Download presentation
Presentation is loading. Please wait.

1
Professor Altaf Talpur Surgical unit -3
UPPER GI BLEEDING Professor Altaf Talpur Surgical unit -3

2
Outline Introduction Treatment Aetiology Complications Presentation
Resuscitation Diagnosis History Clinical examination investigations Treatment Complications Follow up Prognosis conclusion

3
Introduction Bleeding of GIT proximal to ligament of treitz.
Ligament of treitz- a fibromuscular band which extends from right crus of diaphragm to duodenojejunal flexure.

4
Presents as: Haematemesis,, malena, hematochezia or occult blood. Malena can present with loss of 50-60ml of blood. May be acute or chronic 100 cases per 100,000 person per year.

5
Accounts for 3-5% of all hospitalizations
The incidence is 2- fold greater in males but death rate is similar in both sexes. Overall mortality from acute bleeding is 20% . Mortality & morbidity increases as age advances (>60 yrs)
")
6
Etiology of upper GI bleeding

7
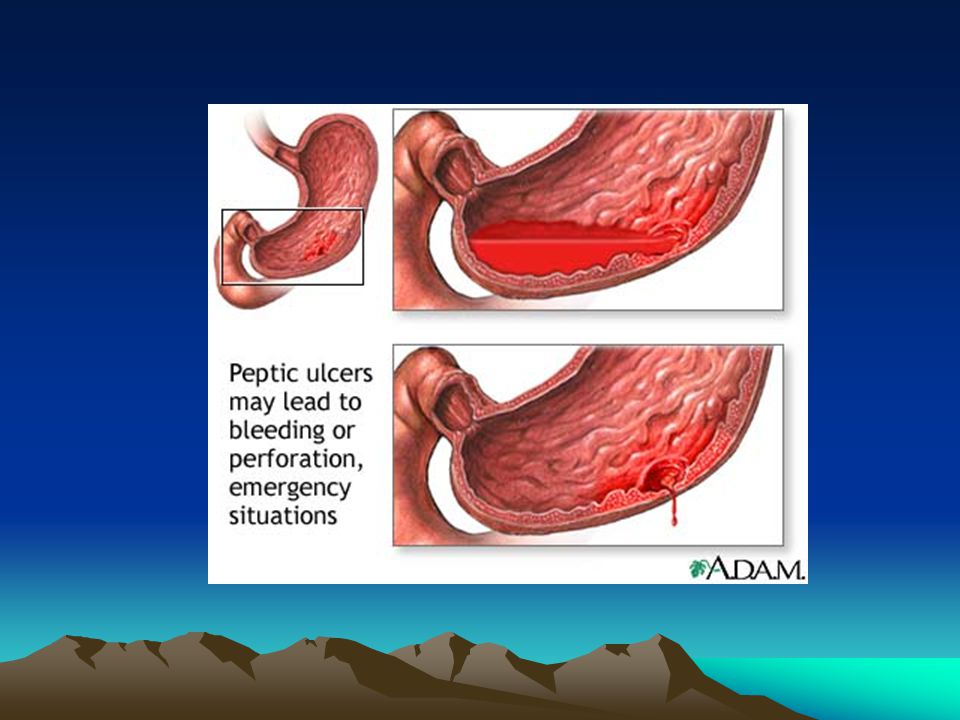
Aetiology (Common causes)
Peptic ulcer disease ≥ 50% of cases Duodenal ulcer Gastric ulcer Stomal ulcer

9
Aetiology (Common causes)
Erosive gastritis, esophagitis, duodenitis 15-30% of cases Common causative factors are: ETOH [alcohol], ASA, NSAID’S,STEROIDS.

