Download presentation
Presentation is loading. Please wait.

1
© Children’s Hospice International Children’s Hospice International 13th Annual ChiPACC Conference With technical assistance from Centers for Medicare & Medicaid Services Hosted by Arnold & Porter, LLP April 16, 2014

2
ChiPACC Children’s Hospice International WELCOME! John Gould, Partner, Arnold & Porter LLP Mahnu Davar, Sr. Associate, Arnold & Porter, LLP Melissa Harris, Director, Division of Benefits and Coverage, CMS Ann Armstrong-Dailey, CHI

3
© Children’s Hospice International Children’s Program for All-inclusive Coordinated Care (ChiPACC) Ann Armstrong-Dailey Founding Director Children’s Hospice International
 Ann Armstrong-Dailey Founding Director Children’s Hospice International")
4
CHI PACC: Lessons Learned “CHI’s ultimate goal is to so ingrain the hospice concept into pediatrics that it is considered an integral part of health care for children and adolescents rather than a separate specialty…” 1983, American Academy of Pediatrics Ann Armstrong-Dailey CHI Pioneering Hospice Care for Children

7
CHI Pioneering Appropriate Care Since 1983 CHI paving the way since 1983: Definition/Standards/Glossary of Terms Education and Training World Congresses International Resource Technical Assistance Advocacy Special Programs including ChiPACC

8
DEMOGRAPHICS USA 2005 POPULATION USA: 296 Million Adult Deaths 2.5 Million 36% died under hospice care Child Deaths 53,526 children 0 -19 years 2.2% died under hospice care Children Diagnosed with Life-threatening Condition 1.2 Million

9
Causes of Death Children 1 – 19 Years All Children 1 - 19 Accidents Assault Malignancy Suicide Congenital malformations, deformations Chromosomal anomalies Heart disease Cerebrovascular diseases All Children 1 – 19 w CCC Malignancy 48% Neuromuscular 23% Cardiovascular 17%

10
Causes of Death Infants All Infants Congenital Malformations19.5% Short gestation/LBW16.5% Sudden Infant Death Syndrome7.4% Maternal complications6.3% Complication of placenta, cord or membranes4% Accidents/unintentional4% Infants with CCC Cardiovascular32% Congenital/genetic26% Respiratory17% Neuromuscular14%

11
Need for additional support! Children with chronic illness and complex health care needs are living longer and require creative approaches to delivery of care coordination and PP/HC (HHS) 10.2 Million children (13.9% of US children ages 0-17) have special health care needs. This number is increasing slightly every year. (HHS) CHI and ChiPACC are addressing this urgent need!
 10.2 Million children (13.9% of US children ages 0-17) have special health care needs. This number is increasing slightly every year. (HHS) CHI and ChiPACC are addressing this urgent need!.")
12
As Governments debate changes & reforms to their nation's healthcare programs ChiPACC considered: Cost-effective solution, Step in the right direction, Improved care for less cost! ChiPACC

13
Current models of care do not adequately address needs of children with life- threatening conditions and their families CHI Pioneering Appropriate Care

14
ChiPACC A parent should never have to choose between hospice care and hope for a cure. ChiPACC: Comprehensive compassionate coordinated care for children with life-threatening conditions and their families From time of diagnosis With hope for cure Most appropriate setting based on Family Choice – rather than funding stream

15
Reimbursement dollars, and support, follow the child and family throughout the continuum of care Hospital Home Care Other Hospice Palliative Care ChiPACC increases quality of care AND saves money! ChiPACC Funding Flow

16
ChiPACC Successful “partnership” Congress + CMS + CHI A growing number of states beginning with Florida! 1st in the NATION 2005! Colorado! 1 st 1915 (c) waiver 2006! California waiver approved 2010! New York waiver approved 2010! North Dakota waiver approved 2010! Additional states exploring A growing number of countries exploring ChiPACC Partnering for Success
 waiver California waiver approved New York waiver approved North Dakota waiver approved Additional states exploring A growing number of countries exploring ChiPACC Partnering for Success.")
17
“I am approving this new Medicaid program in Florida because I believe we must do everything possible to lighten the heavy burden on families of children... This is a step beyond traditional hospice rules, and the right thing to do for these most vulnerable children and their families” The Honorable Mike Leavitt, Secretary U.S. Dept. of Health & Human Services* July, 2005 (*Minister of Health) ChiPACC Support from HHS
 ChiPACC Support from HHS.")
18
ChiPACC In the Future NEXT STEPS FOR ChiPACC: Ongoing Technical Assistance Evaluation Quality Assurance Research Legislation

