Download presentation
Presentation is loading. Please wait.

1
Hemorrhagic Fevers With a Concentration on Filoviruses Simon A Francis Susanna Epstein Medha Goyal

2
History Hemorrhagic Fevers –Definition: a severe multi-system syndrome. Vascular System Damaged Body regulation Impaired Accompanied by hemorrhage –Four families of viruses Arenaviruses (Junin Virus) Nariovirus )Bunyaviruses (Nariovirus ) Flaviviruses (ie. Yellow Fever) Filoviruses (Marburg & Ebola) –CDC Classification: BSL-4 Agent
 Nariovirus )Bunyaviruses (Nariovirus ) Flaviviruses (ie. Yellow Fever) Filoviruses (Marburg & Ebola) –CDC Classification: BSL-4 Agent.")
3
History Hemorrhagic Fevers (Continued)Hemorrhagic Fevers (Continued) –RNA viruses covered in a lipid coating –Viruses are geographically restricted to areas where host species live –Humans are not natural reservoirs for these viruses
Hemorrhagic Fevers (Continued) –RNA viruses covered in a lipid coating –Viruses are geographically restricted to areas where host species live –Humans are not natural reservoirs for these viruses")
4
History Filoviruses –Marburg Virus A.K.A. (African Hemorrhagic Fever, Green Monkey Disease, Marburg Fever) First outbreak (Marburg Germany, 1967) laboratory workers infected by monkeys Simultaneous outbreak in Hamburg, Germany and Belgrade, Yugoslavia (now Serbia) 32 human cases 31 primary one generation of secondary transmission 23% of human mortality Overall Mortality 23%-25%
 First outbreak (Marburg Germany, 1967) laboratory workers infected by monkeys Simultaneous outbreak in Hamburg, Germany and Belgrade, Yugoslavia (now Serbia) 32 human cases 31 primary one generation of secondary transmission 23% of human mortality Overall Mortality 23%-25%.")
5
History Filoviruses (continued) –Ebola Virus Named after a river in the Republic of Congo (Formerly Zaire) First outbreak (Zaire 1967) –318 human cases –88% mortality –Disease spread by close personal contact in hospital setting (amplification) Fatal in humans and non-human primates 80 nm in diameter)Four subtypes (~ 80 nm in diameter) 990-1086 nm in length )974- 1063 nm in length) 1026-1083 nm in length ) –Ebola-Zaire(990-1086 nm in length ), Ebola-Sudan (974- 1063 nm in length), Ebola-Ivory Coast, Ebola-Reston (disease in non-human primates 1026-1083 nm in length )
 –Ebola Virus Named after a river in the Republic of Congo (Formerly Zaire) First outbreak (Zaire 1967) –318 human cases –88% mortality –Disease spread by close personal contact in hospital setting (amplification) Fatal in humans and non-human primates 80 nm in diameter)Four subtypes (~ 80 nm in diameter) nm in length ) nm in length) nm in length ) –Ebola-Zaire( nm in length ), Ebola-Sudan ( nm in length), Ebola-Ivory Coast, Ebola-Reston (disease in non-human primates nm in length )")
6
History Filoviruses (Continued) –Ebola (Continued) Sudan international scientist arrived –To late to deal with virulent epidemics »Hospitals closed »Infected patients quarantined –Reconstructed data from survivors
 –Ebola (Continued) Sudan international scientist arrived –To late to deal with virulent epidemics »Hospitals closed »Infected patients quarantined –Reconstructed data from survivors")
7
Outbreaks Marburg –Europe Outbreaks 1967 Hamburg and Marburg, Germany and Belgrade, Yugoslavia –Africa Outbreaks 1975 –Johannesburg, South Africa –3 died 1980 –Western Kenya –2 Died (Physician died in Nairobi) 1987 –Young man traveling extensively in Kenya 1999-2000 –Outbreak in Durba, Republic of Congo –Cases linked to workers in a gold mine
 1987 –Young man traveling extensively in Kenya –Outbreak in Durba, Republic of Congo –Cases linked to workers in a gold mine")
8
Outbreaks Ebola (types named after location) This diagram was adapted from a WHO publication accompanied by the following note (edited): Phylogenic tree showing the evolutionary relationship of Ebola viruses (courtesy of A. Sanchez, Centers for Disease Control and Prevention [CDC]; derived from Georges-Courbet MC, Sanchez A, Lu CY, et al. Isolation and phylogenetic characterization of Ebola viruses causing different outbreaks in Gabon. Emerg Infect Dis 1997;3:59-62).
..")
9
YearEbola subtypeCountryNo. of human cases Percentage of deaths among cases Situation 1976Ebola-ZaireZaire [Democratic Republic of the Congo (DRC)] 31888%Occurred in Yambuku and surrounding area. Disease was spread by close personal contact and by use of contaminated needles and syringes in hospitals/clinic s. This outbreak was the first recognition of the disease. 1976Ebola-SudanSudan28453%Occurred in Nzara, Maridi and the surrounding area. Disease was spread mainly through close personal contact within hospitals. Many medical care personnel were infected. 1976Ebola-SudanEngland10%Laboratory infection by accidental stick of contaminated needle. 1977Ebola-ZaireZaire1100%Noted retrospectively in the village of Tandala.
] 31888%Occurred in Yambuku and surrounding area. Disease was spread by close personal contact and by use of contaminated needles and syringes in hospitals/clinic s. This outbreak was the first recognition of the disease. 1976Ebola-SudanSudan28453%Occurred in Nzara, Maridi and the surrounding area. Disease was spread mainly through close personal contact within hospitals. Many medical care personnel were infected. 1976Ebola-SudanEngland10%Laboratory infection by accidental stick of contaminated needle. 1977Ebola-ZaireZaire1100%Noted retrospectively in the village of Tandala..")
10
1979Ebola-SudanSudan3465%Occurred in Nzara. Recurrent outbreak at the same site as the 1976 Sudan epidemic. 1989Ebola-RestonUSA00%Ebola-Reston virus was introduced into quarantine facilities in Virginia, Texas, and Pennsylvania by monkeys imported from the Philippines. Four humans developed antibodies to Ebola- Reston virus but did not become ill. 1990Ebola-RestonUSA00%Ebola-Reston virus was introduced once again into quarantine facilities in Virginia, and Texas by monkeys imported from the Philippines. Four humans developed antibodies but did not get sick. 1992Ebola-RestonItaly00%Ebola-Reston virus was introduced into quarantine facilities in Sienna by monkeys imported from the same export facility in the Philippines that was involved in the episodes in the United States. No humans were infected.

