Download presentation
Presentation is loading. Please wait.

1
The “middle-income” curse: Should global aid and treatment access decisions be based on national economic criteria?

2
“Middle Income” Countries
Has replaced the phrase developing countries Middle Income countries are classified by the World Bank Based purely on gross per capita income World Bank categories Upper Income Middle Income Upper middle income Lower middle income Low Income

3
Human Development Index v. World Bank Classification
More than half of the world’s poor live in middle income countries HDI based on: Three dimensions: Health, Education, Living standards Four indicators: Life expectancy at birth, mean years of schooling, expected years of schooling, gross national income per capita Countries like India and Indonesia in Asia or Sudan and South Africa which are middle income rank poorly in terms of human development (128 and 111; 141 and 121) Inequality within countries remains extremely high (2006 Human Development Report): The richest 20% of the population in Bolivia had an HDI rank 97 positions higher than the poorest 20%. In South Africa the top quintile ranks 101 positions above the lowest. Furthermore, the top quintile in the United States has an HDI value that exceeds all other countries for which the statistic was computed, while the poorest quintile ranks 49 positions lower. Add the Gini co-efficient which measures income inequality within countries and the scenario is stark .
 Inequality within countries remains extremely high (2006 Human Development Report): The richest 20% of the population in Bolivia had an HDI rank 97 positions higher than the poorest 20%. In South Africa the top quintile ranks 101 positions above the lowest. Furthermore, the top quintile in the United States has an HDI value that exceeds all other countries for which the statistic was computed, while the poorest quintile ranks 49 positions lower. Add the Gini co-efficient which measures income inequality within countries and the scenario is stark .")
5
UN’s Least Developed Country list v. World Bank Classification
UN: Least Developed Country (LDC): a low-income criterion, based on a three-year average estimate of the gross national income (GNI) per capita (under $750 for inclusion, above $900 for graduation); a human resource weakness criterion, involving a composite Human Assets Index (HAI) based on indicators of: (a) nutrition; (b) health; (c) education; and (d) adult literacy; and an economic vulnerability criterion, involving a composite Economic Vulnerability Index (EVI) based on indicators of: (a) the instability of agricultural production; (b) the instability of exports of goods and services; (c) the economic importance of non-traditional activities (share of manufacturing and modern services in GDP); (d) merchandise export concentration; and (e) the handicap of economic smallness (as measured through the population in logarithm); and the percentage of population displaced by natural disasters. Example: Bhutan World Bank: Middle Income Country UN: LDC
: a low-income criterion, based on a three-year average estimate of the gross national income (GNI) per capita (under $750 for inclusion, above $900 for graduation); a human resource weakness criterion, involving a composite Human Assets Index (HAI) based on indicators of: (a) nutrition; (b) health; (c) education; and (d) adult literacy; and. an economic vulnerability criterion, involving a composite Economic Vulnerability Index (EVI) based on indicators of: (a) the instability of agricultural production; (b) the instability of exports of goods and services; (c) the economic importance of non-traditional activities (share of manufacturing and modern services in GDP); (d) merchandise export concentration; and (e) the handicap of economic smallness (as measured through the population in logarithm); and the percentage of population displaced by natural disasters. Example: Bhutan. World Bank: Middle Income Country. UN: LDC.")
6
Impact of adopting World Bank Classification
Middle Income countries Majority are WTO members Applying the TRIPS Agreement: Patents on second and third line medicines Negotiating Free Trade Agreements Increasingly facing a treatment and funding crisis Three examples: “Access” programmes of MNC pharma Medicines Patent Pool licences Global Fund

