Download presentation
Presentation is loading. Please wait.

1
Strategic Leadership for Health System Transformation W. Henry Mosley

2
Where do leaders operate? Beyond Imagination That’s Impossible Looks Difficult Easy to do

3
What is difficult? Impossible? Beyond imagination?

4
Our best thinking got us here. The problems that we face cannot be solved by the same level of thinking that created them. Albert Einstein

5
The Present Health System Is Perfectly Designed to Produce the Present Results If we want the same results, let us keep the present system!

6
If We Want New Results, We Need to Redesign Our Health Production System

8
Relationship between income and malnutrition

9
The “disconnect” between income and malnutrition Alternatively, Malnutrition “falls” independent of “rises” in income (among the lowest income countries)
")
10
Interest groups Policymakers, planners Managers, providers Communities, households MIS Evaluations Research, pilot projects Leadership the old way The “Blueprint” Strategy Health Project Blueprints

11
Mental Models Sustaining the Blueprint Strategy Highly placed professionals have sufficient knowledge to prescribe interventions that will work in any social context Knowledge from “evidence-based” intervention research done in specific contexts have universal applicability Knowledge from “evidence-based” intervention research done in specific contexts have universal applicability Time-limited, pre-designed, inflexible projects are the best means of introducing innovative health interventions in any setting

12
Mental Models Sustaining the Blueprint Strategy (c ontinued) The institutions, personnel and services of National Ministries of Health constitute the “health system” of a country Short-term material investments and focused technical assistance to the MOH will produce sustainable improvements in a country’s health Using outside “experts” to gather, analyze, interpret and publish data is an effective means of gaining an understanding of the realities in the field
 The institutions, personnel and services of National Ministries of Health constitute the health system of a country Short-term material investments and focused technical assistance to the MOH will produce sustainable improvements in a country’s health Using outside experts to gather, analyze, interpret and publish data is an effective means of gaining an understanding of the realities in the field")
13
Interest groups Policymakers, planners Managers, providers Communities, households MIS Evaluations Research, pilot projects The “Blueprint” Strategy A fundamental flaw Health LearningAction Project Blueprints Disconnects learning from action

14
Social Consequences of Blueprint Projects No (or limited) learning by the front-line health workers – who are the members of the households and communities where the action is taking place No (or limited) learning by the front-line health workers – who are the members of the households and communities where the action is taking place Therefore, no fundamental changes in behaviors and no sustainability after the project is completed Evidence – Look at the health disparities among developing countries and the inequities within countries after 50 years of top down projects
 learning by the front-line health workers – who are the members of the households and communities where the action is taking place No (or limited) learning by the front-line health workers – who are the members of the households and communities where the action is taking place Therefore, no fundamental changes in behaviors and no sustainability after the project is completed Evidence – Look at the health disparities among developing countries and the inequities within countries after 50 years of top down projects")
15
Donor Aid in Developing Countries Too Often Produces Little Sustainable Benefits The twin tragedies of global poverty 1 So many people in developing countries are seemingly fated to live horribly stunted lives and die such early deaths After 50 years and more than $2.3 trillion in aid from the West, there is shockingly little to show for it. 1 Paraphrased from: William Easterly, The White Man’s Burden. Why the West’s efforts to aid the rest have done so much ill and so little good. Penguin Press, NY, 2006

16
So what do we need to change? Ourselves first – We need to: Break down the walls between all our formal institutions and learn to communicate with each other Engage the people from the community and all sectors of government in a learning process to deepen our understanding of the realities of human development

17
To change the way we act, we must first change the way we think A first step is to change our “Mental Model” of what constitutes the “health system” of a country

19
You are the Minister of Agriculture. You are asked by a reporter from CNN to describe the agricultural system in your country. What is your answer? Do You Really Know What Are the Production Systems of Your Country?

20
Mental Models Define Our “Reality” and Pre-determine the Choices We Make and the Actions We Take Mental Models Define Our “Reality” and Pre-determine the Choices We Make and the Actions We Take Who “produces crops” in your mental model of the agricultural system? How does your answer determine the roles and functions of the Ministry of Agriculture?