11
1994Ebola-ZaireGabon4959%Occurred in Mékouka and other gold-mining camps deep in the rain forest. Initially thought to be yellow fever; identified as Ebola hemorrhagic fever in 1995. 1994Ebola-Ivory CoastIvory Coast10%Scientist became ill after conducting an autopsy on a wild chimpanzee in the Tai Forest. The patient was treated in Switzerland. 1995Ebola-ZaireDemocratic Republic of the Congo (formerly Zaire) 31581%Occurred in Kikwit and surrounding area. Traced to index case-patient who worked in forest adjoining the city. Epidemic spread through families and hospitals. 1996Ebola-ZaireGabon3168%Occurred in Mayibout area. A chimpanzee found dead in the forest was eaten by people hunting for food. Nineteen people who were involved in the butchery of the animal became ill; other cases occurred in family members.
 31581%Occurred in Kikwit and surrounding area. Traced to index case-patient who worked in forest adjoining the city. Epidemic spread through families and hospitals. 1996Ebola-ZaireGabon3168%Occurred in Mayibout area. A chimpanzee found dead in the forest was eaten by people hunting for food. Nineteen people who were involved in the butchery of the animal became ill; other cases occurred in family members..")
12
1996Ebola-ZaireGabon6075%Occurred in Booué area with transport of patients to Libreville. Index case-patient was a hunter who lived in a forest camp. Disease was spread by close contact with infected persons. A dead chimpanzee found in the forest at the time was determined to be infected. 1996Ebola-ZaireSouth Africa250%A medical professional traveled from Gabon to Johannesburg, South Africa, after having treated Ebola virus-infected patients and thus having been exposed to the virus. He was hospitalized, and a nurse who took care of him became infected and died. 1996Ebola-RestonUSA00%Ebola-Reston virus was introduced into a quarantine facility in Texas by monkeys imported from the Philippines. No human infections were identified.