7
Middle Income Countries and “access” programmes of Multinational Pharmaceutical Companies

8
Companies All multinational companies – primarily the patent holders on key ARVs, have access programmes of some sort Some follow differential pricing i.e. different (lower) prices in developing countries Some follow voluntary licencing i.e. licences given to generic companies to manufacture and supply generic versions of their patented medicines
 prices in developing countries. Some follow voluntary licencing i.e. licences given to generic companies to manufacture and supply generic versions of their patented medicines.")
9
What happened to the price discounts?
2011 – MSF analysis reveals that several MNCs have “Shut Down HIV Drug Discount Programmes In Middle-Income Countries” Tibotec/ Johnson & Johnson exclude all countries classified as ‘middle-income’ ViiV (Pfizer + GlaxoSmithKline) no longer offers reduced prices to middle-income countries, even when programmes are fully funded by the Global Fund to fight AIDS, TB and Malaria or the US-government’s PEPFAR programme. Merck: Will no longer issue price discounts for 49 middle-income countries for raltegravir. India, Indonesia, Thailand, Viet Nam, Ukraine, Colombia and Brazil Brazil pays $5,870 per patient per year for raltegravir In LDCs, Merck charges $675 per patient per year for the drug, “Access” programmes touted as voluntary solutions that big pharma offers appear unreliable and unsustainable in the long term Middle-income countrieswill now have to negotiate discounted prices on a case-by-case basis.
 no longer offers reduced prices to middle-income countries, even when programmes are fully funded by the Global Fund to fight AIDS, TB and Malaria or the US-government’s PEPFAR programme. Merck: Will no longer issue price discounts for 49 middle-income countries for raltegravir. India, Indonesia, Thailand, Viet Nam, Ukraine, Colombia and Brazil Brazil pays $5,870 per patient per year for raltegravir. In LDCs, Merck charges $675 per patient per year for the drug, Access programmes touted as voluntary solutions that big pharma offers appear unreliable and unsustainable in the long term. Middle-income countrieswill now have to negotiate discounted prices on a case-by-case basis.")
10
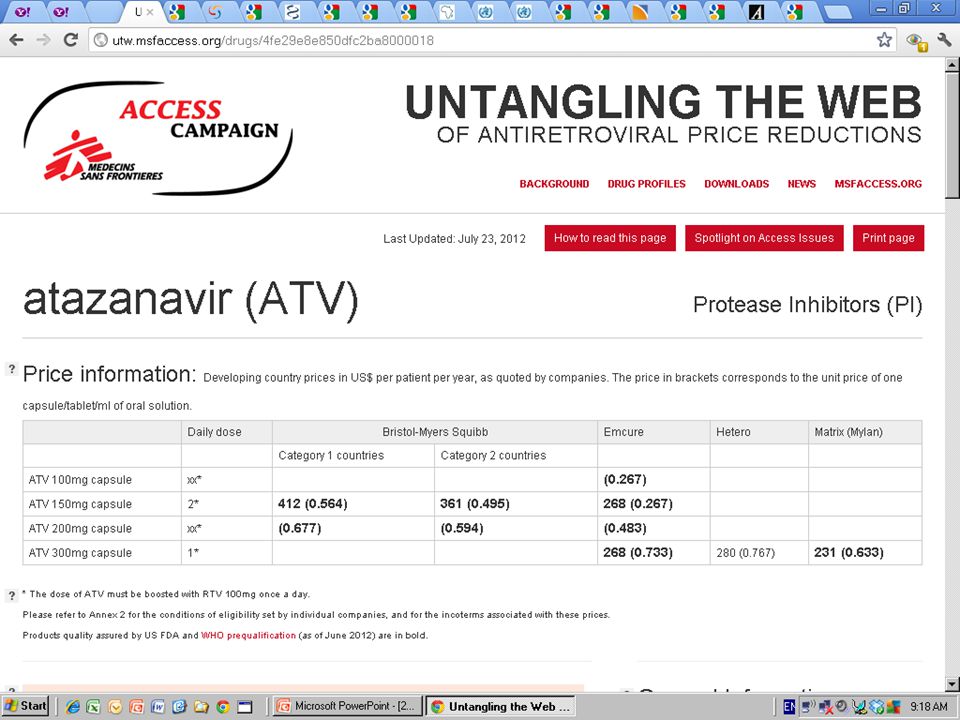
BMS - Atazanavir Category 1 countries: BMS includes in Category 1 all sub-Saharan African countries (except Southern African countries), plus countries classified as low-income by the World Bank (except North Korea, Kyrgyzstan, Moldova and Uzbekistan). Category 2 countries: BMS includes in Category 1 all Southern African countries. Botswana; Lesotho; Malawi; Mozambique; Namibia; South Africa; Swaziland; Zambia; Zimbabwe. For other developing countries, prices are negotiated on a case-by-case basis
, plus countries classified as low-income by the World Bank (except North Korea, Kyrgyzstan, Moldova and Uzbekistan). Category 2 countries: BMS includes in Category 1 all Southern African countries. Botswana; Lesotho; Malawi; Mozambique; Namibia; South Africa; Swaziland; Zambia; Zimbabwe. For other developing countries, prices are negotiated on a case-by-case basis.")
13
Middle Income Countries and the Patent Pool-Gilead Licences

