Download presentation
Presentation is loading. Please wait.

1
Airway Management's Dirty Laundry – Lessons From The NAP4 Study D. John Doyle MD PhD Cleveland Clinic

2
Dr D John Doyle Professor of Anesthesiology Cleveland Clinic, Cleveland, Ohio MDUniversity of Toronto, 1982 PhDUniversity of Toronto, 1986 BoardedRoyal College of Physicians, Canada, 1986 BoardedAmerican Board of Anesthesiology, 1989 University of Toronto / Toronto General Hospital 1987 to 2001 Case Western Reserve University / Cleveland Clinic 2002 to present Past President: Society for Airway Management Society for Technology in Anesthesia

7
Transtracheal Injection of Local Anesthestic Through an IV Catheter

8
NO CONFLICTS OF INTEREST

9
Cambridge University Press 2012

10
4th National Audit Project of the Royal College of Anaesthetists (NAP4) Major complications of airway management in the UK March 2011 http://www.rcoa.ac.uk/nap4
 Major complications of airway management in the UK March")
11
A valuable educational resource, full of valuable lessons 24 chapters, 5 appendices Free download: http://www.rcoa.ac.uk/nap4 http://www.rcoa.ac.uk/nap4

12
Easy to read, engaging style Captured the interest of anesthesiologists around the world Many cautionary tales

15
The National Audit Project 4 was initiated jointly by the Difficult Airway Society and the Royal College of Anesthetists to investigate airway management in the UK. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

16
The investigators collected airway complication data arising in ORs, ICUs & EDs from all NHS hospitals over a 1 year period. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

17
The endpoints were: death, permanent disability such as brain damage; an unplanned surgical airway; or an unanticipated admission to ICU/ prolongation of ICU stay. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch
18
A census of all clinical activity over 2 weeks was carried to estimate denominator and incidence figures. There were 133 reports of serious airway complications relating to general anesthesia, giving an incidence of 1:22,000. There were 16 anesthesia deaths and 3 episodes of permanent brain damage, resulting in an anesthesia airway-related mortality rate of 1:180,000. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

20
Approximately 42% of anesthesia events reported had a primary airway event indicating intubation difficulty that was ultimately responsible for 13% of airway related mortality. The majority of the events occurred in straightforward elective surgery in ASA I-II male patients aged <60. A potential practice inadequacy identified was that a formal airway assessment was recorded in only 35 of 133 cases (26%). http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch
.")
21
Aspiration was the single most common primary cause of mortality (rather than cerebral hypoxia per se), and notably, aspiration occurred as frequently using a supraglottic airway as during the use of a tracheal tube. Aspiration accounted for 8 anesthesia deaths and two cases of brain damage.

22
Nearly 50% of the events followed head & neck surgery. Approximately 70% of these reports were associated with obstructive lesions within the airway & reports indicated evidence of poor anticipation and planning for management of airway instrumentation & extubation. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

23
Obese patients were disproportionately represented, presenting twice as frequently in the population that suffered incidents than in the group that did not. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

24
Use of a needle cricothyroidotomy as a rescue technique suffered a 65% failure rate with numerous mechanisms of failure cited including: equipment, training, insertion technique and ventilation technique. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch
25
An emergency surgical airway was necessary in 43% of anesthesia cases…most surgical airways were undertaken by surgeons. One quarter of events involved emergence … usually resulting in airway obstruction from laryngospasm, biting on the airway device or airway swelling. Reviewers found that elements of poor management were observed in the majority of cases. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

26
At least 1 in 4 major airway events were from ICU or ED. A consultant was usually present for the in-theatre events, in contrast to the ICU and ED events, where junior staff were more frequently present. The severity of ICU and ED events was greater, with death and brain damage a more frequent outcome. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

27
Displacement of tracheostomies caused 50% of ICU events. The majority of events in ED concerned difficult or failed tracheal intubation during RSI. In ICU/ED, capnography was often not used or was misinterpreted (especially during cardiac arrest) and was a contributory factor in 73% of deaths or neurological injury, usually due to unrecognised oesophageal intubation. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch
 and was a contributory factor in 73% of deaths or neurological injury, usually due to unrecognised oesophageal intubation.")
28
The executive summary suggests that when potential difficulty with airway management is identified, rather than an airway plan, a strategy is required. An airway plan suggests a single approach to management whereas a strategy is a co-ordinated, logical sequence of plans which includes a back-up plan & rescue techniques i.e., forward planning for initial failure. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

29
Of note, events were reported when supraglottic airway devices were used inappropriately, and supraglottic airways were used to avoid tracheal intubation in some patients with a recognised difficult airway without evidence of a back-up plan. Also, the project identified numerous cases where AFOI was indicated but not used. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

30
The authors suggest that choosing the safest technique for airway management may not necessarily be the anaesthetist’s most familiar and it may be necessary to seek the assistance of colleagues with specific skills. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

31
The authors also suggest that obesity needs to be recognized as a risk factor for airway difficulty and strategies modified accordingly. http://www.anaesthesiacases.com.au/cpd/dr_maryannes_journal_watch/may_2011_journal_watch

33
An Important Lesson: It is usually OK to wake up the patient and abort the anesthetic if airway problems are encountered!

