Download presentation
Presentation is loading. Please wait.

1
Dallas 2015 TFQO: Jerry Nolan #310 EVREV 1: Jerry Nolan COI #301 EVREV 2: Charles Deakin COI #221 Taskforce: ALS ALS 714 : Advanced airway placement (SGA vs TT)
")
2
Dallas 2015 COI Disclosure (SPECIFIC to this systematic review) Jerry Nolan COI #310 Commercial/industry Editor-in-Chief Resuscitation Potential intellectual conflicts Co-applicant AIRWAYS-2 (igel versus intubation) NIHR Funded Charles Deakin COI #221 Commercial/industry Editorial Board, Resuscitation Director, Prometheus Medical Potential intellectual conflicts TMG, AIRWAYS-2 (igel versus intubation) NIHR Funded
 Jerry Nolan COI #310 Commercial/industry Editor-in-Chief Resuscitation Potential intellectual conflicts Co-applicant AIRWAYS-2 (igel versus intubation) NIHR Funded Charles Deakin COI #221 Commercial/industry Editorial Board, Resuscitation Director, Prometheus Medical Potential intellectual conflicts TMG, AIRWAYS-2 (igel versus intubation) NIHR Funded")
3
Dallas 2015 2010 TR Healthcare professionals trained to use supraglottic airway devices may consider their use for airway management during cardiac arrest and as a backup or rescue airway in a difficult or failed tracheal intubation.

4
Dallas 2015 C2015 PICO Population: patients in cardiac arrest in any setting Intervention: Insertion of supraglottic airway as first advanced airway Comparison: Tracheal intubation as first advanced airway Outcomes: Survival with Favorable neurological/functional outcome at discharge, 30 days, 60 days, 180 days AND/OR 1 year (9-Critical) Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year (8-Critical) Change ROSC, CPR parameters, aspiration pneumonia
 Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year (8-Critical) Change ROSC, CPR parameters, aspiration pneumonia")
5
Dallas 2015 Inclusion/Exclusion & Articles Found The search yielded a total of 369 studies. Of these, 2 RCTs and 15 observational studies were included for bias assessment. 4 studies excluded after bias assessment because they reported only blood gas data