14
Background Medicines Patent Pool on 12 July 2011, the first production licences with Gilead Sciences tenofovir disoproxil fumarate (“TDF”) Emtricitabine (FTC) elvitegravir (“EVG”), cobicistat (“COBI”) QUAD (combination of all four) As opposed to companies, this mechanism is supposed to be health driven
 Emtricitabine (FTC) elvitegravir ( EVG ), cobicistat ( COBI ) QUAD (combination of all four) As opposed to companies, this mechanism is supposed to be health driven.")
15
The “Territories”

16
”TDF TERRITORIES” (112 countries)
Additions to TDF territory in the new licence Anguilla (British overseas territory), Armenia, Aruba, British Virgin Islands, Ecuador, El Salvador, Fiji Islands, Georgia, Kazakhstan, Montserrat (British overseas territory), Nauru, Palau, Southern Sudan, Sri Lanka, Tonga, Turkmenistan, Turks and Caicos (British overseas territory) Who is left out of TDF territory: Asia: Malaysia, North Korea, China, Philippines Latin America: Argentina, Brazil, Chile, Colombia, Paraguay, Peru, Uruguay, Venezuela Central America: Costa Rica, Mexico, Panama, Middle East: Iran, Iraq, Lebanon, Jordan Eastern Europe & Baltics: Albania, Azerbaijan, Belarus, Bulgaria, Croatia, Czech Rep, Estonia, Hungary, Latvia, Lithuania, Montenegro, Poland, Republic of Kosovo, Republic of Macedonia, Romania, Russia, Serbia, Slovak Rep, Turkey, Ukraine, Africa: Algeria, Egypt, Morocco, Tunisia, Libya Island Nations: Marshall Islands, Micronesia,
, Armenia, Aruba, British Virgin Islands, Ecuador, El Salvador, Fiji Islands, Georgia, Kazakhstan, Montserrat (British overseas territory), Nauru, Palau, Southern Sudan, Sri Lanka, Tonga, Turkmenistan, Turks and Caicos (British overseas territory) Who is left out of TDF territory: Asia: Malaysia, North Korea, China, Philippines. Latin America: Argentina, Brazil, Chile, Colombia, Paraguay, Peru, Uruguay, Venezuela. Central America: Costa Rica, Mexico, Panama, Middle East: Iran, Iraq, Lebanon, Jordan. Eastern Europe & Baltics: Albania, Azerbaijan, Belarus, Bulgaria, Croatia, Czech Rep, Estonia, Hungary, Latvia, Lithuania, Montenegro, Poland, Republic of Kosovo, Republic of Macedonia, Romania, Russia, Serbia, Slovak Rep, Turkey, Ukraine, Africa: Algeria, Egypt, Morocco, Tunisia, Libya. Island Nations: Marshall Islands, Micronesia,")
17
TDF “Territory” BLUE: Countries included in previous TDF licence
PURPLE: New additions to TDF territory RED: Countries where generic supply is not permitted under Pool licences TDF “Territory”

18
”COBI TERRITORIES” (103 countries)
COBI territory not the same as TDF “Territory” Who is left out of COBI territory: Asia: Malaysia, North Korea, China, Philippines + Kazakhstan + Sri Lanka + Thailand + Turkmenistan + Indonesia Latin America: Argentina, Brazil, Chile, Colombia, Paraguay, Peru, Uruguay, Venezuela + Ecuador + El Salvador Central America: Costa Rica, Mexico, Panama Middle East: Iran, Iraq, Lebanon, Jordan Eastern Europe & Baltics: Albania, Azerbaijan, Belarus, Bulgaria, Croatia, Czech Rep, Estonia, Hungary, Latvia, Lithuania, Montenegro, Poland, Republic of Kosovo, Republic of Macedonia, Romania, Russia, Serbia, Slovak Rep, Turkey, Ukraine Africa: Algeria, Egypt, Morocco,Tunisia,Libya + Botswana + Namibia Island Nations: Marshall Islands, Micronesia,