19
Progress PROGRESS to date includes: CMS expanded policy for ChiPACC ChiPACC Bill introduced Concurrent Care Health Reform Provision ChiPACC Bill (revised) re-introduced
 re-introduced")
20
ChiPACC Bill

21
Children’s Program of All-inclusive Coordinated Care “Mattie & Melinda Bill” Reintroduced January 27, 2009, U.S. Congress Congressmen Jim Moran (D VA) & Bill Young (R FL) -One sentence included in 2010 Healthcare Reform Bill- Provision for concurrent care Revised Bill re-introduced 2014
 & Bill Young (R FL) -One sentence included in 2010 Healthcare Reform Bill- Provision for concurrent care Revised Bill re-introduced")
22
Mattie & Melinda Mattie StephanicMelinda Lawrence

23
ChiPACC Overview of the Bill ChiPACC “Mattie & Melinda” Bill Ultimately serving 1.2 million children and families in U.S.A. (many more worldwide) The ChiPACC Bill: Based on the collaborative model of care developed by CHI, the Children's Program of All-inclusive, Coordinated Care (ChiPACC) which provides each enrolled child an individualized treatment plan that includes and manages services from providers across the health care spectrum. ChiPACC: Services will improve upon the often inconsistent care that is currently available to seriously ill children under Medicaid, doing so at a savings to taxpayers. ChiPACC: Goes beyond hospice and palliative care – while incorporating these critical components ChiPACC: Exceeds IOM 2002 Report recommendations for children’s palliative care ChiPACC: Cost effective!
 The ChiPACC Bill: Based on the collaborative model of care developed by CHI, the Children s Program of All-inclusive, Coordinated Care (ChiPACC) which provides each enrolled child an individualized treatment plan that includes and manages services from providers across the health care spectrum. ChiPACC: Services will improve upon the often inconsistent care that is currently available to seriously ill children under Medicaid, doing so at a savings to taxpayers. ChiPACC: Goes beyond hospice and palliative care – while incorporating these critical components ChiPACC: Exceeds IOM 2002 Report recommendations for children’s palliative care ChiPACC: Cost effective!.")
24
ChiPACC Its Many Benefits ChiPACC benefits everyone! In addition to saving taxpayers money, ChiPACC benefits: Child & Family: Increased quality of care Healthcare Providers: Reimbursed for ChiPACC services Healthcare Programs & Institutions: Reimbursed for ChiPACC services Society: ChiPACC is preventive medicine, decreasing dysfunction within the family and society, and allowing families to continue productive lives in their communities

27
On Being a Champion A champion is a winner, A hero… Someone who never gives up Even when the going gets rough, A Champion is a member of A winning team… Someone who overcomes challenges Even when it requires creative solutions. A champion is an optimist, A hopeful spirit… Someone who plays the game, Even when the game is called life… Especially when the game is called life. There can be a champion in each of us, If we live as a winner, If we live as a member of the team, If we live with a hopeful spirit, For life. Mattie J.T. Stepanek, September 1999

28
CHI Information Children’s Hospice International For information: Web: www.CHIonline.org Email: Info@CHIonline.org

30
CMS Participation 2014 CHI TA Webinar Melissa Harris, Director Division of Benefits and Coverage Disabled and Elderly Health Programs Group

31
Florida’s Pediatric Palliative Care Program Partners in Care: Together for Kids

32
Department of Health, Children’s Medical Services (CMS) Florida Hospices Agency for Health Care Administration PARTNERS
 Florida Hospices Agency for Health Care Administration PARTNERS")
33
Partners in Care: Together for Kids Support Counseling Pain and Symptom Management Specialize d Nursing SERVICE S Specialized Personal Care Activity Therapies Respite