10
Erosive gastritis

11
Aetiology (Common causes)
Esophageal and gastric varices 10-20% of cases caused by portal hypertension

12
Esophageal varices

13
Aetiology (Common causes)
Mallory- Weiss syndrome 5% of cases Characterized by longitudinal mucosal tear in the cardioesophageal region. Result from repeated vomitting or retching. Common in male alcoholic patients

14
Mallory Weis Syndrome

15
Aetiology Less common Rare Oesophagitis Malignant gastric tumor
Benign gastric tumors Oesophageal ulcer Oesophageal tumors A-V malformations Rare Duodenal tumous Pancreatic tumors Arterial aneurysm Blood dyscrasia Hereditary telangiectasia Haemobilia

16
Malignancy In 3% of cases presentation is with upper GI bleeding
Gastric cancer Oesophageal cancer

17
ESOPHAGEAL TUMORS

18
GASTRIC TUMORS

19
Clinical presentation
Chronic upper GI bleeding Anemia. Weakness. Fatigueness. Pt :looks pale. Malena. Occult blood positive.

20
Acute upper GI bleeding
Presents as emergency with hemetemesis or malena. Hypovolaemia: Mild: no significant hypovolaemia. Moderate: hypovolaemia which responds to volume replacement. Severe: hypovolaemia with continued active major bleeding making resuscitation difficult even with blood transfusions. These patients are difficult to manage. Patients will show all signs of shock.

21
Note: all patients should be examined for stigmata of CLD.
H/O drugs (NSAIDS). H/O ulcers. H/O alcohol abuse.
. H/O ulcers. H/O alcohol abuse.")
22
Resuscitation Initial management has 4 primary goals:
Quick assessment with attention to hemodynamic status Appropriate resuscitation (ABC) & monitoring Identify major source of bleeding Specific therapeutic intervention.
 & monitoring. Identify major source of bleeding. Specific therapeutic intervention.")
23
Resuscitation (General measures)
Airway cleared of clot. Oxygen inhalation. Maintain IV line with at least 2 wide bore cannulae Sample to blood bank for cross matching. Class I + II hemorrhage replace with crystalloid. Class III + IV hemorrhage replace with crystalloid & blood. Pass NG tube for diagnostic & therapeutic purpose. Catheterize the patient. Sedation may be needed.

24
SEVERITY

25
Specific measures If stable following resuscitation, proceed for upper GI endoscopy. Endoscopy ideally done within 4-24 hrs. If patient could not be stabilized, an emergency laparatomy may be necessary.

26
Diagnosis History of: Epigastric pain or retrosternal burning
hematemesis, melena, or hematochezia. Vomiting, weight loss, alteration of bowel habits. Aortic graft surgery Use of ASA, NSAID’S, steroids, alcohol addiction

27
Diagnosis Physical examination
Vital signs may show hypotension & tachycardia. Cool, clammy skin. Petechiael hemorrhage & purpura seen in coagulopathy. Signs of chronic liver disease. Proper abdominal & rectal examination.

28
Investigations Upper GI endoscopy. Arteriography. Barium swallow
Ultrasound Lab investigations

29
Endoscopy Most important investigation For diagnosis & intervention
Establishes diagnosis in 90% of patients Can be repeated more than once.

30
Arteriography In pts who bleeds contineously & site can not be identified. Has accuracy of 50-90%. Accuracy is increased if there is active bleeding during investigation. Demonstrates bleeding of ml/min With technetium-labelled RBC, ml/min Embolisation may be done at same time

31
Barium swallow / meal Used when endoscopy is not available
Double contrast study is ideal May show varices, esophagitis, peptic ulcers, gastric tumors etc

32
Abdominal Ultrasound scan
To assess both liver architecture and portal circulation More widely available than Arteriography Should be performed before more invasive procedures

33
Lab Investigations CBC Electrolytes Glucose Coagulation studies
Liver function studies Blood grouping and cross-match

34
Lab investigations CBC, urea/creatinine, S/Electrolytes, ABGs.
ed urea/ creatinine in upper GI bleeding. Normal Hb in pts with active bleeding. Iron deficiency anemia in chronic blood loss.