19
”EVG-QUAD TERRITORIES” (99 countries)
EVG – Quad territory not the same as TDF and COBI “Territory” Who is left out of EVG-QUAD territory: Asia: Malaysia, North Korea, China, Philippines + Kazakhstan + Sri Lanka + Thailand + Turkmenistan + Indonesia Latin America: Argentina, Brazil, Chile, Colombia, Paraguay, Peru, Uruguay, Venezuela + Ecuador + El Salvador + Dominican Republic Central America: Costa Rica, Mexico, Panama, + Aruba Middle East: Iran, Iraq, Lebanon, Jordan Eastern Europe & Baltics: Albania, Azerbaijan, Belarus, Bulgaria, Croatia, Czech Rep, Estonia, Hungary, Latvia, Lithuania, Montenegro, Poland, Republic of Kosovo, Republic of Macedonia, Romania, Russia, Serbia, Slovak Rep, Turkey, Ukraine, Africa: Algeria, Egypt, Morocco, Tunisia, Libya + Botswana + Namibia Island Nations: Marshall Islands, Micronesia, + Montserrat

20
COBI/EVG/QUAD “Territory”
BLUE: Countries included in COBI/EVG/QUAD RED: Countries where generic supply is not permitted under Pool licences COBI/EVG/QUAD “Territory”

21
Patent Pool Mandate UNITAID press release: Given that UNITAIDs mandate is to ensure that medicines are made available according to public health needs, and particularly in countries where the disease is widespread, the Patent Pool plan aims to enable both low- and middle-income countries to benefit from the work of the Patent Pool. Patent Pool-Unitaid MoU: Patent Pool interpretation: The Pool has been mandated by UNITAID to seek inclusion of all developing countries, and considers the geographical scope to be a key area where these licences could be improved. UN High Level Meeting: patent pools that benefit ALL developing countries

22
Who is out? Who is out: Countries in conflict
Libya . Egypt . Tunisia . Countries that are going through conflicts or upheavals. Several countries that typically under-report their epidemics and where people living with HIV are more reliant on the private sector market than government programmes for improved treatment. North Africa and the Middle East for instance. Both regions are out of the licence for TDF and for the newer medicines. Who is out: Countries with TRIPS-plus provisions, little donor money and in more FTA negotiations China and Russia have imposed data exclusivity. Peru, Jordan, Ukraine, Mexico, Costa Rica have got TRIPS-plus measures thanks to FTAs with the US. Malaysia, Peru and Chile are in talks for another US FTA. In Eastern Europe, several of the excluded countries are candidates for EU accession. And nearly all of them are in FTA negotiations with the EU.

23
Who is out: Countries with some of the oldest HIV treatment programmes
Nearly the whole of the Latin American continent has been left out of the Pool. In many of these countries, Brazil in particular, governments started HIV treatment programme much earlier than the rest of the developing world. As a result their cohort of people developing resistance and in need of newer medicines is much larger than other countries currently in the Gilead licence. Who is out: Regions with growing epidemics Barring a few countries, Eastern Europe finds itself almost totally excluded from the Gilead licence. UNAIDS points to the growing epidemic in these countries. Of the countries mentioned in the fact sheet below, Russia and the Ukraine are excluded from the TDF territory while Kazakhstan is excluded from the territory for the newer drugs.

25
Patent Pool licence geographic scope on Africa: Exclusion of Botswana and Namibia
2006 Gilead tenofovir licences 2011 Gilead Patent Pool licence for tenofovir 2011 Gilead-Patent Pool licence for new ARVs