34
Map of Florida PIC:TFK Providers

35
Partners in Care: Together for Kids DEVELOPMENT PHASE 2001-2003 Implementation Guidelines Billing codes Partnerships LEGISLATIVE PHASE 2004-2005 Title XXI State Plan Amendment 1915(b)(3) CHI PACC Waiver IMPLEMENTATI ON PHASE 2005-2007 7 sites EXPANSION PHASE 2009-Present 14 sites, covering 54 of the 67 Florida Counties
(3) CHI PACC Waiver IMPLEMENTATI ON PHASE sites EXPANSION PHASE 2009-Present 14 sites, covering 54 of the 67 Florida Counties")
36
Partners in Care: Together for Kids Transition Phase –On January 1, 2014, the Partners in Care: Together for Kids Program transitioned from the 1915(b) waiver to the 1115 waiver. –On August 1, 2014, the Children’s Medical Services (CMS) Network will be a statewide plan for Florida Medicaid under Medicaid Managed Assistance (MMA) and the services of the Partners in Care: Together for Kids will continue to be provided to eligible children enrolled in the CMS Network. –The Program will continue to operate as it does today.
 Network will be a statewide plan for Florida Medicaid under Medicaid Managed Assistance (MMA) and the services of the Partners in Care: Together for Kids will continue to be provided to eligible children enrolled in the CMS Network. –The Program will continue to operate as it does today..")
37
Partners in Care: Together for Kids

38
Total clients receiving PIC:TFK Services: 723 Total amount of claims paid: $681,335.33 Average cost per client: $942.37 *Data for the CY 2013

39
Partners in Care: Together for Kids Data Limitations -Only reflects Title XIX (Medicaid) clients -With the National Correct Coding Initiative, implemented by the Centers for Medicare and Medicaid Services, there are outstanding claims for both the Support Counseling Services and Nursing Services
 clients -With the National Correct Coding Initiative, implemented by the Centers for Medicare and Medicaid Services, there are outstanding claims for both the Support Counseling Services and Nursing Services")
40
Partners in Care: Together for Kids Program Contacts Dusty Edwards, RN, BSN Department of Health, Children’s Medical Services Dusty.Edwards@flhealth.gov Claire Anthony-Davis, RN Florida Agency for Health Care Administration Claire.Davis@ahca.myflorida.com

41
Brian Greffe, M.D. Professor of Pediatrics University of Colorado Denver SOM Medical Director, The Butterfly Program April 16th, 2014 COLORADO CHI PACC WAIVER UPDATE

42
PRESENTATION OUTLINE Timeline – Colorado 1915c CHI PACC Waiver Overview of the Waiver Past, Present, and Future

43
COLORADO CHI PACC WAIVER TIMELINE The Butterfly Program accepts its first patient 1999 (Jun) 2001 The Butterfly Program awarded demonstration project grant from CHI Open Dialogue with the Dept of Health Care Policy and Financing (CO Medicaid) on working towards crafting a 1915c waiver based on CHI-PACC standards 2002 2003 Legislation required for drafting of a new Medicaid waiver; fiscal analysis indicates waiver could save Medicaid $20,000/year/child based on avoidance of unnecessary ER visits and hospitalizations Senate Bill 206 signed into law by Governor Bill Owens 2004 (Jun) 2004 - 2006 (Mar) Focus groups convened to determine waiver services; drafting of waiver Waiver submitted to CMS 2006 (Mar) 2007 (Jan) Waiver approved by CMS authorizing 200 patient slots Final approval of rule (waiver) by Medical Services Board 2007 (Dec) 2008 Waiver implemen- tation; first patient-2/2008 Legislative Audit Committee requests State Auditor to run audit of waiver due to specific concerns of stakeholders 2010 2010 - 2013 Audit findings and recommendation reviewed; periodic meetings with stakeholders to work on recommended changes Joint Budget Committee approves reimbursment rate increase for waiver services: passed in House and awaiting Senate approval 2014 2014 (Jul 1) Implementation of recommended changes based on audit findings
 2001 The Butterfly Program awarded demonstration project grant from CHI Open Dialogue with the Dept of Health Care Policy and Financing (CO Medicaid) on working towards crafting a 1915c waiver based on CHI-PACC standards Legislation required for drafting of a new Medicaid waiver; fiscal analysis indicates waiver could save Medicaid $20,000/year/child based on avoidance of unnecessary ER visits and hospitalizations Senate Bill 206 signed into law by Governor Bill Owens 2004 (Jun) (Mar) Focus groups convened to determine waiver services; drafting of waiver Waiver submitted to CMS 2006 (Mar) 2007 (Jan) Waiver approved by CMS authorizing 200 patient slots Final approval of rule (waiver) by Medical Services Board 2007 (Dec) 2008 Waiver implemen- tation; first patient-2/2008 Legislative Audit Committee requests State Auditor to run audit of waiver due to specific concerns of stakeholders Audit findings and recommendation reviewed; periodic meetings with stakeholders to work on recommended changes Joint Budget Committee approves reimbursment rate increase for waiver services: passed in House and awaiting Senate approval (Jul 1) Implementation of recommended changes based on audit findings")
44
Waiver Name Change Legislation passed indicated that waiver would be called “Pediatric Hospice Waiver” even though model of care in waiver follows CHI PACC principles Waiver program named HOPEFuL shortly after implementation Healing Opportunities, Palliative care, Encouragement For Living for you Waiver is currently named “Children with Life-Limiting Illness” (CLLI) waiver Important to market program as one of “supportive” care avoiding use of terms “hospice” and “palliative”
 waiver Important to market program as one of supportive care avoiding use of terms hospice and palliative")
45
Waiver Audit 2010 – Legislative Audit Committee request State Auditor to run an audit of the waiver given specific concerns of stakeholders Findings of the audit included Waiver services were poorly defined An inadequate number of providers were participating in the program Rates for services under the program were not in line with industry standards leading to low provider enrollment Monthly meetings set up with stakeholders and Colorado Medicaid as a result of findings in order to resolve above issues