21
You are the Minister of Health. You are asked by a reporter from CNN to describe the health system in your country. You are the Minister of Health. You are asked by a reporter from CNN to describe the health system in your country. What is your answer? Do You Really Know What Are the Production Systems of Your Country?

22
Mental Models Define Our “Reality” and Pre- determine the Choices We Make and the Actions We Take Mental Models Define Our “Reality” and Pre- determine the Choices We Make and the Actions We Take Who “produces health” in your mental model of the health system? How does your answer determine the roles and functions of the Ministry of Health?

23
The Household Production of Health The Household Production of Health Premises 1. Households are the primary units for the production of health.

24
Households Mothers are the primary managers and implementers of the household health production tasks, and women and children are the major “beneficiaries/victims” Therefore gender relations and status of women are key determinants of health in the developing world

25
The Household Production of Health Premises (continued) 2. Households, like every social institution, have three basic capabilities for the production of the desired outputs Resources Practices Values

26
Material money housing possessions utilities property equipment technologies Non-material gender time health ethnicity/language beliefs/knowledge/skills reputation social status social networks self-image/motivation Resources Productive Capabilities

27
Formal Sanctioned by laws, religion, regulations, relating to: marriage/divorce property rights interpersonal relationships gender/sexual/violence personal mobility labor force participation Informal The customary ways of making decisions, taking actions relating to: gender roles marital relations child marriage/violence sexual relations health care provision money management freedom of mobility Productive Capabilities Practices

28
Values Progress resistant Hierarchical Status based on birth/gender Knowledge from traditions Conformity honored Destiny due to fate Past/present oriented Closed minded, arrogant Suspicion of “others” Success by relationships Progress Promoting Egalitarian Status by achievement Learning by trial and error Creativity, innovation honored Destiny from self-reliance Future oriented Open minded, self-critical Mutual trust Success based on merit

29
Households Values PracticesResources 1. Which health production capabilities are more important – material or non-material? Which do we measure? Why? 2. What do we mean when we say that a person or household is “resourceful”? Can we measure it? How?

30
Values Practices Resources A culture is the product of the interactions of:

31
Culture The DNA of Social Institutions Culture is self-replicating from generation to generation Like DNA, a cultural system is resistant to change Externally driven development programs typically ignore culture – Why?

32
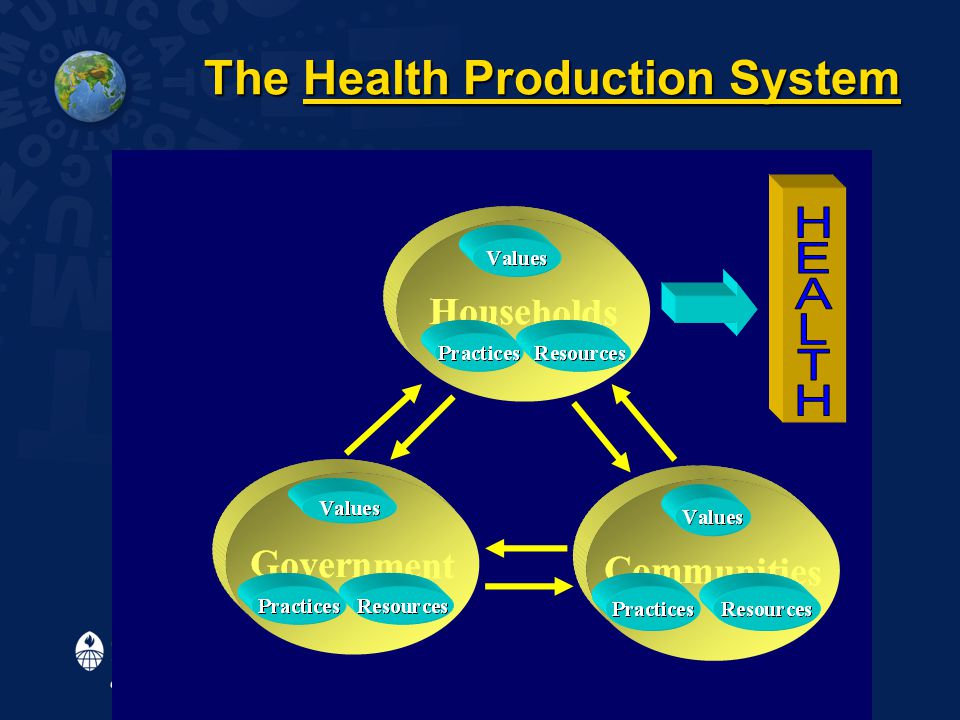
The Household Production of Health Premises (continued) 3. Households produce health in the context of the local community and the wider society – which is a nation’s health production system. 3. Households produce health in the context of the local community and the wider society – which is a nation’s health production system.