26
Published September, 6 th 2010 Middle income category costs Botswana HIV fight, VP says APA-Gaborone (Botswana) Botswana’s Vice President and acting National Aids Council (NAC) Chairman, Lt. Gen. Mompati Merafhe, said on Monday that the Southern African country’s need of more than US$1 billion for its 2010/11 HIV/AIDS programmes is not helped by the fact that Botswana is classified as Middle Income Country thus loses loan opportunities. Speaking at the NAC meeting on Monday, Merafhe said although the Botswana Government continues to commit resources to HIV and AIDS, its classification as a Middle Income Country comes at a cost as it continues to lose opportunities for concessional loans and grants. “Fund raising efforts for the fight against HIV/AIDS is estimated at over US$930 million, if successful, they will go a long way in augmenting our meagre resources,” said Merafhe. “We fear for loss of such gains, if we do not get additional financial assistance. It is therefore important that we make use of any fundraising opportunity that comes our way,” said Merafhe. According to an updated report from the National Aids Coordinating Agency (NACA), they had to make cuts and savings from ‘non-critical’ areas to survive the shortfall. The report says most funds were released between July and August to implementing partners.
, they had to make cuts and savings from ‘non-critical’ areas to survive the shortfall. The report says most funds were released between July and August to implementing partners.")
27
Patent Pool: Health needs approach?
Adopting the approach of MNC pharma to VLs and World Bank classification contradicts health needs approach the Patent Pool is supposed to adopt. Instead countries who fall within the artificial economic criteria are being left out of the Pool regardless of their treatment needs or an assessment of other factors like reduced funding that are preventing the scale-up of improved treatment in these countries.

28
“Therefore, it is alarming that many countries in Latin America are excluded from the MPP License with Gilead. According to recent UNAIDS report, countries in this region have spent increasingly their scarce public resources to supply AIDS treatment. In addition, the current scenario of global retreat from international donors for projects on HIV/AIDS affects especially Latin America. The region has often been forgotten and is the only one from the global south that has not been cited in the recent UNGASS 2011 Political Declaration on HIV. In the context faced by our continent, where demand for the incorporation of new drugs protected by patents - as may be the case of cobicistat and elvitegravir - is large, the MPP could play a key role ensuring more affordable prices to these countries. However, this is not what happened in the first license signed with a pharmaceutical company.”

29
Middle Income Countries and the Global Fund

30
10%, 55%, 75%?

31
10%, 55%, 75%? In the past year, debates at the Global Fund of how to continue funding in an increasingly hostile funding environment have led to some “creative” solutions by the Board Among these was the 55% rule proposed in November 2011 i.e. each year, 55% of all funding must go to low income countries. February 2012: the Board Chair announced a proposal called the 75% rule i.e. for lower middle income countries and above, funding for each grant renewal would be limited to 75% of what had originally been approved. As we have seen earlier, the use of the World Bank classification ignores the fact that that the majority of world’s poor live in MICs or that these are the countries struggling with restrictive trade and intellectual property laws May 2012: After considerable opposition by civil society, the Global Fund Board has asked for further analysis of the 55% rule.

32
The Global Fund Secretariat argued that without any changes to the rules, renewals in would be heavily skewed towards MICs. But this is because many countries have transitioned to higher income levels without the concomitant improvements in healthcare or poverty And as noted before many of them are facing patent barriers in access. Civil Society concern: GFATM moving from demand/needs driven to top down/supply driven Other bilateral donors have similarly shifted priorities UNAIDS?

33
Algeria: MARPs programmes have faced a crushing blow – not eligible for 2 years
MENA – Will not be able to pay the cost of treatment – patents, ACTA, FTA… Argentina: activists are asking about sustainability (Programme approved for five years is likely to be retrospectively cut back to two years) India: the experience of getting second line treatment
 India: the experience of getting second line treatment.")
34
Conclusion The use of World Bank criteria to determine access to HIV funding and treatment has gained acceptance in part because of the impression that the “middle income” status of a country indicates the ability of the country or its people to fund HIV programmes or HIV treatment. This does not however reflect actual situations in country including intellectual property barriers or the fact that several HIV programmes with marginalized communities are only in existence because of neutral, evidence based funding from the Global Fund. Such an approach undermines the very basis of Universal Access and is likely to be counterproductive both in the short term (with countries hesitating from adopting evidence of treatment as prevention into policies) and in the long term (as HIV programmes in these countries shrink or are shaped by national priorities and prejudices including in relation to marginalized groups).
 and in the long term (as HIV programmes in these countries shrink or are shaped by national priorities and prejudices including in relation to marginalized groups).")
Similar presentations