6
Dallas 2015 Risk of Bias in RCTs

7
Dallas 2015 Risk of Bias in non-RCTs

11
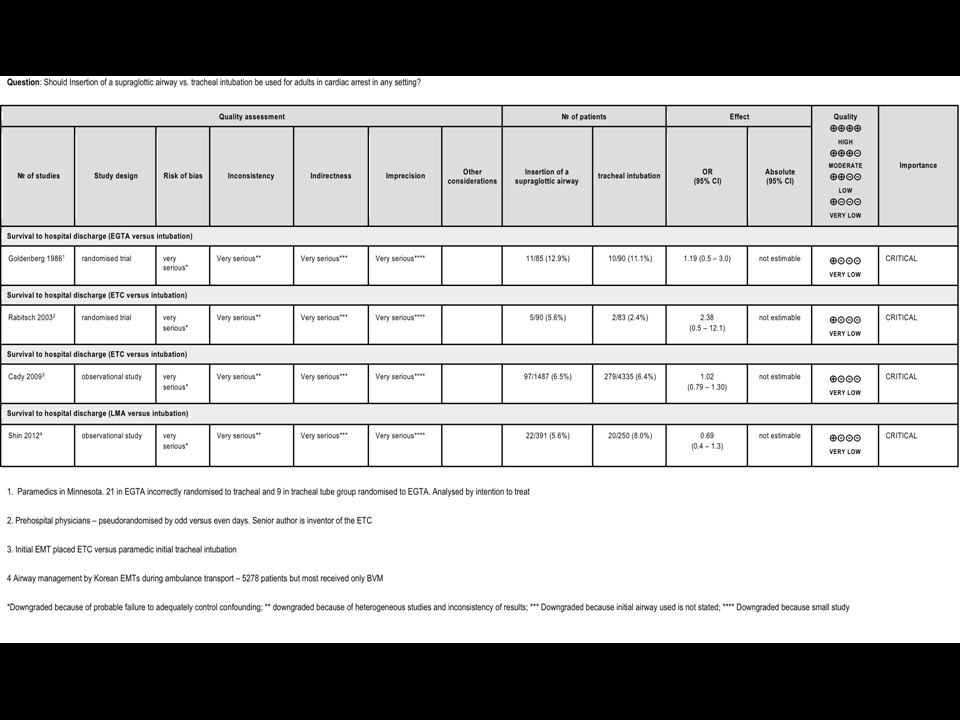
Dallas 2015 Proposed Consensus on Science statements EGTA (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence (downgraded for very serious concerns about risk of bias and imprecision) from one RCT enrolling 175 OHCAs show no difference between EGTA and tracheal intubation (OR 1.19 95% CI 0.5 - 3.0) [Goldenberg 1986 90] Combitube (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence (downgraded for very serious concerns about risk of bias and imprecision) from one RCT enrolling 173 OHCAs that showed no difference between Combitube and tracheal intubation (OR 2.38 95% CI 0.5 – 12.1) [Rabitsch 2003 27] and very low quality evidence from one observational study of 5822 OHCAs that showed no difference between tracheal intubation by paramedics and Combitube insertion by emergency medical technicians (EMTs) (adjusted OR 1.02; 95% CI 0.79 -1.30) [Cady 2009 495]. For the important outcome of ROSC we have identified very low quality evidence from one observational study of 5822 OHCAs that showed no difference between tracheal intubation by paramedics and Combitube insertion by emergency medical technicians (EMTs) (adjusted OR 0.93; 95% CI 0.82 -1.05). [Cady 2009 495].
![Dallas 2015 Proposed Consensus on Science statements EGTA (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence (downgraded for very serious concerns about risk of bias and imprecision) from one RCT enrolling 175 OHCAs show no difference between EGTA and tracheal intubation (OR % CI ) [Goldenberg ] Combitube (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence (downgraded for very serious concerns about risk of bias and imprecision) from one RCT enrolling 173 OHCAs that showed no difference between Combitube and tracheal intubation (OR % CI 0.5 – 12.1) [Rabitsch ] and very low quality evidence from one observational study of 5822 OHCAs that showed no difference between tracheal intubation by paramedics and Combitube insertion by emergency medical technicians (EMTs) (adjusted OR 1.02; 95% CI ) [Cady ].](http://images.slideplayer.com/16/5257432/slides/slide_11.jpg "For the important outcome of ROSC we have identified very low quality evidence from one observational study of 5822 OHCAs that showed no difference between tracheal intubation by paramedics and Combitube insertion by emergency medical technicians (EMTs) (adjusted OR 0.93; 95% CI ). [Cady ]..")
12
Dallas 2015 Proposed Consensus on Science statements LMA (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence from one observational study of 641 OHCAs that showed lower rates of survival to hospital discharge with insertion of an LMA compared with tracheal tube (OR 0.69; 95% CI 0.4 – 1.3) [Shin 2012 313] Supraglottic airways (SGAs: Combitube, LMA, laryngeal tube) versus tracheal intubation For the critical outcome of favourable neurological survival we have identified low quality evidence from one observational study of 5377 OHCAs showing no difference between tracheal intubation and insertion of a SGA (adjusted OR 0.71; 95% CI 0.39 – 1.30) [Kajino 2011 R236], from one observational study of 281,522 OHCAs showing higher rates of favourable neurological outcome between insertion of a SGA and tracheal intubation (OR 1.11; 95% CI 1.0 – 1.2) [Hasegawa 2013 257] and from two studies showing higher rates of favourable neurological outcome between tracheal intubation and insertion of a SGA (8701 OHCAs adjusted OR 1.44; 95% CI 1.10 – 1.88 [McMullan 2014 617]) and (10,455 OHCAs adjusted OR 1.40; 95% CI 1.04 – 1.89 [Wang 2012 1061]).