38
Some Clinical Themes

45
SAD – supraglottic airway device

46
Some Clinical Themes

56
Possible Lessons for American Anesthesia

57
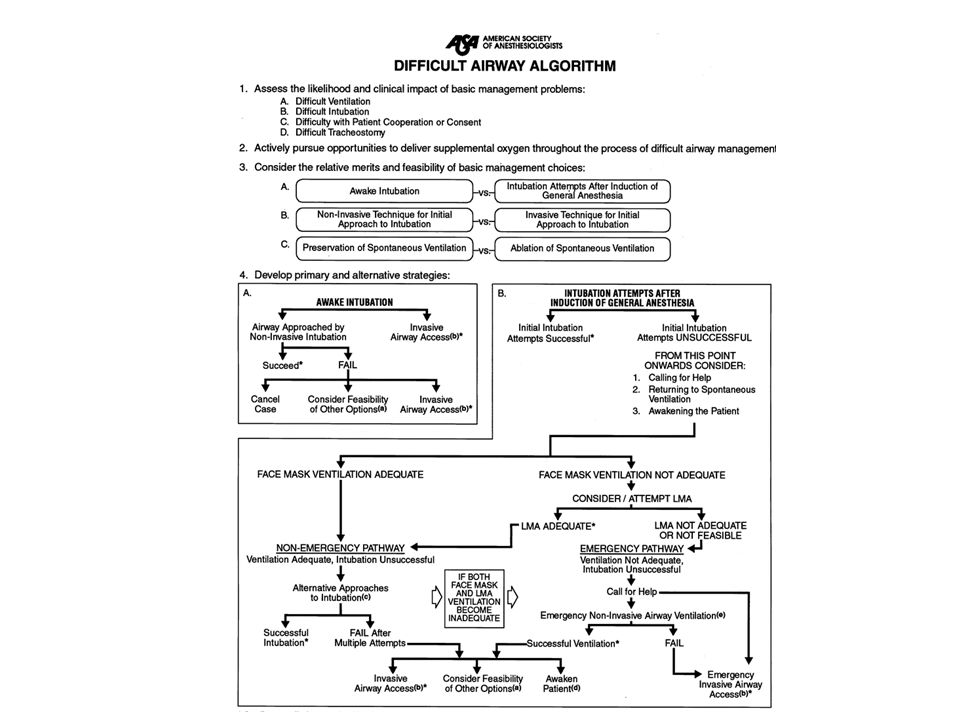
ASA DAA

58
Table 1. Components of the Preoperative Airway Physical Examination. This table displays some findings of the airway physical examination that may suggest the presence of a difficult intubation.

63
Healy DW, Maties O, Hovord D, Kheterpal S. A systematic review of the role of videolaryngoscopy in successful orotracheal intubation. BMC Anesthesiol. 2012 Dec 14;12:32. doi: 10.1186/1471-2253-12-32. PubMed PMID: 23241277; PubMed Central PMCID: PMC3562270.

64
Regular Videolaryngoscopes GlideScope family McGrath products Storz products AP Advance CoPilot VL Truphatek

65
Two Cheap, Useful, Life-Saving Gadgets Airway Introducers (bougies) Airway Exchange Catheters
 Airway Exchange Catheters")
66
Intubation Bougies

67
Cormack-Lehane Grading System Grade I: most of glottis is seen Grade II: only posterior portion of glottis can be seen (May not be ASA Task Force "difficult" if some part of the vocal cords are seen.) Grade III: only epiglottis may be seen (none of glottis seen)(ASA Task Force "difficult.") Grade IV: neither epiglottis nor glottis can be seen (ASA Task Force "difficult.")
 Grade III: only epiglottis may be seen (none of glottis seen)(ASA Task Force difficult. ) Grade IV: neither epiglottis nor glottis can be seen (ASA Task Force difficult. )")
68
The Eschmann Bougie is a yellow colored, 60 cm, 15 French, stiff stylet marketed by Portex as Catalog Number 103014 and manufactured in England by Eschmann Health Care. It is fabricated from a braided polyester base with a resin coating. It costs around $75 each and can be reused.