33
Households Government Communities The Health Production System

35
Interest groups Policymakers, planners Managers, providers Communities, households MIS Evaluations Research, pilot projects The “Blueprint” Strategy What values dominate? Health LearningAction Project Blueprints Disconnects learning from action

36
Productive Capabilities Values Progress resistant Hierarchical Status based on birth/gender Knowledge from traditions Conformity honored Destiny due to fate Past/present oriented Closed minded, arrogant Suspicion of “others” Success by relationships Progress Promoting Egalitarian Status by achievement Learning by trial and error Creativity, innovation honored Destiny from self-reliance Future oriented Open minded, self-critical Mutual trust Success based on merit

37
What Are the Health Production Capabilities? For every 1000 families* in an LDC, complete the following RESOURCESGovernmentHouseholds - Health providers - Funds/capita/year - Preventive skills - Curative skills PRACTICES - Hours/day - Days/week VALUES - Motivation <5 2000 – 4000+ $400 HighLow ~824 ~57 LowHigh *About 5,000 persons

38
The Burden of Disease What are the health problems in the population, and how do they come about? Source: WHO, World Health Report 2002. Reducing Risks, Promoting Healthy Life

39
What are the “household production” tasks that relate to the “burden of disease”? Undernutrition – food production/purchase and storage; dietary selection and meal preparation; family food allocation; dietary practices in pregnancy and postpartum; breastfeeding and complementary feeding practices; etc.

40
What are the “household production” tasks that relate to the Burden of Disease? What are the “household production” tasks that relate to the Burden of Disease? Unsafe sex – negotiating gender roles and sexual relationships, “protecting” unmarried daughters (and sons), delaying sexual debut, arranging marriages, secluding women, limiting sexual partners, practicing contraception, obtaining abortions, utilizing condoms, etc.
, delaying sexual debut, arranging marriages, secluding women, limiting sexual partners, practicing contraception, obtaining abortions, utilizing condoms, etc..")
41
Unsafe water, sanitation and hygiene – collection, storage, utilization of water; bathing, washing clothing, bedding, utensils, use of soap; food preparation (incl. infant formula) and storage; latrine practices and waste disposal; etc. Indoor smoke from solid fuel – collection of biomass for fuel; use of open indoor fires; lack of windows, etc What are the “household production” tasks that relate to the Burden of Disease?
 and storage; latrine practices and waste disposal; etc. Indoor smoke from solid fuel – collection of biomass for fuel; use of open indoor fires; lack of windows, etc What are the household production tasks that relate to the Burden of Disease .")
42
From 70 – 90% of all sickness care takes place in the home* Household members, especially mothers: make the primary diagnoses of illnesses assess the severity and likely outcomes select among available providers and treatment options procure and administer treatments How about sickness care? *Source: WHO, World Health Report 2002. Reducing Risks, Promoting Healthy Life

43
Leadership Challenges in Health 1. 1. How do you get all the diverse actors in a “multi-minded” health production system to move together in towards a common goal? 2. 2. How do you overcome the barriers to change generated by long-standing, self-sustaining institutional cultures at every level?