46
Current Waiver Stats Currently 197 children enrolled as of 4/7/14 200 slots available Waiver has serviced 256 children since implementation Very slow enrollment following implementation Data for clients who had had claims Client will not show up if provider did not bill for service Number may also be lower than expected due to provider capacity issue

47
Home and Community Based Services (HCBS) CLLI Waiver Domain Changes
 CLLI Waiver Domain Changes")
48
Palliative Care Scope narrowed Pain and symptom management Agency RN with EOL care experience +/- ELNEC training Home Health Agency Hospice Care Coordination Goal to help families in coordinating the complicated medical care often required by these children Agency RN, Home Health Agency, Hospice, Agency Medical MSW

49
Therapeutic Life-Limiting Illness Support Grief /loss or anticipatory grief counseling/support Change will allow providers to provide all encompassing support To involve both patient and family Providers LCSW Licensed Professional Counselor LSW Licensed psychologist Non-denominational chaplain/spiritual care counselor State plan services will be utilized prior to waiver services when available and appropriate

50
Expressive Therapy Provision of creative art, music or play therapy which gives the children to creatively and kinesthetically express their medical situation Provider qualifications for music therapist update Providers Art/Play Therapies Providers who meet requirements for Therapeutic Life Limiting Illness Support with a minimum of one year experience in the provision of art or play therapy to children and adolecscents Degree in music therapy (BA, MA, PhD) plus certification
 plus certification")
51
Complementary Therapies Massage is the only complementary therapy waiver benefit Limited to 24 hours a year Not included as waiver benefits Acupuncture Aromatherapy

52
Respite Care 3 types of respite care To be provided in the home of an eligible client on a short term basis, not to exceed 30 days per annual certification based on date of entry into the program Providers Skilled nursing Home health aide Personal care Provider to be from qualified Medicaid home health, hospice, or personal care agency

53
Bereavement Waiver benefit when hospice has not been elected Care coordinator discusses this option with family prior to the death of the child Service is billed and paid as a lump sum to hospice agency prior to the death of the child if family opts for bereavement Bereavement services available up to one year following the death of the child

54
Dietary and Nutritional Support No longer going to be added as a waiver benefit effective 1/1/14 Part of state plan benefit

55
Summary of HCBS CLLI Waiver Benefits Palliative Care Pain and symptom management Care Coordination Therapeutic Life Limiting Illness Support Counseling Expressive Therapies Art, Music, Play therapies Complementary Therapy Massage Respite Care Bereavement All clients eligible for all other Medicaid state plan benefits including hospice and home health