71
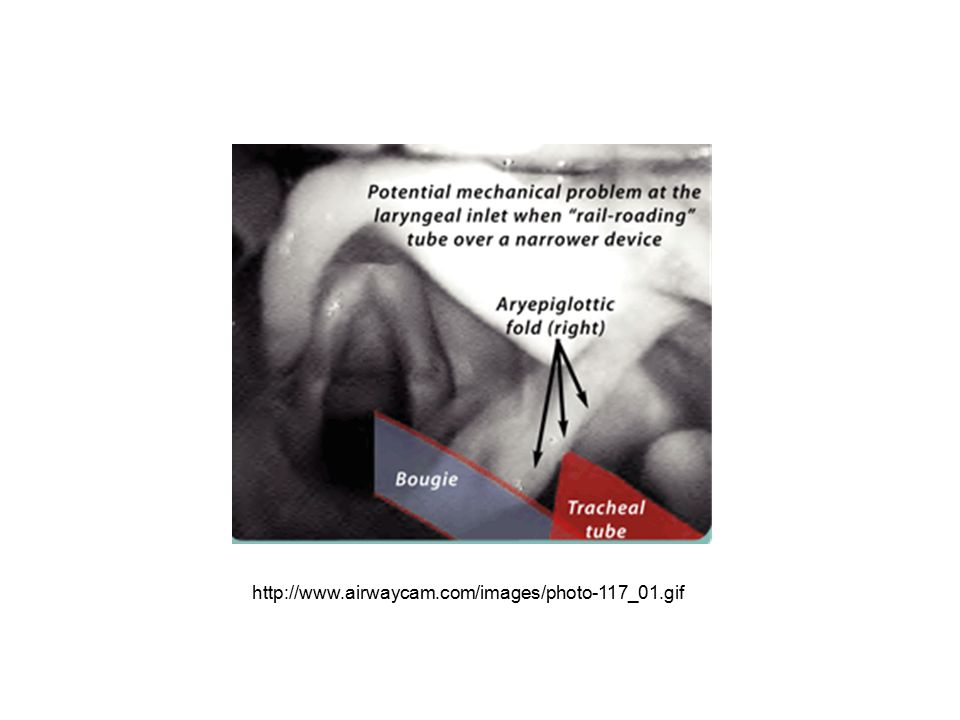
Eschmann Bougie I have found this stylet to be invaluable when faced with a difficult intubation. The technique is simple. If the tip of the epiglottis is visible, slide the upward angled end of the bougie along the bottom of the epiglottis, feeling gently for the unseen glottic opening. It is unlikely that the bougie will be directed into the more posterior esophagus if care is taken to maintain contact with the bottom of the epiglottis. Once the tip is thought to be through the cords, continue to push it into the trachea. With experience, a positive confirmation of tracheal placement can be made by feeling the "clicks" as the angled tip of the bougie passes over the tracheal rings. A 6 or 7 mm endotracheal tube is then passed over the stylet (the modified Seldinger technique for intubation). If the tube hangs up at the cords, simple twisting of the tube will usually allow it to pass. http://www.calsocanes.com/Bulletins/vol%2047-4/tips984.pdf http://www.accessem.com/loadBinary.aspx?fileNa me=knoo3_c022f021t.jpg http://bay- medical.com/media/catalo g/product/cache/1/image/3 00x/9df78eab33525d08d6 e5fb8d27136e95/9/-/9- 0208-xx_16.jpg
. If the tube hangs up at the cords, simple twisting of the tube will usually allow it to pass. fileNa me=knoo3_c022f021t.jpg medical.com/media/catalo g/product/cache/1/image/3 00x/9df78eab33525d08d6 e5fb8d27136e95/9/-/ xx_16.jpg.")
72
http://www.airwaycam.com/images/photo-117_01.gif
73
Airway Exchange Catheters

78
A patient who underwent maxillofacial surgery due to trauma. She was extubated with the use of the pediatric airway exchange catheter (PAEC), and required reintubation after 6 hours of extubation. This was easily achieved over the PAEC without cutting the archbar. Dosemeci et al. Critical Care 2004 8:R385
, and required reintubation after 6 hours of extubation. This was easily achieved over the PAEC without cutting the archbar. Dosemeci et al. Critical Care :R385.")
79
AEC, airway exchange catheter; NaCl, 0.9% saline; NPPV, non- invasive positive pressure ventilation; PES, post- extubation stridor. http://ccforum.com/content/fig ures/cc8142-3-l.jpg

80
The End

Similar presentations





































 Facemasks: Intersurgical sizes 0 and 1 Laerdal sizes 0 and 1 (re-usable) Oropharyngeal Airway (sizes 000, 00 and 0) ETT.>")











