Download presentation
Presentation is loading. Please wait.

2
CASE PRESENTATION By, Dr. Syed Hunain Riaz PGR M-II JHL

3
PRESENTING COMPLAINTS Black colored stools 1 month Generalized weakness 1 month

4
HISTORY OF PRESENTING ILLNESS Ashraf, a 40 years old man, presented with a month’s history of black colored stools, with no h/o associated black colored vomiting Stools were sticky, 4-5 times a day on average, and fouls smelling No associated unconsciousness, abdominal distention, jaundice or body swellings

5
No h/o abdominal pain No h/o heartburn/pain before or after meals, no h/o regurgitation after meals, no h/o back pain after meals No h/o difficulty in swallowing

6
No h/o anorexia or weight loss appreciated by the patient No h/o any worms in stools Has previously had such an episode for which was re-admitted in LGH No h/o chest pain on rest or at exertion.

7
H/o dyspnea on exertion, no orthopnea No h/o burning or numbness of hands or feet There is h/o medication intake for pain for trauma to his spine for which he was admitted in LGH 6 months back No documentation of any multivitamin intake

8
No h/o joint pains or swellings H/o multiple tooth extractions in the past from quacks There is no h/o blood transfusions No family h/o any such disease

9
PAST HISTORY Was admitted in LGH for trauma to his spine Was unable to move his legs and developed urine and fecal incontinence Underwent spine surgery. Regained ability to move his legs Was unable to lift his feet of the ground, and the urine and fecal incontinence persisted

10
According to Xrays. He had a prosthetic vertebrae inserted in his spine, level of L5 Given routine painkillers during stay in orthopedics ward, Discharged and returned home, during his stay he did not develop any new complaints After a month, developed black colored stools, with no associated vomiting. There was no unconsciousness or fits

11
He was re-admitted in LGH, developed mild-moderate abdominal distention Diagnosed at as a case of CLD at LGH Treated and discharged

12
The malena remained settled, the abd distention also, but after two months, he again developed malena, which lasted a month before he came to JHL Non- diabetic, non-hypertensive, no h/o tuberculosis or asthma

13
FAMILY HISTORY Parents both deceased, no account on cause of death. No h/o any such disease in siblings, no family h/o tuberculosis, asthma or diabetes

14
PERSONAL HISTORY Non-smoker Non-addict

15
SOCIOECONOMIC HISTORY Has no source of income currently, after being unable to walk Low socioeconomic status

16
EXAMINATION

17
General Physical Exam Middle aged man, lying in bed, with a markedly pale look Well oriented in time place and person Urinary catheter in place and wearing a pamper

18
Pallor: + + + Cyanosis: - Clubbing: - Jaundice:- Leuconychia: - Koilonychia: - Palmar Erythema: - Dupytren’s contracture: - Lymph nodes: No clinically significant lymph nodes palpable Pedal edema: - Normal papillae on tongue, no mouth ulcers, no stomatitis

19
BP: 130/80 mm HG Pulse: 110/min, is regular Temp: Afebrile R/R: 18/min

20
GASTROINTESTINAL EXAM Abdomen protuberant with central and inverted umblilicus No prominent veins, or pulsations A surgical scar in left hypochondrium about 5 inches in length No gynaecomastia, or spider nevi

21
Abdomen non-tender Fluid appreciated in flanks ( on shifting dullnes ), otherwise gaseous distention Liver lower edge 4-5 centimeters in mid clavicular line, smooth surface, non tender and regular margins, upper border percussed in right 5 th ICS ( span about 15 cms ) Spleen palpated about 5 inches below left costal margin, non tender, smooth in consistency and regular margins Kidneys not palpable Bowel sounds audible
, otherwise gaseous distention Liver lower edge 4-5 centimeters in mid clavicular line, smooth surface, non tender and regular margins, upper border percussed in right 5 th ICS ( span about 15 cms ) Spleen palpated about 5 inches below left costal margin, non tender, smooth in consistency and regular margins Kidneys not palpable Bowel sounds audible")
23
CARDIOVASCULAR EXAM Shape of chest normal, no scars, no prominent veins, no pulsations Apex beat palpated in left 5 th ICS, normal in character Ejection systolic murmur heard, loud at aortic area

24
NERVOUS SYSTEM Higher mental functions intact Motor system in upper limbs revealed no finding Motor system in lower limb: Power:5/5 bilaterally in proximal muscles 0/5 in muscles of dorsiflexion/plantarflexion bilaterally Reflexes: Normal knee jerks bilaterally Absent Ankle jerks bilaterally Sensory system intact in all the limbs No cerebellar signs in upper limbs, could not assess in lower limbs

25
Respiratory Exam Normal shape of chest Normal chest expansion Chest moving bilaterally equally with respiration Normal vesicular breathing

26
DIFFERENTIAL DIAGNOSIS FROM THE INFO SO FAR? 1.VARICEAL BLEED WITH UNDERLYING CLD? 2.NSAID INDUCED GASTRITIS/PEPTIC ULCER? 3.STRESS ULCERS? 4.GASTRIC/SMALL INTESTINAL MALIGNANCY?