13
1996Ebola-RestonPhilippines00%Ebola-Reston virus was identified in a monkey export facility in the Philippines. No human infections were identified. 2000- 2001 Ebola- Sudan Uganda42553%Occurred in Gulu, Masindi, and Mbarara districts of Uganda. The three most important risks associated with Ebola virus infection were attending funerals of Ebola hemorrhagic fever case-patients, having contact with case-patients in one's family, and providing medical care to Ebola case- patients without using adequate personal protective measures. 2001- 2002 Ebola-ZaireGabon and The Republic of the Congo 12279%Outbreak occurred over the border of Gabon and the Republic of the Congo. Additional information is currently available on the WHO website.WHO website

14
New York Times February 15, 2003 World Briefing: Africa CONGO REPUBLIC: EBOLA TOLL REACHES 51 The death toll from a suspected outbreak of the deadly Ebola virus in Congo Republic has crept up to 51, and people have begun fleeing into dense forest to escape what some believe to be an evil spell. The authorities have tried to impose tight restrictions on movement in the hope of preventing the spread of the outbreak, the second reported in little over a year in the country's remote northwest. It is thought to have been caused by the consumption of infected monkey meat. (Reuters)
.")
15
Transmission Ebola Virus –No carrier state (reservoir Unknown) –Researchers Hypothesize that it is Zoonotic –Unpopular theory that plant may be the reservoir of the virus –Human to Human Transmission through contact of contaminated secretions. Ebola-Reston –Occurred in the U.S (Reston, VA) –Occurred in African Green Monkeys –Why only to non-human primates? Four scientist found to have antibody for the disease –Circumstantial Evidence of airborne transmission Spread within and between rooms (national center for Infectious Diseases) Marburg Virus –Transmission from animal host unknown –Human to Human (Close Contact and change of fluids highly suspect source of transmission)
 –Occurred in African Green Monkeys –Why only to non-human primates. Four scientist found to have antibody for the disease –Circumstantial Evidence of airborne transmission Spread within and between rooms (national center for Infectious Diseases) Marburg Virus –Transmission from animal host unknown –Human to Human (Close Contact and change of fluids highly suspect source of transmission).")
16
Reservoir Not known May be –A rare species –One that usually does not contact clinical host – If contact is made the virus may not be easily transmitted Hypothesize –Bats –Plants

19
Filoviruses General Facts Replication: –Not fully understood. Created by budding of the surface of their host cells (Susanna) Structure: –Pleomorphic: Long sometimes branched filament shaped like a “6”, “U” or a circle. –Each Virion contains one molecule of single stranded, negative sense RNA (Susanna) Symptoms of Ebola and Marburg (Medha)
 Structure: –Pleomorphic: Long sometimes branched filament shaped like a 6 , U or a circle. –Each Virion contains one molecule of single stranded, negative sense RNA (Susanna) Symptoms of Ebola and Marburg (Medha).")
20
INCUBATION & DEATH PERIODS Ebola Incubation at 2 – 21 Days Marburg Incubation: : 3-9 days VHF (in general) - Death Between 7 – 16 Days Ebola Death Ensues as Early as 2 Days after expression of symptoms
 - Death Between 7 – 16 Days Ebola Death Ensues as Early as 2 Days after expression of symptoms")
22
Morphology and Structure Filamentous or Bacillus form Vary greatly in length (up to 14000 nm) Mean Unit Length Marburg- 860 nm Ebola- 1200 nm Uniform diameter of 80 nm
 Mean Unit Length Marburg- 860 nm Ebola nm Uniform diameter of 80 nm")
23
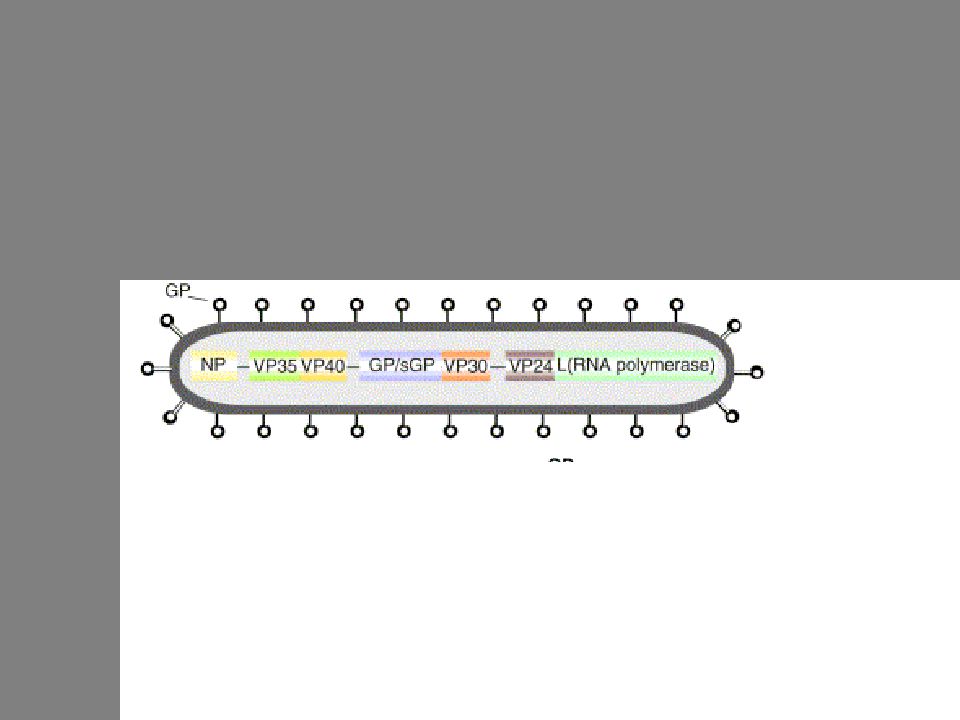
Filovirus Composed of: Ribonucleoprotein complex (nucleocapsid) Matrix Envelope studded with peplomers (10 nm long)
 Matrix Envelope studded with peplomers (10 nm long)")
24
Filovirus Genome Nonsegmented, negative-strand RNA Filovirus Genome – 19 kb 7 Genes Nucleotide and amino acid differences b/w Marburg and Ebola – 55% Ebola – 37 to 41% Overlaps 1 in Marburg genome – VP30 to VP24 2 in Ebola genome- VP35 to VP40 & GP to VP30

