Download presentation
Presentation is loading. Please wait.

1
Radiology of Digestive System
Department of Radiology Zhongshan Hospital, Fudan university RAO Sheng-Xiang

2
Plain film radiograph Hepatic angle Spenic angle Renal shadow
Psoas muscle Properitoneal fat strip

3
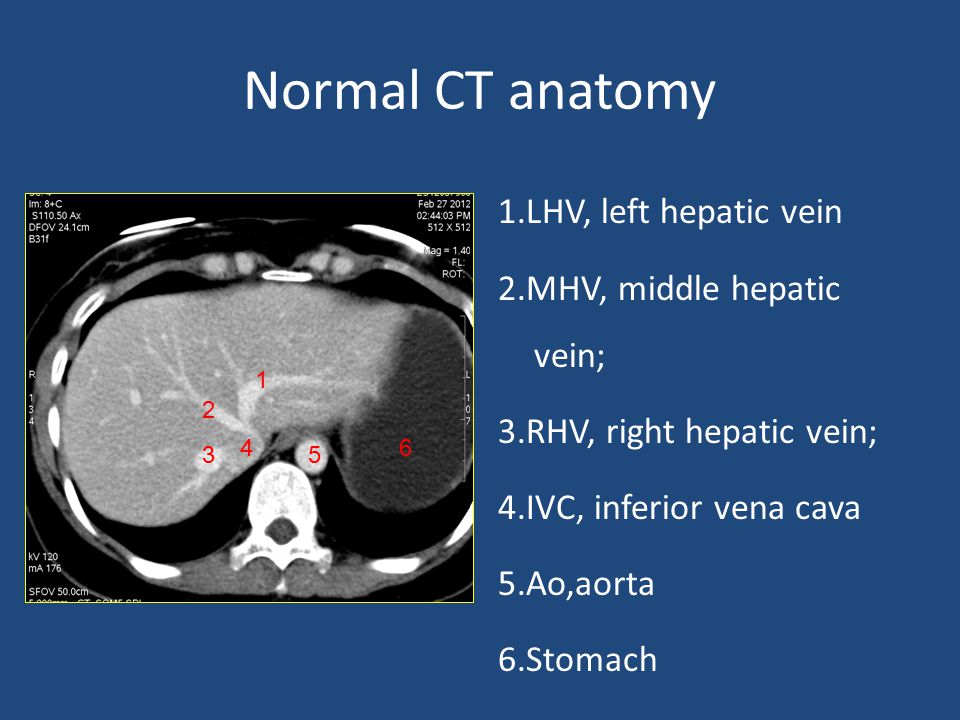
Normal CT anatomy 1.LHV, left hepatic vein 2.MHV, middle hepatic vein; 3.RHV, right hepatic vein; 4.IVC, inferior vena cava 5.Ao,aorta 6.Stomach 1 2 4 6 3 5
4
1.LPV, left portal vein 2.Stomach 3.Speen 4.IVC, inferior vena cava
5.Ao,aorta 1 2 4 5 3

5
1.Gallbladder 2.RPV, right portal vein 3.antrum 4.duodenal bulb 3 1 4

6
1.CA,celiac axis 2.Splenic artery 3.common hepatic artery 4.Duodenum
5.Kidney 6.Pancreas 7.Portal vein 8.Adrenal gland 2 6 7 3 1 4 5 5

7
SMA:superior mesenteric artery
CBD,common bile duct Spenic vein Pancreas

8
SMV, superior mesenteric vein
SMA, superior mesenteric artery Uncinate process

9
CTA SMA, superior mesenteric artery CA,celiac axis Splenic artery
common hepatic artery

10
main portal trunk; right portal branch; splenic vein; inferior mesenteric vein; superior mesenteric vein

11
RHV, right hepatic vein;
MHV, middle hepatic vein; LHV, left hepatic vein IVC, inferior vena cava

12
pancreatic duct

13
Upper abdominal calcification
may be an important sign of disease Gallstones ,Porcelain gallbladder Urinary Calculi Calcified adrenal glands Pancreatic calcification Tumor calcification ……………

