourable) Boston Scientific/ Microvasive.")
31
Ultraflex ® Stent

34
Ultraflex ® Stents

35
SmartStent ® Nitinol tube Laser cut No overlapping wires Less breakage in human vascular applications Cordis Endovascular ®

36
Infiniti Stent Also nitinol Single woven wire Only stent produced exclusively for vet use Claims as yet unproven

37
Stent Placement Stent deployed under fluoroscopic guidance Target – 5mm cranial to bifurcation Placement checked with tracheoscopy

38
Stent in Place

39
Radiographs

40
Postoperative Care Perioperative antibiotics Corticosteroids for 7 days Sedation Cough suppression 24 hours oxygen if needed Humidification

41
6 Month Post Implant

42
Stent Results The little girl with the curl syndrome… Good outcomes… Immediate improvement Breathing near normal Mild chronic cough And the not-so-good outcomes…

43
Stent Complications Stent fracture Granulation in stent Tracheal exudate Additional collapse at ends of stent

44
Fractured Stent

46
Stent Fracture Originally thought to be due to bending stresses All brands/types of nitinol stents can fracture - there is NO unbreakable stent At this time, removal is best option - BUT - not for the fainthearted!

47
Granulation Tissue

49
Tracheal Mucus

50
Collapsed at Ends

51
Stent plus Rings

52
Stent Advantages Preserves tracheal blood supply Preserves recurrent laryngeal nerve Continuous tracheal support Easy deployment Multiple, sequential deployment

53
Rings vs. Stents Cost to client (stent more expensive) Stents are easier and quicker Complication rate similar Neither cure, only control symptoms Stent placement requires expensive equipment Rings require surgical expertise Lack of proper size stent
 Stents are easier and quicker Complication rate similar Neither cure, only control symptoms Stent placement requires expensive equipment Rings require surgical expertise Lack of proper size stent.")
54
A “typical” case with tracheal rings Day 1: Preop workup (bloodwork, radiographs, tracheoscopy) Day 2: Surgery Postop recovery in ICU Day 3: Still in ICU Day 4: Discharged from hospital Home monitoring – continue medical therapy 2 – 4 weeks Recheck time variable, depends on outcome Long term outcome usually good, but…
 Day 2: Surgery Postop recovery in ICU Day 3: Still in ICU Day 4: Discharged from hospital Home monitoring – continue medical therapy 2 – 4 weeks Recheck time variable, depends on outcome Long term outcome usually good, but…")
55
A “typical” case with tracheal stent Day 1: Workup as for rings. Order stent from supplier Day 2: Stent arrives (usually). Stent is placed in a 30 minute procedure and patient recovers in ICU Day 3-4: Recovery in ICU Day 5: Discharge from hospital Home care for 2-4 weeks Re-check tracheoscopy at one month to check if stent is embedded
. Stent is placed in a 30 minute procedure and patient recovers in ICU Day 3-4: Recovery in ICU Day 5: Discharge from hospital Home care for 2-4 weeks Re-check tracheoscopy at one month to check if stent is embedded.")
56
Miss Piggy - Stent disaster case #1 Signalment: Miss Piggy 6 year old spayed female Yorkie Body weight 13 lbs (BCS 8/9!!) Grade III/VI heart murmur History: Coughing for past 2 years, getting worse past yr Presented to emergency clinic Saturday night Unable to breathe, cyanotic Oxygen dependent
 Grade III/VI heart murmur History: Coughing for past 2 years, getting worse past yr Presented to emergency clinic Saturday night Unable to breathe, cyanotic Oxygen dependent")
57
Miss Piggy Presentation at UT Still oxygen dependent Tracheoscopy findings: Cervical - Grade 3 entire length Thoracic - Grade 3-4 entire length Left main bronchus Grade 2-3 Plan: stent entire trachea Poor anesthetic risk Guarded prognosis given

58
Miss Piggy Stent placement Thoracic stent 1 cm cranial to carina 5mm overlap at thoracic inlet Cervical stent 1 cm caudal to cricoid

59
Miss Piggy Postop first 24 hours Doing well in oxygen Next day… Trial period out of oxygen - - cough and cyanosis Back to oxygen and medical mgmt Antitussives Bronchodilators

60
Miss Piggy 3rd postop day Brief trial out of oxygen - - same result Still looks good in oxygen 4th postop day 4am “can’t get comfortable” 7am - 7pm: awake all day 9pm: lung sounds getting “harsh” 11pm: crackles ausculted

61
Miss Piggy 5th day…. Early am hours - No response to bronchodilators or diuretics Patient very tired, has not slept in 24 hours 9am - respiratory failure

62
Stent disaster #2 - Tuffy Signalment: 4 year old male castrated Yorkie BW 8 lbs, BCS 6/9 History: Started at 2 years old Now coughs at slightest exertion Cyanotic with mild exercise

63
Tuffy Tracheoscopy: Cervical collapse - grade 3 Thoracic collapse - also grade 3 Bronchi both open Plan: Stent entire trachea

64
Tuffy Immediate postop Doing well! 3 weeks later… “gagging” noticed Recheck at UT BOTH stents fractured Tracheal lumen open but small Lots of exudate

65
What next? Immediate plan Stabilize his condition Antibiotics Some antitussives Definitive plan Stent removal Re-stent over the broken ones

66
Tuffy – the outcome Survived the procedure! Immediate improvement in breathing Went home doing well, but some cough Continued to improve Still coughs some Overall quality of life – better than before Cost to owner: $5K+ total, lots of gray hair!

67
Future Needs Immediate needs: Improved surgical treatment options Less breakable stents Improved rings - can we go intrathoracic? Improved medical management options Cough suppression with less sedation Tracheal cartilage - can malacia be arrested?

68
Future Needs Long-term needs Greater understanding of the etiology of this process What is happening at the cellular and molecular level? Identification of molecular/genetic marker(s) Creation of a breed registry for this disease Apparent genetic cause Can we “breed it out”?
 Creation of a breed registry for this disease Apparent genetic cause Can we breed it out .")
69
Special thanks to: Dr DJ Krahwinkel Sue Schwarten Danielle Browning UT photo and media services Linda Hicks and Mr T

70
Thank you – any questions?

Similar presentations