25
Glycoprotein Gene Marburg- GP gene encodes 1 product 1 open reading frame (0) Ebola- GP gene encodes 2 products 2 open reading frames (0 & -1) connected by the insertion of 1 additional A at a series of 7 U’s on the genomic RNA
 Ebola- GP gene encodes 2 products 2 open reading frames (0 & -1) connected by the insertion of 1 additional A at a series of 7 U’s on the genomic RNA")
26
The 7 sequentially arranged genes are transcribed into Ebola - 8 major mRNAs (7 structural proteins and 1 nonstructural protein) Marburg – 7 major mRNAs (7 structural proteins)
 Marburg – 7 major mRNAs (7 structural proteins)")
27
Filovirus Proteins Ebola and Marburg encode 7 structural proteins Ebola encodes 1 nonstructural protein Two Main Categories Associated with the nucleocapsid transcription and replication of viral genome Associated with the envelope assembly of virus receptor binding and virus entry

28
Ribonucleocapsid Proteins 1. Nucleoprotein (NP) Gene 1 2. Viral Protein 35 (VP35) Gene 2 3. Viral Protein 30 (VP30) Gene 5 4. Polymerase L Gene 7 Matrix Proteins 5. Viral Protein 40 (VP40) Gene 3 6. Viral Protein 24 (VP24) Gene 6 Membrane Protein 7. Glycoproteins (GP) Gene 4 Secreted Protein 8. Secretory Glycoprotein (sGP) Gene 4
 Gene 2 3. Viral Protein 30 (VP30) Gene 5 4. Polymerase L Gene 7 Matrix Proteins 5. Viral Protein 40 (VP40) Gene 3 6. Viral Protein 24 (VP24) Gene 6 Membrane Protein 7. Glycoproteins (GP) Gene 4 Secreted Protein 8. Secretory Glycoprotein (sGP) Gene 4.")
30
Nucleoprotein Primary structural protein associated with the nucleocapsid Hydrophobic N-terminal half Binds genomic RNA Hydrophilic C-terminal half (Variable b/w Marburg and Ebola) Interacts with matrix proteins
 Interacts with matrix proteins")
31
VP30 - Minor structural protein associated with the nucleocapsid Polymerase L- Transcription and Replication (largest and least abundant protein) VP35- Cofactor in transcription and Replication (Cofactor in polymerase complex) VP40- Matrix protein Virus assembly and budding Forms hexamers when it contacts the plasma membrane which confers added stability during assemebly. (most abundant protein) VP24- Minor Matrix Protein Possibly uncoats virus during infection
 VP24- Minor Matrix Protein Possibly uncoats virus during infection.")
32
Expression of Glycoprotein Transcriptional RNA Editing (occurs only in Ebola) At a series of 7 U’s on the genomic RNA template insert a non-template-coded adenosine 20% of GP mRNA is edited GP with 680 amino acids 80% of GP mRNA is not edited sGP with 370 amino acids
 At a series of 7 U’s on the genomic RNA template insert a non-template-coded adenosine 20% of GP mRNA is edited GP with 680 amino acids 80% of GP mRNA is not edited sGP with 370 amino acids")
33
GP (Structural) Formation of GP 1 -GP 2 Heterodimer In the trans-Golgi, the precursor molecule (GP 0 ) is post-translationally cleaved by furin at yielding a heterodimer, (GP 1 -GP 2 ) Furin cleavage site (Arg-Arg-X-Arg/LYS-Arg) (Marburg, cleavage site is more toward N-terminus) Heterodimer is linked together by one disulfide bond, a cysteine bridge
 Formation of GP 1 -GP 2 Heterodimer In the trans-Golgi, the precursor molecule (GP 0 ) is post-translationally cleaved by furin at yielding a heterodimer, (GP 1 -GP 2 ) Furin cleavage site (Arg-Arg-X-Arg/LYS-Arg) (Marburg, cleavage site is more toward N-terminus) Heterodimer is linked together by one disulfide bond, a cysteine bridge")
35