35
Treatment ( peptic ulcer disease)
At endoscopy 10ml epinephrine at ulcer base Thermal treatment with bipolar diathermy Laser photocoagulation Rebleed is treated similarly A second rebleed is treated by surgery

36
Post endoscopy treatment
Continuous intravenous infusion of Octretide (somatostatin analogue) Proton pump inhibitors H. pylori treatment may be required.
 Proton pump inhibitors. H. pylori treatment may be required.")
37
Surgery- PUD Surgical options are: Truncal vagotomy & drainage
Highly selective vagotomy Partial gastrectomy

38
Surgery - PUD Indications for surgery are: Exsanguinating hemorrhage
Visible spurting arterial bleed Concomitant perforation Pts >60 yrs, who rebleed once or need 4 units at resuscitation or 8 units in 48 hrs Younger pts requiring 8 units at initial resuscitation or 12 units in 48 hrs Rare blood group

39
Treatment Gastric erosions / stress ulcers
Treatment of underlying cause Intraluminal antacids IV proton pump inhibitors Bleeding usually subsides in hrs

40
Treatment Esophageal varices
1. Endoscopic sclerotherapy Repeated at 3 weeks interval then 3 monthly until varices disappear Some sclerosing agents are ethanolamine oleate, sodium morrhuate, 3% tetradecyl sulphate, absolute alcohal 2. Rubber band ligation 3. Vasoconstriction therapy (octreotide, vasopressin, propranolol)
")
41
Sclerotherapy of esophageal varices

42
Esophageal variceal Banding

43
4. Balloon tamponade: if above measures fail
Modified Sengstaken- Blakemoore tube Minnesota tube, Linton tube, Foley catheter Balloon tamponade applied for 12 hrs Stop bleeding in 80% of cases Must be followed by surgery as bleeding is likely to recur after removal.

44
Balloon temponade

45
Surgery – esophageal varices
TIPS: in refractory bleed Shunt established between portal vein & Rt or middle hepatic vein Stapling transection of esophagus at CEJ Distal splenorenal shunt Portosystemic shunts Spleenectomy in hypersplenism Liver transplantation

46
Transjuglar intrahepatic portosystemic shunt [TIPS]_
![Transjuglar intrahepatic portosystemic shunt [TIPS]_](http://slideplayer.com/slide/3883170/13/images/46/Transjuglar+intrahepatic+portosystemic+shunt+%5BTIPS%5D_.jpg "Transjuglar intrahepatic portosystemic shunt [TIPS]_")
47
Treatment Mallory- weiss Esophagitis Benign gastric tumors
observe if persist, suture mucosal tear Esophagitis Observe Benign gastric tumors Excise Dieulafoy’s lesion Endoscopic electrocoagulation, sclerotherapy

48
Complications Of presenting problem Of resuscitative measures
Of underlying disease Of treatment

49
Complications of massive hemorrhage
Hemorrhagic shock Acute renal shut down MODS Death

50
Complications of resuscitation
Fluid overload Pulmonary edema CCF Blood transfusion reaction Cardiac arrest Hypothermia Esophageal perforation

51
Complications of underlying diseases
Rebleed in PUD & varices Gastric outlet obstruction in PUD Progressive CLD causing portal hypertension, ascites & coagulopathies

52
Complications of definitive surgery
PUD Early & late dumping gastric tumors Iron deficiency anemia Bypass procedures for portal hypertension mucosal ulceration Hepatic encephalopathy

53
Follow-up To monitor progress of non- surgical treatment
To prepare pts for elective definitive surgery To look out for, and treat complications of surgery

54
Prognosis Depends upon ROCKALL scoring system this includes :
The state / time of presentation of pt energetic resuscitation underlying disease Co morbidities

55
ROCKALL SCORING SYSTEM

56
Adverse prognostic factors

57
Conclusion Upper GI bleeding is not uncommon & may be life threatening. Prompt intervention could be life saving. It require multidisciplinary approach. Definitive treatment depends upon the final diagnosis.

58
THANK YOU

Similar presentations










>")

 682-3793; (p) 413-3222.>")