27
INVESTIGATIONS

28
Complete Blood Examination CBC: Hb: 3.2 g/dl HCT: 12.3 % RBC: 1600/mm³ WBC: 10,000/mm³ DLC: N: 55 % L: 40 % M: 3% E: 2% Platelets: 202,000/mm³

29
RBC INDICES: MCV: 76 fl MCH: 20 MCHC: 26 pg RETICS: 1.5 % RETIC INDEX: 0.16 LDH: 298 U/L

30
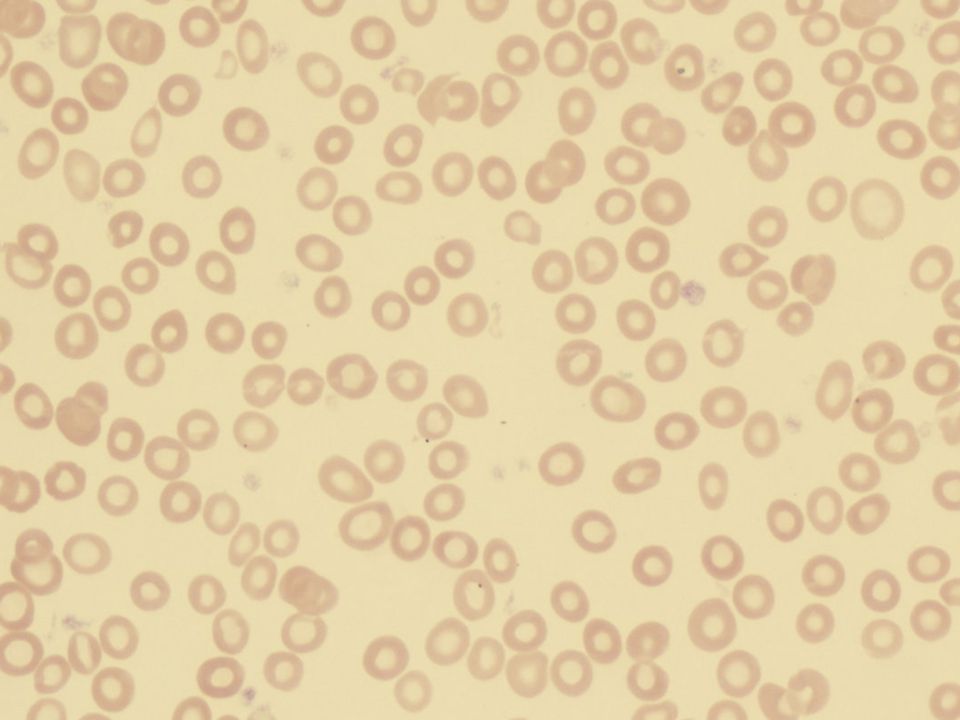
RBC MORPHOLOGY: Hypchromia: ++ Macrocytosis: ++ Poikilocytosis: ++ Anisocytosis: ++ Target cells: ++

31
STOOL EXAMINATION: + for occult blood on two occasions No ova cysts or parasites seen No presence of fat

32
URINE EXAMINATION: Normal color and pH No red blood cells or pyuria Normal urobilinogen content No presence of bilirubin

33
LFT’S: Bilirubin: 0.6 SGPT: 13 u/l Alk Phos: 212 u/l S/Albumin: 3.7 g/dl PT: 15/13 aPTT: 35/33 RFT’S: B/Urea: 21 mg/dl S/Creatinine: 0.6 mg/dl

34
USG ABDOMEN/PELVIS: Liver 16 cm’s in span, slightly coarse echotexture portal vein diameter 13 mm No focal lesion, no varices at porta-hepatis, or splenic hilum Spleen enlarged, splenic index 150 No lymph nodes or mass seen

35
S/Electrolytes: S/Na: 135 mmol/l S/K: 3.7 mmol/l S/Ca: 8.3 mg/dl S/PO4: 2.3 mg/dl VIRAL MARKERS: HBsAg: -ve by ELISA Anti-HCV: +ve by ELISA