GP 1 Molecule C-terminus: hydrophilic, highly glycosylated Sequences for receptor recognition and binding N-terminus: hydrophobic Connects GP 1 to GP 2 by a disulfide bond GP 2 Molecule Fusion peptide near near its N-terminus Capable of inserting itself in plasma membranes Believed to mediate the fusion of the host and virus membranes Functions of GP Forms the Virion Peplomers (Surface Spikes) Trimers of the GP 1 -GP 2 Heterodimer, probably assembled in the ER Mediates viral entry by receptor binding and membrane fusion
 Trimers of the GP 1 -GP 2 Heterodimer, probably assembled in the ER Mediates viral entry by receptor binding and membrane fusion")
36
sGP (non-structural) Formation and Structure Homodimer Synthesized from GP mRNA using the conventional ORF Produced from a precursor molecule cleaved by furin near the C- terminus, Precursor molecule SGP and Delta Peptide Homodimer is linked in anti-parallel orientation by 2 disulfide bonds between the 1 st and 6 th cysteines on separate molecules
 Formation and Structure Homodimer Synthesized from GP mRNA using the conventional ORF Produced from a precursor molecule cleaved by furin near the C- terminus, Precursor molecule SGP and Delta Peptide Homodimer is linked in anti-parallel orientation by 2 disulfide bonds between the 1 st and 6 th cysteines on separate molecules")
38
Virus Entry and Replication in Host Cells Viral surface spikes recognize and bind surface receptors of host Virus enters cell via endocytosis Release of nucleocapsid into cytoplasm Transcription viral RNA polyadenylated, monocistronic mRNA Translation and buildup of viral proteins, primarily NP Budding and release of viruses Host Cell – dies intracytoplasmic vesiculation, mitochondrial swelling, organelle breakdown

39
Molecules mediating filovirus entry Marburg Asialoglycoprotein Receptor (Found exclusively in hepatocytes) Recognizes glycoproteins displaying N-linked sugar chains with terminal galactose residues Ebola Integrins N-glycosylated transmembrane cell surface receptors Ebola and Marburg Human folate receptor- Co-factor expressed on cell-surface
 Recognizes glycoproteins displaying N-linked sugar chains with terminal galactose residues Ebola Integrins N-glycosylated transmembrane cell surface receptors Ebola and Marburg Human folate receptor- Co-factor expressed on cell-surface")
40
Reverse Transcription System Volchkov et al. contructed 2 recombinant EBOV clones 1. pFL-EBOVe + antigenomic cDNA clone with authentic editing site 2. pFL-EBOVe - antigenomic cDNA clone with mutated editing site Eliminated editing site using site-directed mutagenesis Editing site in middle of GP gene AAAAAAA EBOV polyadenylation signal ATTAAGAAAAAA AAAAAAA AAGAAGAA

42
Observations 1. Both pFL-EBOVe + and pFL-EBOVe - Showed typical filovirus structure Possessed similar infectivity and virus production 2. Visible Cytopathic Effects pFL-EBOVe + : 4-6 days after infection But there was still an intact monolayer at day 8 pFL-EBOVe - : 3-4 days after infection 5-6 days after infection, cell rounding was complete

43
3. Differences in expression of the GP gene Wild Type – 1/5 GP, 4/5 sGP pFL-EBOVe + - 1/5 GP, 4/5 sGP pFL-EBOVe - - no sGP expression, increase in GP expression The increase in GP expression by pFL-EBOVe - no simultaneous increase in virus release most of GP synthesized were immature precursors -with sugar side chains high in mannose -sensitive to treatment with endoglycosidase H -GP transport was arrested in ER or early Golgi

46
Conclusions No Transcriptional RNA Editing Over-expression of GP Exhausts Cell Host Machinery Eventual Cell Death So GP expression and cytotoxicity can be down- regulated by virus through transcriptional RNA editing and sGP expression