![Dallas 2015 Proposed Consensus on Science statements LMA (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence from one observational study of 641 OHCAs that showed lower rates of survival to hospital discharge with insertion of an LMA compared with tracheal tube (OR 0.69; 95% CI 0.4 – 1.3) [Shin ] Supraglottic airways (SGAs: Combitube, LMA, laryngeal tube) versus tracheal intubation For the critical outcome of favourable neurological survival we have identified low quality evidence from one observational study of 5377 OHCAs showing no difference between tracheal intubation and insertion of a SGA (adjusted OR 0.71; 95% CI 0.39 – 1.30) [Kajino 2011 R236], from one observational study of 281,522 OHCAs showing higher rates of favourable neurological outcome between insertion of a SGA and tracheal intubation (OR 1.11; 95% CI 1.0 – 1.2) [Hasegawa ] and from two studies showing higher rates of favourable neurological outcome between tracheal intubation and insertion of a SGA (8701 OHCAs adjusted OR 1.44; 95% CI 1.10 – 1.88 [McMullan ]) and (10,455 OHCAs adjusted OR 1.40; 95% CI 1.04 – 1.89 [Wang ]).](http://images.slideplayer.com/16/5257432/slides/slide_12.jpg "Dallas 2015 Proposed Consensus on Science statements LMA (I) versus tracheal intubation (C) For the critical outcome of survival to hospital discharge we have identified very low quality evidence from one observational study of 641 OHCAs that showed lower rates of survival to hospital discharge with insertion of an LMA compared with tracheal tube (OR 0.69; 95% CI 0.4 – 1.3) [Shin ] Supraglottic airways (SGAs: Combitube, LMA, laryngeal tube) versus tracheal intubation For the critical outcome of favourable neurological survival we have identified low quality evidence from one observational study of 5377 OHCAs showing no difference between tracheal intubation and insertion of a SGA (adjusted OR 0.71; 95% CI 0.39 – 1.30) [Kajino 2011 R236], from one observational study of 281,522 OHCAs showing higher rates of favourable neurological outcome between insertion of a SGA and tracheal intubation (OR 1.11; 95% CI 1.0 – 1.2) [Hasegawa ] and from two studies showing higher rates of favourable neurological outcome between tracheal intubation and insertion of a SGA (8701 OHCAs adjusted OR 1.44; 95% CI 1.10 – 1.88 [McMullan ]) and (10,455 OHCAs adjusted OR 1.40; 95% CI 1.04 – 1.89 [Wang ]).")
13
Dallas 2015 Proposed Consensus on Science statements Supraglottic airways (SGAs: Combitube and LMA) versus tracheal intubation For the important outcome of ROSC we have identified very low quality evidence from one observational study of 713 OHCAs that showed no difference between tracheal intubation and Combitube or LMA insertion by EMTs or emergency life-saving technicians (ELTs) (OR 0.65; 95% CI 0.4 – 1.2). [Yanagawa 2010 340].