14
Gallstones 15% -20%of gallstones contain sufficient calcium to be identified on plain film right upper quadrant laminated appearance (a dense outer rim and more radiolucent center)
")
16
Porcelain gallbladder
calcification in the wall of the gallbladder indicative of chronic obstruction of the cystic duct, chronic gallbladder inflammation, and an increased risk of gallbladder carcinoma

17
Discontinuous mural calcification diffuse

18
Kidney stones About 85% of urinary calculi are visible on plain film.
Staghorn Calculus a large calculus occupying the collecting system of the left kidney and assuming its shape

19
Calcified adrenal glands
associated with adrenal hemorrhage in the newborn, tuberculosis, and Addison disease either side of the first lumbar vertebra

20
Pancreatic Calcifications
chronic alcohol-induced pancreatitis Coarse and punctate calcifications extend upward across the left upper quadrant

22
Intestinal Distention
The small bowel is dilated when it exceeds 2.5 to 3.0 cm in diameter. The colon is dilated when it exceeds 5 cm in diameter The cecum is dilated when it exceeds 8 cm in diameter.

23
Normal Bowel Gas Pattern
The normal distribution of gas in the stomach and duodenum The colon----- mottled pattern of stool The small bowel----a few gas collections

24
Mechanical bowel obstruction Small Bowel
Dilated loops of small bowel (>3 cm) Air-fluid levels that exceed 2.5 cm in length Air-fluid levels at differing heights within the same loop (strong evidence of obstruction) Small bubbles of gas trapped between the valvulae conniventes
 Air-fluid levels that exceed 2.5 cm in length. Air-fluid levels at differing heights within the same loop (strong evidence of obstruction) Small bubbles of gas trapped between the valvulae conniventes.")
25
Causes of Small Bowel Obstruction

26
Erect radiograph of the abdomen
Air-fluid levels at different heights The valvulae conniventes that extend across the entire diameter of the bowel lumen

28
Mechanical bowel obstruction Large Bowel
Most colonic obstructions occur in the sigmoid colon Dilation of the colon from the cecum to the point of obstruction The colon distal to the obstruction is devoid of gas

29
Causes of Large Bowel Obstruction

31
Sigmoid volvulus A large gas-filled loop(inverted U shape or a coffee bean shape) without haustra or septa, Arising from the pelvis and extending high into the abdomen and often to the diaphragm Barium enema: a beaking sign at the point of the twist

32
Adynamic ileus(Functional ileus)
Decreased or absent peristalsis Diffuse gaseous, distension of bowel(small bowel and colon,rectum)
")
33
Pneumoperitoneum Common causes:bowel perforation, trauma, recent surgery Free air beneath the domes of the diaphragm

34
Dysphagia: Esophagus The length of the esophagus is tubular, and its termination is saccular A ring: the tubulovestibular junction is formed by a symmetric muscular ring B ring : an asymmetric mucosal ring or notch that occurs at the junction of esophageal squamous epithelium with gastric columnar epithelium

35
The esophageal vestibule
demarcated by the muscular A ring and the mucosal fold of the B ring B ring (mucosal ring) <14mm---always symptomatic 14mm-20mm--50% symptomatic >20mm---asymptomatic
 <14mm---always symptomatic. 14mm-20mm--50% symptomatic. >20mm---asymptomatic.")
36
Benign Stricture Resulting from Reflux Esophagitis
usually confined to the distal esophagus may be tapered, smooth, and circumferential (the classic appearance)
")
37
Esophageal carcinoma Four basic radiographic patterns
An annular constricting lesion, appearing as an irregular ulcerated stricture, is most common. The polypoid pattern causes an intraluminal filling defect The infiltrative variety grows predominantly in the submucosa and may simulate a benign stricture. The least common pattern is that of an ulcerated mass.