56
Cost Containment/Effectiveness Preliminary cost data from fiscal 2012-2013 indicates the waiver is cost effective Average per capita cost with state plan services - $61,808 Institutional cost per capita - $100, 773 Waiver is up for renewal by CMS in 2015

57
Brian Greffe, MD – Brian.Greffe@childrenscolorado.org Brian.Greffe@childrenscolorado.org Candace Bailey – Candace.Bailey@state.co.usCandace.Bailey@state.co.us

59
California’s Pediatric Palliative Care Waiver Program Department of Health Care Services Jill Abramson, MD,MPH April 16, 2014

60
Overview Services Updates Issues Next Steps Outline

61
Overview: Partners for Children 1915(c) Home and Community-Based Waiver Provides home-based, family-centered, coordinated palliative care to children with life-limiting conditions Enabling legislation: The Nick Snow Children’s Hospice and Palliative Care Act of 2006 (Bill number AB 1745) Program summary: eligible children identified, enrolled by county nurse, referred to hospice or home health agency that provides waiver services Pilot ran from April 2009 through March 2012 The waiver has been renewed through March 2017 *
 Home and Community-Based Waiver Provides home-based, family-centered, coordinated palliative care to children with life-limiting conditions Enabling legislation: The Nick Snow Children’s Hospice and Palliative Care Act of 2006 (Bill number AB 1745) Program summary: eligible children identified, enrolled by county nurse, referred to hospice or home health agency that provides waiver services Pilot ran from April 2009 through March 2012 The waiver has been renewed through March 2017 *")
62
Finds/enrolls client Connects client with agency Reviews care plan Authorizes services Provides local oversight Care Coordinator At HHA or HA Meets with family to develop care plan and coordinate services Coordinates waiver and community services Meets with family and CCSNL bimonthly Supports client in multiple settings CCSNL

63
Care coordination (RN + SW) Massage/ art/ music Respite Pain/Symptom management Family Counseling/bereavement PFC Services
 Massage/ art/ music Respite Pain/Symptom management Family Counseling/bereavement PFC Services")
64
Number, age demographics of enrolled Since waiver inception: 206 Current enrollment: 86 Average time in program: approx. 12 months Medical conditions neoplasm, muscular dystrophy, cystic fibrosis, cerebral palsy, metabolic disorder County of residence include Los Angeles, Orange, Monterey, Sonoma, Santa Cruz + Race/ethnicity 70% Latino/Hispanic, then Caucasian, Asian, Black Age -1 year through 20 years Enrollment

65
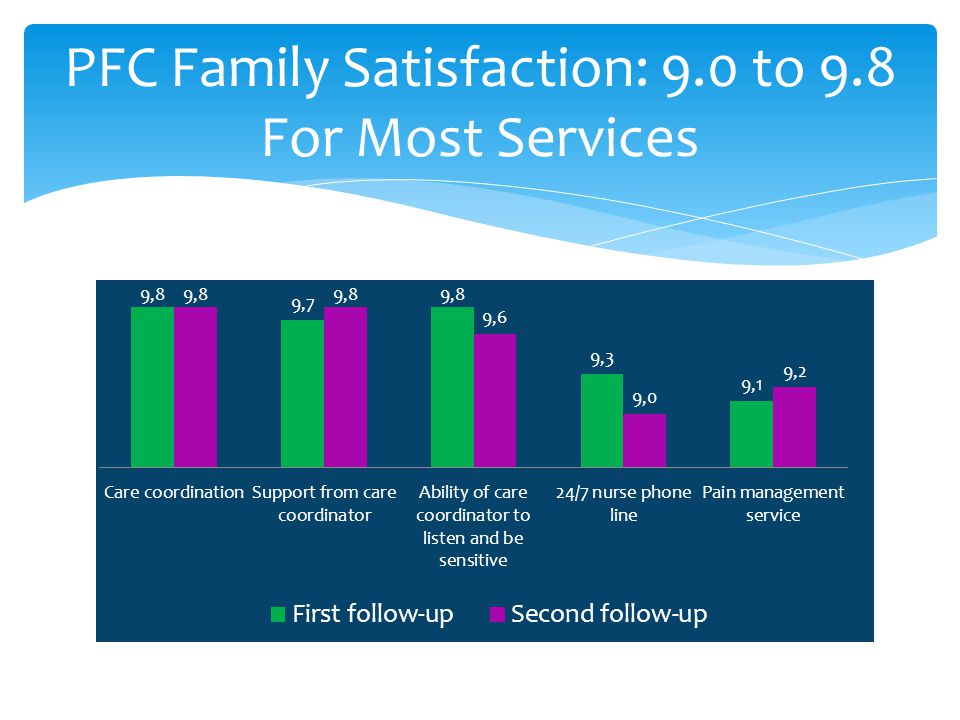
UCLA Center for Health Policy Final evaluation in progress Satisfaction surveys – families, agencies, CCSNLs – very positive feedback Cost evaluation – preliminary findings suggest significant savings PFC evaluation