47
Pathogenesis of EBOV Infection sGP 1. Inhibits early activation of neutrophils -Binds to neutrophils via CD16b cell surface receptor -CD16b activates neutrophils via lateral membrane interaction with CR3 2. Adsorbs neutralizing antibodies GP 1. Specific region of GP induces cytotoxic effects in endothelial cells -Rapid release of vasoactive agents from infected cells -Induces cell rounding and detachment from extracellular matices -Increases cell membrane premeability

48
2. Proteolytic activation of GP 0 precursor via cleavage -EBO-Z GP cleaved by furin -Prerequisite for fusion between viral envelope and host cell membrane -Enables virus to replicate in host systematic infection 3. Two sequences contribute to evasion of host immunity -Possible immunosuppressive sequence in GP 2 molecule -Amino acid sequence at amino terminus suppresses lymphocyte mitogen-stimulated proliferation in vitro

49
Destruction of the Immune System 1. Infects mononuclear phagocytes and fibroblastic reticular system (associated with lymph nodes) - Failure of early T-cell activation -Disrupts antigen trafficking and cytokine production -Extensive apoptosis of blood leukocytes -Lymphopenia (reduction in lymphocyte #) and severe damage to lymphoid tissue 2. Macrophages and circulating monocytes help transmit virus to other tissues
 - Failure of early T-cell activation -Disrupts antigen trafficking and cytokine production -Extensive apoptosis of blood leukocytes -Lymphopenia (reduction in lymphocyte #) and severe damage to lymphoid tissue 2. Macrophages and circulating monocytes help transmit virus to other tissues.")
50
3. VP35 protein – Type 1 IFN Antagonist -Combats the host interferon response possibly enhancing the replicative ability of the virus

51
Key to Surviving Ebola French National Institute- Early Immune Response 1996 – Two large outbreaks in Gabon Compared immune responses Survived -IgG response against virus’s protein coat early on -Cleared circulating antigen -Activated cytotoxic T-cells Died -No IgG response -Barely detectable levels of IgM

52
Pathology of Marburg and Ebola EARLY STAGE: Striking lesions usually in liver, spleen and kidney Necrosis prominent in liver, lymph tissue, and spleen little inflammatory response Viral particles invade phagocytic cells

53
Pathology of Marburg and Ebola LATE STAGE: Liver and spleen become enlarged with excess blood Hemorrhage in the gastrointestinal tract, pleural, pericardial and peritoneal spaces and into the renal tubules with deposition of fibrin Abnormalities in coagulation parameters suggest that disseminated intravascular coagulation is a terminal event. There is usually also profound leukopenia in association with bacteremia. Example of cervical tissues with severely enlarged and hemorrhagic lymph nodes from a laboratory Rhesus monkey.

54
Differential Diagnosis High Fever Severe prostration Diffuse maculopapular rash Bleeding Myalgia Bradychardia Desquamation Loss of apetite

55
OTHER DIAGNOSTIC CRITERIA Coagulation Studies Serologic Study Leukopenia (Low White Blood Cell Count) Thrombocytopenia (Low Platelet Count) Low Electrolytes lymphopenia followed by neutrophilia
 Thrombocytopenia (Low Platelet Count) Low Electrolytes lymphopenia followed by neutrophilia")
56
DIAGNOSTIC TESTS FOR EBOLA ELISA (Enzyme-Linked Immunosorbent Assay) Can ’ t differentiate Ebola strains with electron microscope Indirect fluorescent antibody test (IFAT) Western blot analysis Radioimmunoprecipitation assay skin biopsies
 Can ’ t differentiate Ebola strains with electron microscope Indirect fluorescent antibody test (IFAT) Western blot analysis Radioimmunoprecipitation assay skin biopsies")
57
ELISA Purified, inactivated filovirus antigens pre-coated onto an ELISA platePurified, inactivated filovirus antigens pre-coated onto an ELISA plate If the patient has filovirus, serum contains antibodies to the filovirus antigens, and those antibodies will bind to the antigens on the plate. Test can be specific to IgM or IgG.If the patient has filovirus, serum contains antibodies to the filovirus antigens, and those antibodies will bind to the antigens on the plate. Test can be specific to IgM or IgG. Anti-human Ig coupled to Chromogen enzyme binds IgM or IgG.Anti-human Ig coupled to Chromogen enzyme binds IgM or IgG. Color change indicates positive testColor change indicates positive test