38
Malignant Stricture Abrupt narrowing with irregular mucosa The prominent shoulders are characteristic of tumor

39
Polypoid Squamous Cell Carcinoma

40
Esophageal achalasia usually at age 30 to 50 years
Absence of peristalsis of body of esophagus Failure of the LES to relax with swallowing Smooth,tapered or beaklike appearance

41
Anatomy of the Upper GI Tract

42
Normal anatomy of stomach
composed of the cardia, fundus, body, and antrum

43
A well-distended stomach has a wall thickness of approximately 5 mm

44
Benign Ulcer(1) Projection beyond the lumen of stomach
soomth lucent line (collar ) at the neck of ulcer
 at the neck of ulcer.")
45
Benign Ulcer(2) Hampton line :a thin, sharp, lucent line that traverses the orifice of the ulcer.
 Hampton line :a thin, sharp, lucent line that traverses the orifice of the ulcer.")
46
Benign Ulcer(3) Radiating folds extending into the crater
 Radiating folds extending into the crater")
47
Malignant ulcer location within the lumen of the stomach
nodular, rolled, irregular, or shouldered edges

48
Gastric adenocarcinoma
The most common malignancy in the stomach The pattern of spread : local extension , distant metastases drop metastases to the ovaries

49
Polypoid Gastric Carcinoma
Polypoid Gastric Carcinoma. a lobulated filling defect (arrows) in the antrum of the stomach.
 in the antrum of the stomach.")
50
CT: focal wall thickening diffuse wall thickening
a lobular mass with or without ulceration destruction of the multilayered pattern or with transmural enhancement regional lymphadenopathy; metastases

51
CT: Focal wall thickening transmural enhancement

52
CT:diffuse wall thickening

53
Locally invasive gastric adenocarcinoma
heterogeneous thickening of the gastric fundus. growing into the splenic hilum , left adrenal gland

54
A large heterogeneous mass in the body of the stomach
round and contains an ulcer A large metastasis lies in the liver

55
Lymphatic spread

56
Gastrointestinal stromal tumors (GISTs)
the most common mesenchymal tumors distinct from true smooth muscle and neural tumors The best defining feature :the expression of KIT (CD117) arise from the pacemaker cells of Cajal
 arise from the pacemaker cells of Cajal.")
57
extragastric (most cases)
Growth pattern) extragastric (most cases)
 extragastric (most cases)")
58
polypoid in appearance (small GISTs)
")
59
Large, heterogeneous exophytic mass

60
Extensive ulceration of the mass

61
Diffuse Liver Disease Fatty liver Cirrhosis

62
Fatty liver(Steatosis)
In normal adults, the precontrast attenuation value of the liver is consistently higher than that of the spleen Milder degrees of diffuse steatosis :the attenuation value of the liver is less than that of the spleen Marked diffuse steatosis :the liver parenchyma is lower in attenuation than the hepatic blood vessels

63
The attenuation value of the liver parenchyma is markedly lower than that of the spleen
The intrahepatic vessels stand out as hyperattenuating structures

64
Focal fatty infiltration
The same imaging features as diffuse infiltration Vessels run their normal course through the area of involvement (lack of mass effect )
")
65
Cirrhosis hypertrophy of the caudate lobe and left lobe with shrinkage of the right lobe inhomogeneity of hepatic parenchyma, irregularity (nodularity) of the liver surface, Extrahepatic signs :evidence of portal hypertension, splenomegaly, and ascites
 of the liver surface, Extrahepatic signs :evidence of portal hypertension, splenomegaly, and ascites.")
66
nodularity of the liver contour
atrophy of the medial segment (M) and enlargement of the lateral segment prominent notch in the right posterior surface of the liver
 and enlargement of the lateral segment. prominent notch in the right posterior surface of the liver.")
67
Focal Liver diseases Cyst Hemangioma Hepatocellular carcinoma
metastasis

68
Cyst:CT appearance a well-circumscribed, homogeneous mass of near-water-attenuation value (less than 20 HU) no enhancement after IV contrast medium administration

69
Two large well-circumscribed, homogeneous, near-water-density masses
no discernible wall

70
Hemangioma the most common benign liver tumor
fed by hepatic artery branches internal circulation is slow generally remain stable in size over time

71
well-defined, hypodense on unenhanced scans
Enhancement pattern : nodular enhancement from the periphery of the lesion and proceeding toward the center gradually

72
Precontrast CT :an attenuation value similar to that of the blood in the inferior vena cava(IVC)
")
73
Arterial phase :multiple areas of globular, peripheral enhancement.
Note that the enhanced portions of the mass have an attenuation value similar to that of the intrahepatic vessels.