66
PFC Family Satisfaction: 9.0 to 9.8 For Most Services

68
PFC evaluation – $2848 pmpm cost savings Note: Change in ER costs was low and was omitted Source: UCLA analysis of PFC enrollees’ claims data

69
Claims – resolving Managed Care and OHC - resolving Long referral process – partnering with referring inpatient pediatric palliative care team to shorten Home health and hospice agency buy in Current reimbursement not sustainable for agencies – restructure rates? Updates

70
Modify reimbursement Additional streamlining Consider expanding to additional counties Survey on what other services may be needed Sharing the PFC experience at Grand Rounds and other meetings to increase referrals Next Steps

71
Jill Abramson, MD, MPH Partners for Children state lead, DHCS Jill.Abramson@dhcs.ca.gov Partners for Children: http://www.dhcs.ca.gov/services/ppc/Pages/default.aspx ccsppc@dhcs.ca.gov ccsppc@dhcs.ca.gov Contacts and Resources

73
To Children’s Hospice and Pediatric Care Coalition for continuing support To Robert Dimand MD, Chief Medical Officer of SCD and to other DHCS staff and County CCS staff who have helped with this waiver program, To Providence Trinity Hospice, Coastal Kids Home Care and Hospice By the Bay who have provided outstanding services despite many reimbursement issues.

74
Children’s Hospice International Redesign Medicaid in New York State Annual Conference/Webinar April 16, 2014

75
State Update: New York Children’s Hospice International Annual Conference/Webinar April 16, 2014

76
State Update: New York Presented by: Liz Morales, Care At Home I/II Program New York State Department of Health Office of Health Insurance Programs Division of Long Term Care Bureau of Home and Community Based Waivers

77
Outline Outline Care at Home (CAH) I/II Waiver CAH I/II Waiver Services
 I/II Waiver CAH I/II Waiver Services")
78
New York’s Approach CAH I/II is a Medicaid waiver for children who are determined physically disabled according to Social Security Administration criteria

79
CAH I/II Program Background The CAH I/II waiver, which has been in existence since 1985, includes five pediatric palliative care services. The waiver renewal in 2009 included many changes, including the addition of three other waiver services. The addition of Medicaid eligible children Levels of Care CAH I: Skilled Nursing Facility CAH II: Hospital

80
Who is eligible for Care at Home? Children who have a Skilled Nursing Facility or Hospital level of care Under 18 years of age Can be cared for at home safely and at no greater cost than in the appropriate facility Child must not be married

81
Who is eligible for Care at Home? Children who are Medicaid eligible when parents’ income and/or resources are counted* - OR - Children who are Medicaid ineligible when parents’ income and/or resources are counted but eligible when parents’ income and resources are not counted *Effective April 15, 2009

82
CAH I/II Waiver Services Case Management Respite Home and Vehicle Modifications Family Palliative Care Education Pain and Symptom Management Bereavement Massage Therapy Expressive Therapy Art Music Play

83
CAH I/II Palliative Care Waiver Providers Services provided by a: Hospice; or Certified Home Health Agency (CHHA)
")
84
Palliative Care Children’s Advisory Group Comprised of hospices, CHHAs and providers of long term care Continues to be a source of information and guidance Served as a resource to assist NYS DOH to: Define service descriptions Define provider credentials Develop provider/program requirements Define continuing education credentials Provide outreach to potential providers

85
Moving Forward Moving Forward Continue to outreach to potential providers. Continue to outreach to potential families whose children may be eligible. Develop educational and outreach materials for families with disabled children.