44
Leadership Skills for Change Catalytic - Shared Vision of a health future that people want to create Enabling - Teamwork with trust, open- mindedness, transparency and mutual accountability for all outcomes Learning – Generating new knowledge to mobilize the vast resources of ordinary people for change

45
Policymakers, planners Managers, providers Communities, households Needs Tasks Outputs Competencies Demand Decisions Leadership the New Way - “Learning Organization” Strategy Interest groups Learning Health 3 1 2 Linking Action to Learning

46
Policymakers, planners Managers, providers Communities, households Needs Tasks Outputs Competencies Demand Decisions “Learning Organization” Strategy What values dominate? Interest groups Learning Health 3 1 2 Linking Action to Learning

47
Productive Capabilities Values Progress resistant Hierarchical Status based on birth/gender Knowledge from traditions Conformity honored Destiny due to fate Past/present oriented Closed minded, arrogant Suspicion of “others” Success by relationships Progress Promoting Egalitarian Status by achievement Learning by trial and error Creativity, innovation honored Destiny from self-reliance Future oriented Open minded, self-critical Mutual trust Success based on merit

48
Maternal Mortality - Blueprint Project Can the community participate here? Strategic objective – Reduce MMR by 20% - from (500/100,000 to 400/100,000) in 5 years.
 in 5 years..")
49
Maternal Mortality - Shared Vision Can the community participate here? Shared Vision - No mother dies from child birth in our community. Should we do it alone? Or through the Learning Organization?

50
Bureaucratic Perceptions 4% MMR reduction/year is “easy to do.” 10% MMR reduction/year is “difficult!” 25% MMR reduction/year is “impossible!” Elimination of MMR is “beyond imagination!”

51
Where do leaders operate? Beyond Imagination That’s Impossible Looks Difficult Easy to do

52
Does your country have a Shared Vision? Government goal - reduce MMR by 4% every year! Community goal - Zero MMR! Household goal - Zero MMR!

53
Question Should a vision be achievable under present conditions?

54
Shared vision asks: What do we want to happen? Or What do we want to create? NOT What is feasible given present conditions?

55
Should visions be based on situation analysis? Should we want only what we can have given the current situation? Should we aim for what we truly want and change the current situation?

56
A few questions 1. Do you have a national shared vision for reproductive health? 2. Do you have a shared vision for RH in your organization? 3. Can everyone describe what the shared vision is? 4. If you don’t have a shared vision, what is the reason?

57
Key question Do families, the primary producers of health, participate in shaping the reproductive health vision for their community?

58
Exciting and Sustaining Action by Every Team Member Exciting and Sustaining Action by Every Team Member Does every frontline worker know: what the goal is? what the goal is? what the score is in their community? what the score is in their community? what their part is on the team? what their part is on the team? how well they are performing? how well they are performing?

59
Resourcefulness “Development can be neither given nor received – it must come from within…. What the less developed have been most deprived of is not the fruits of development, but the opportunity to develop themselves.” Jamshid Gharajedaghi

61
What is difficult? Impossible? Beyond imagination?

62
Leadership – Helping People Be More “Resourceful” in Producing Health Leadership – Helping People Be More “Resourceful” in Producing Health Old way Professionals in facilities providing services New way Resourceful households producing health Transforming the health system

63
THE WISDOM OF TAO XVII RULERS Of the best rulers The people only know that they exist, The next best they love and praise, The next they fear, And the next they revile. When they do not command the people's faith, Some will lose faith in them, And then they resort to oaths! But of the best, when their task is accomplished, their work done, The people all remark, "We have done it ourselves." Source: The Wisdom of China and India by Lin Yuntang

64
Where do leaders operate? Beyond Imagination That’s Impossible Looks Difficult Easy to do

Similar presentations

















>")


 County Health Department.>")
IS?. Purpose of HIS “is to produce relevant information that health system stakeholders can use for making transparent and evidence-based.>")