74
Equilibrium phase : near-complete enhancement of the mass with an attenuation value equivalent to that of the blood in the inferior vena cava(IVC) and hepatic veins
 and hepatic veins")
75
T2WI:marked hyperintense

76
Hepatocellular carcinoma
The most common primary malignancy of the liver Risk factors : cirrhosis, chronic hepatitis Growth patterns: solitary massive, multinodular, and diffuse infiltrative Serum α-fetoprotein(AFP) levels are often elevated
 levels are often elevated.")
77
Hypervascular :contrast enhancement on arterial phase images, with diminishing enhancement on delayed phase images Tumor thrombus Tumor capsule: a sharply marginated rim

79
Necrosis: central low density
The satellite lesions

82
T2WI T1WI AP PP DP

83
Portal Vein Thrombosis
Multiple hypodense nodules ----HCC Filling defect with the vein

84
Metastases The most common malignant masses in the liver
Most commonly originate from the GI tract, breast, and lung Necrosis, fibrosis, calcification, or hemorrhage within the mass The most common enhancement pattern :continuous ring-like enhancement

85
Multiple Hypoattenuating lesions with mild continuous rim enhancement

86
T2WI:a central area of hyperintensity
rim enhancement

87
Normal MR Cholangiopancreatography (MRCP).
.")
88
Biliary Dilatation Diameter of intrahepatic bile ducts larger than 40% of the diameter of the adjacent portal vein Dilation of the common duct greater than 6 mm Gallbladder diameter greater than 5 cm

90
Causes of Biliary Tract Obstruction

91
Choledocholithiasis approximately 20% of cases of obstructive jaundice in the adult CT:high-density calcification within the duct MRCP has shown good sensitivity (86% to 100%) and specificity (85% to 100%) for ductal stones
 and specificity (85% to 100%) for ductal stones.")
94
MRCP Filling defects

95
Cholangiocarcinoma arise from the epithelium of bile ducts and are usually adenocarcinomas Growth patterns include mass forming, periductal infiltrating, and intraductal polypoid

96
Mass forming periductal infiltrating Intraductal polypoid

97
Peripheral cholangiocarcinoma
Delayed enhancement biliary dilatation Atrophy (liver)
")
99
Perihilar and extrahepatic cholangiocarcinomas
typically exhibit an infiltrating growth pattern focal, circumferential thickening of the bile duct with proximal dilatation perihilar lesions may be similar in appearance to the intrahepatic, mass-forming type of cholangiocarcinoma, or may manifest as an intraluminal polypoid mass

104
Pancreatic carcinoma a highly lethal tumor
CT is recommended for initial imaging assessment CT:a hypodense mass that distorts the contour of the gland obstruction of the common bile duct and pancreatic duct and atrophy of pancreatic tissue beyond the tumor

105
B A C D

107
Signs of unresectability
tumor involvement of adjacent organs enlarged regional lymph nodes (>15 mm) encasement or obstruction of peripancreatic arteries or veins metastases in the liver peritoneal carcinomatosis
 encasement or obstruction of peripancreatic arteries or veins. metastases in the liver. peritoneal carcinomatosis.")
108
Pancreatic Carcinoma: Nonresectable
encases and narrows the celiac axis and its branches partially envelopes the aorta

109
Plain film radiographs of the abdomen are important for the assessment of the acute abdomen
CT, US, and MR provide comprehensive evaluation of the abdomen, including the peritoneal cavity, retroperitoneal compartments, abdominal and pelvic organs, blood vessels, and lymph nodes

110
Thank you !

Similar presentations