86
Future Endeavors The renewal application for CAH I/II was submitted to CMS in the Fall 2013. Care At Home waiver staff are in discussion with CMS to finalize and obtain approval Contains no major changes; new Pediatric Assessment tool will be employed (UAS-NY), upon approval from CMS
, upon approval from CMS.")
87
Contacts CAH I/II – DOH State Contact: (518) 474-5271 Liz Morales Care At Home Program I/II EAM04@health.state.ny.us Carol Hodecker CXH09@health.state.ny.us Susan Appleby SXA10@health.state.ny.us Hospice and Palliative Care Children’s Advisory Group Contact: (518) 446-1483 Kathy A. McMahon President and CEO of HPCANY kmcmahon@hpcanys.org

88
Federal Legislative Update on Coordinated Care for Children with Life-Limiting Conditions David Pore and Sara Garofalo Arnold & Porter, LLP April 16, 2014

89
CMS Rule on HCBS Waivers CMS issued a final rule in January 2014, which makes changes to Home and Community Based Services (HCBS). Applicable to waivers 1915(c) : –Allows Secretary to waive certain statutory requirements to let states extend HCBS to certain subgroups of Medicaid participants who qualify for institutional levels of care –Allows states to combine three eligibility groups –Implements requirements for person-centered plans –Defines HCB setting requirements
 : –Allows Secretary to waive certain statutory requirements to let states extend HCBS to certain subgroups of Medicaid participants who qualify for institutional levels of care –Allows states to combine three eligibility groups –Implements requirements for person-centered plans –Defines HCB setting requirements.")
90
ChiPACC Legislation ChiPACC legislation has been introduced in previous sessions of Congress by Rep. Jim Moran (D-VA). –Re-introduction anticipated in spring of 2014. Bill would increase state flexibility and make it easier for states to implement a ChiPACC program as a Medicaid state plan option. –Currently, states must get approval through a complicated and timely waiver process through CMS. –Five states including, California, Colorado, New York, Florida, and North Dakota have programs in operation. –Additional states are in various levels of developing programs.
. –Re-introduction anticipated in spring of Bill would increase state flexibility and make it easier for states to implement a ChiPACC program as a Medicaid state plan option. –Currently, states must get approval through a complicated and timely waiver process through CMS. –Five states including, California, Colorado, New York, Florida, and North Dakota have programs in operation. –Additional states are in various levels of developing programs..")
91
ChiPACC Legislation Bill General Overview: –Provides enrolled children with individualized treatment plan that does not limit scope, amount, or duration of care for eligible services. –Eligible services include acute, long term care, palliative care, respite, curative treatment and counseling support services to individual and family members. –Coordinated care improves access to community- based care to avoid costly hospitalizations. –Service delivery system would be cost neutral to the Medicaid program.

92
Legislative Outlook in 2014 Working with key members of House Energy and Commerce Committee, Congressional caucuses on potential avenues for including ChiPACC language in upcoming legislative vehicles: –SCHIP reauthorization; Medicaid overhaul legislation; complex children’s hospital legislation (Reps. Barton/Castor). –Positioning ChiPACC program as a cost-saving option which can be used as an offset in other must-pass legislation. Educating members and staff on states’ waivers savings. Developing new ChiPACC champions in Congress and outreach to natural allies engaged in pediatric healthcare issues. Working to identify and utilize ChiPACC’s existing partnerships to leverage support for ChiPACC program with key members of Congress.
. –Positioning ChiPACC program as a cost-saving option which can be used as an offset in other must-pass legislation. Educating members and staff on states’ waivers savings. Developing new ChiPACC champions in Congress and outreach to natural allies engaged in pediatric healthcare issues. Working to identify and utilize ChiPACC’s existing partnerships to leverage support for ChiPACC program with key members of Congress..")
93
© Children’s Hospice International Children’s Hospice International 13th Annual ChiPACC Conference With technical assistance from Centers for Medicare & Medicaid Services DISCUSSION MELISSA HARRIS Facilitator

94
ChiPACC Contacts For additional Information please contact: CMS : Melissa.Harris@cms.hhs.gov CHI: armstrongdailey@chionline.org John.Gould@APORTER.COM Mahnu.Davar@APORTER.COM David.Pore@APORTER.COM

Similar presentations
















>")





 Sustainability for Early Childhood Systems Building.>")