58
Clinical Course 2-21 Day incubation time 50-90% Mortality Variability of clinical presentations complicate early detection and management Non-specific prodrome typically lasts < 1 week 10 to 12 days after the onset of disease, the sustained fever may break, with improvement and eventual recovery of the patient. 1-2 weeks after onset of symptoms: Death often preceded by hemorrhagic diathesis, shock, multi-organ system failure

59
A Word From the Experts…

60
On Scene Footage…

61
Transmission Direct contact with the blood, secretions, organs or semen of infected persons: –study of risk factors among family members in Kikwit. 27 surviving members were interviewed. Determined that those who had direct contact or who were exposed during late hospital phase were at very high risk. Those who had no physical contact with infected members remained uninfected. –Transmission through semen occurs up to 80 days after clinical recovery. Handling ill or dead infected people or chimpanzees Health care workers have frequently been infected while attending patients- Kikwit outbreak. Neonatal Droplets or small filovirus particle aerosols confirmed in alveoli of monkeys during Reston outbreak.

62
Current Therapy Essentially supportive and directed toward ensuring adequate tissue delivery of oxygen, nutritional support, and hydration. Hemorrhage is managed by replacement of blood, platelets, and clotting factors Passive transfer of human antibodies has remained inconclusive in its benefit to Marburg and Ebola. Ribavirin is a synthetic nucleoside analog that is of use in treating Lassa fever and Arenavirus, but there is unfortunately no benefit in Ebola virus infection.

63
Prophylaxis Study shows: –hyperimmune globulin effective in protecting experimentally infected baboons if administered at the same time as virus, the treatment was ineffective if delayed for 3 days. Hyperimmune globulin should, however, be considered for prophylactic use in laboratory or nosocomial accidents although humans may require antibodies with higher specificity. Inconclusive evidence- whether whole blood transfusion from convalescent patients are effective. – Kikwit epidemic- 8 convalescent patients were given blood transfusions. 7/8 survived. Administered late, patients had better prognosis for survival, lack of controls.

64
Comorbidity: Pregnancy Illness from Ebola is generally more severe in pregnant women, with more serious hemorrhagic and neurologic complications Case fatality rate of pregnant women was 95.5% versus 77% in nonpregnant infected persons Spontaneous abortion is frequent, with fetal losses reported to be as high as 23%–66% All infants born to mothers with EHF ultimately died within 19 days of delivery

65
Potential Vaccines Dutch biotechnology company, Crucell, is to collaborate with the US National Institute of Allergy and Infectious Diseases (NIAID) to develop the first vaccine against the Ebola virus. –The new vaccine uses DNA encoding three Ebola glycoproteins and one nucleoprotein, followed by a boost with a replication-defective adenovirus expressing Ebola antigens (Nature 408, 605; 2000). It is the first vaccine to generate protective immunity against Ebola in non- human primates. Scientists at the US Army Medical Research Institute of Infectious Diseases report a simple method for generating Ebola virus–like particles. (JAMA March 2002) A researcher has discovered a link between HIV and Ebola virus: Both viruses use the same method to spread through the human body. Aids Alert - 01-Feb-2002
. It is the first vaccine to generate protective immunity against Ebola in non- human primates. Scientists at the US Army Medical Research Institute of Infectious Diseases report a simple method for generating Ebola virus–like particles. (JAMA March 2002) A researcher has discovered a link between HIV and Ebola virus: Both viruses use the same method to spread through the human body. Aids Alert - 01-Feb")
66
Vaccine Contd. Reverse genetics vs Forward genetics –genetics that is concerned with genetic material whose nucleotide sequence is known -analyzes its contribution to the phenotype of the organism by varying the nucleotide sequence -observe the results of such variation in the living organism, in living cells, or in vitro on macromolecules

67
Ebola from scratch In January 2002 scientists reported making Ebola using "reverse genetics". –They took the virus's genome plus pieces of DNA coding for the key viral proteins and added them to cells. These proteins then kick start the replication process. Good News: DNA is more stable and easily manipulated. Method provides in-depth understanding of viral mechanism of action that may lead to a vaccine/cure. Bad News: People acquire ability to synthesize Ebola

68
Weaponization History of Ebola Weaponization –Soko Asafra head of Aum Shinrikyo cult 1992 –Russians

69
THE APRIL of 1988 USTINOV INCIDENT Ustinov conducted basic research on the Marbur Virus studying its potential as a weapon Long term goal: To see if Marburg Virus could be loaded into special biological warheads on the Soviets MIRV missiles. MIRV has multiple warheads which are directed at different targets They at the time where designed to be loaded with strategic/operational smallpox virus, black death, and anthrax. Variant U was born

70
Weaponization Fall 1991 Marburg Variant U becomes a strategic operational Bioweapon Russians loaded virus into 10 separate cone- shaped warheads on the MIRV. –Cooling system inside each warhead keeps the virus alive during heat of atmosphere. –Biowarheads parachuted over the target city Certain altitude they break apart Each warhead burst a spray of more than a hundred oval bomblets each the size of a small cantaloupe Cantaloupes fly and then split again in an overlapping manner releasing a haze of bio-particles that quickly become invisible.