14
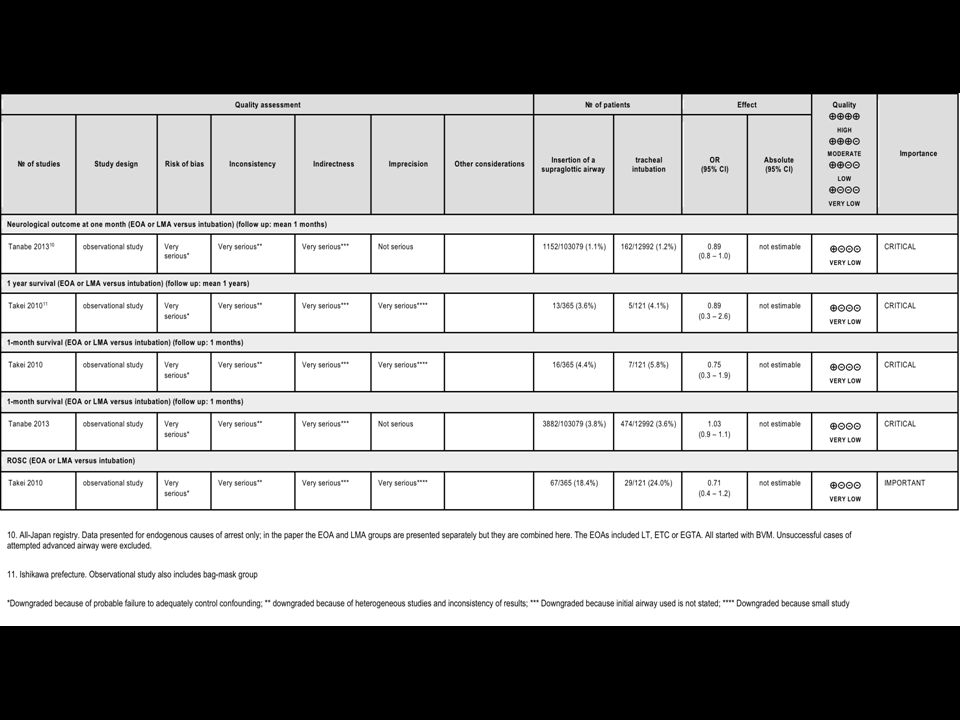
Dallas 2015 Proposed Consensus on Science statements Supraglottic airways (SGAs: Esophageal obturator airway and LMA) versus tracheal intubation For the critical outcome of neurologically favourable one-month survival we have identified very low quality evidence from one observational study of 138,248 OHCAs that showed higher rates of neurologically favourable one-month survival with tracheal intubation compared with insertion of an esophageal obturator airway or LMA (OR 0.89; 95% CI 0.8 – 1.0). [Tanabe 2013 389] For the critical outcome of one-year survival we have identified very low quality evidence from one observational study of 923 OHCAs that showed no difference in one-year survival with tracheal intubation compared with insertion of an esophageal obturator airway or LMA (OR 0.89; 95% CI 0.3 – 2.6). [Takei 2010 715]. For the critical outcome of one-month survival we have identified very low quality evidence from one observation study that showed no difference in one-month survival between tracheal intubation and insertion of an esophageal obturator airway of an LMA (OR 0.75; 95% CI 0.3 – 1.9) [Takei 2010 715] and very low quality evidence from another observation study that showed higher one-month survival with tracheal intubation compared with insertion of an esophageal obturator airway of an LMA (OR 1.03; 95% CI 0.9 – 1.1) [Tanabe 2013 389] For the important outcome of ROSC we have identified very low quality evidence from one observational study of 923 OHCAs that showed a higher rate of ROSC with tracheal intubation compared with insertion of an esophageal obturator airway or LMA (OR 0.71; 95% CI 0.4 – 1.2). [Takei 2010 715].
. [Takei ]. For the critical outcome of one-month survival we have identified very low quality evidence from one observation study that showed no difference in one-month survival between tracheal intubation and insertion of an esophageal obturator airway of an LMA (OR 0.75; 95% CI 0.3 – 1.9) [Takei ] and very low quality evidence from another observation study that showed higher one-month survival with tracheal intubation compared with insertion of an esophageal obturator airway of an LMA (OR 1.03; 95% CI 0.9 – 1.1) [Tanabe ] For the important outcome of ROSC we have identified very low quality evidence from one observational study of 923 OHCAs that showed a higher rate of ROSC with tracheal intubation compared with insertion of an esophageal obturator airway or LMA (OR 0.71; 95% CI 0.4 – 1.2). [Takei ]..")
15
Dallas 2015 Draft Treatment Recommendations We suggest using either a supraglottic airway or tracheal tube as the initial advanced airway management during CPR (weak recommendation, very low quality evidence) for out of hospital cardiac arrest. We suggest using either a supraglottic airway or tracheal tube as the initial advanced airway management during CPR (weak recommendation, very low quality evidence) for in hospital cardiac arrest.
 for in hospital cardiac arrest..")
16
Dallas 2015 Values and preferences The type of airway used may depend on the skills and training of the healthcare provider. Tracheal intubation requires considerably more training and practice. Tracheal intubation may result in unrecognised oesophageal intubation and increased hands off time in comparison with insertion of a supraglottic airway. Both a supraglottic airway and tracheal tube are frequently used in the same patients as part of a stepwise approach to airway management but this has not been formally assessed.

17
Dallas 2015 Next Steps This slide will be completed during Task Force Discussion (not EvRev) and should include: Consideration of interim statement Person responsible Due date
 and should include: Consideration of interim statement Person responsible Due date")
Similar presentations






 EVREV 1: Gene Ong (#COI = 118) EVREV 2: Jos Bruinenberg (#COI = 19) Taskforce: Pediatric Taskforce The Long.>")