71
Challenges Finding the Reservoir Need to know more about Transmission –From animal to man –Ways of putting it into food Aerosolization –Possible –Stable Base needed (difficult)
")
72
Why Use Filoviruses as Bioweapon Filoviruses (Ebola in particular) –Rates of fatality –Deaths Terror of dying Ignorance of the general public –Think that they can die by being in same room with person Much not known by general physicians and scientist
 –Rates of fatality –Deaths Terror of dying Ignorance of the general public –Think that they can die by being in same room with person Much not known by general physicians and scientist")
73
Genetic Engineering At Marburg and Ebola conference talk about creation of genetically engineered Ebola virus –Volchkov of Claude Bernard University in France and Institute for Virology in Marburg –Powerful Molecular tool to analyze how these viruses cause disease. Constructed DNA Molecule (Complimentary Nucleotide sequence to Ebola) Introduced complementary sequence in cultured cell lines with genes coding for 4 key Ebola proteins Cells proceeded to make new Ebola RNA Resulting in fully infectious when transferred to new cell lines Military Definition: The creation of genetically altered viruses and/or bacteria to enhance their power as weapons Reasons for use in Filoviruses –To make the virus stronger –Mixtures Ebolapox –Smallpox is an extremely lethal virus highly contagious in the air.
 Introduced complementary sequence in cultured cell lines with genes coding for 4 key Ebola proteins Cells proceeded to make new Ebola RNA Resulting in fully infectious when transferred to new cell lines Military Definition: The creation of genetically altered viruses and/or bacteria to enhance their power as weapons Reasons for use in Filoviruses –To make the virus stronger –Mixtures Ebolapox –Smallpox is an extremely lethal virus highly contagious in the air..")
74
OPERATIONAL EFFECTIVENESS OF EBOLAPOX Produces a form of smallpox called blackpox Blackpox is the most severe type of Smallpox. In BLACKPOX infection the skin does not develop blisters Instead the skin becomes dark all over Blood vessels leak, resulting in severe internal hemorrhaging Therefore, EBOLAPOX would not only provide the Terrorist with the hemorrhages and high mortality rate of the Ebola virus, but in addition as an added bonus would incorporate into its operational effectiveness the incredibly high contagiousness of Smallpox

75
Ways to protect against Ebola Government –Biosafety Department –CDC & other agencies –Debriefing of experts –Public health education Weaponeers Public policy and preventative measures (Medha)
")
76
PREVENTING VHF EPIDEMIC Hospitalization and Isolation of Patients Quarantine Areas if Necessary Protective Measures (Gloves, Gowns, Face Shields, Masks, Eye Protection) Disinfect Bedding, Utensils, Excreta (Heat or Chemicals) Burn Used Articles
 Disinfect Bedding, Utensils, Excreta (Heat or Chemicals) Burn Used Articles")
77
Isolation Criteria Decision-making for isolation is based upon 4 main factors: 1. Potential harm to life 2. Potential harm to critical systems 3. Potential harm to property 4.Topography & meteorological considerations

78
Isolation Precautions Direct Contact with infected blood, body fluids to be avoided. Airborne transmission rare, but cannot be conclusively excluded- negative pressure room and HEPA respirator. Laboratory Precautions- BSL 4 Personal Protective Equipment Post-Mortem Practices (Kikwit And Uganda)
.")
79
Prevention and Control Reservoir remains unknown Clarify roles of GP, sGP, and other viral proteins. Multivalent vaccine needed (4 strains of Ebola) Health infrastructures strengthened especially in Africa Surveillance improved to prevent potential spread of an epidemic.
 Health infrastructures strengthened especially in Africa Surveillance improved to prevent potential spread of an epidemic..")
Similar presentations












 Ebola viruses are found in several African.>")

 is a severe, often-fatal disease in humans and nonhuman primates (monkeys,>")







. Viruses are made of genetic material (DNA or RNA) surrounded.>")


 replication of DNA viruses (2) the culture, growth and recognition of virus.>")
 Cause hemorrhagic fevers.>")