36
Mild ascites present Small amount of interloop fluid present CXR-PA view: Normal heart size, clear angles, and no active or old lung pathology seen

37
UPPER GI ENDOSCOPY: No varices visualised at lower end of esophagus/fundus of stomach No bleed, or ulcer visualized in the stomach or 1 st or 2 nd part of duodenum No mass visualized in esophagus, stomach or duodenum

39
BONE MARROW BIOPSY: Hypercellular fragments ERYTHROPOEISIS: Hyperactive, MEGALOBLASTIC and MICRONORMOBLASTIC picture Dyserythropoesis with nuclerhexis Howell jolly bodies seen

40
LEUCOPOESIS: Active with normal maturation MEGAKARYOPOESIS: Adequate with normal maturation

41
IRON/FOLATE/B12 STUDIES Serum Ferritin: 32 ng/ml ( 32-501 ) Serum B12: 213 pg/ml ( 180-900 ) Serum Iron: 25 ug/ml ( 25-156 ) Serum Folate: 3 ng/ml ( 3-17 )
 Serum B12: 213 pg/ml ( ) Serum Iron: 25 ug/ml ( ) Serum Folate: 3 ng/ml ( 3-17 )")
42
FINAL DIAGNOSIS??? DOUBLE DEFICIENCY ANEMIA ( IRON/FOLATE AND B12 ) due to 1.Combined effect of liver disease( folate/B12def) and blood loss ( source??? )
 due to 1.Combined effect of liver disease( folate/B12def) and blood loss ( source . ).")
43
A CONUNDRUM? COULD IT BE HYPERSPLENISM???? QUERY REGARDING MYELOPDYSPLASIA????

44
IRON/ FOLATE/B12 DEFICIENCY ANEMIAS

45
IRON DEFICIENCY ANEMIA Most common anemia world wide Most common cause is GI bleed Other causes include: 1.Increased demand as in pregnancy 2.Hemoglobinuria 3.Decreased absorption

47
Daily intake almost 10-15 mg of iron Only 10 percent absorbed Presence of HYPOCHROMIC MICROCYTIC CELLS ON PERIPHERAL SMEAR ANISOCYTOSIS/POIKILOCYTOSIS HYERPCELLULAR MARROW, WITH ERYTHROID HYPERPLASIA

48
TREATMENT Oral replacement with ferrous sulfate/ ferrous gluconate I/V replacement where indicated Treatment to be continued 3-6 months after hemoglobin and indices return to normal

49
B12 DEFICIENCY ANEMIA Liver stores adequate, dietary deficiency very rare Is present in meat Takes years for deficiency to develop if with dietary deficiency

50
Other causes: 1. Decreased absorption: Achlorhydria Partial or total gastrectomy Pernicious anemia Gut infestation with fish tape worm Helicobacter pylori infection 2. Structural intestinal disease: Chron’s disease Surgical resection of gut

51
Normal B12 levels: 180-900 ng/ml PRESENTATION: Features of dorsal column tract dysfunction Peripheral neruopathy ( glove and stocking ) Sensory ataxia Psychiatric disturbances
 Sensory ataxia Psychiatric disturbances")
52
LAB FINDINGS MACRO-OVOLOCYTES ( WITH HOWEL JOLLY BODIES ) HYPERSEGMENTED NEUTROPHILS RASIED LDH RASIED INDIRECT BILIRUBIN
 HYPERSEGMENTED NEUTROPHILS RASIED LDH RASIED INDIRECT BILIRUBIN")
53
HALLMARK IS MEGALOBLASTIC BONE MARROW MULTILOBED NEUTROPHILS, METAMYLOCYTES MAY BE SEEN GIANT PLATELET PRECURSORS IN MARROW PANCYTOPENIA CAN BE PRESENT

55
DIAGNOSTIC TEST IS RASIED METHYLMALONIC ACID ( > 1000 NMOL/L)
")
56
TREATMENT I/M or oral B12 supplements in a dose of 1000 mcg/day

57
FOLIC ACID DEFICIENCY ANEMIA Present in leafy vegetables and fruits More common than B12 deficiency Causes include: Decreased intake Decreased absorption 1. Sprue 2. Drugs

58
INCREASED REQUIREMENT ( PREGNANCY ) CAN OCCUR IN ALCOHOLICS AND LIVER DISEASE INHIBITION TO ACTIVE FORM ( METHOTREXATE )
 CAN OCCUR IN ALCOHOLICS AND LIVER DISEASE INHIBITION TO ACTIVE FORM ( METHOTREXATE )")
59
PRESENTATION: 1.General symptoms of anemia 2. No Neurological dysfunction 3. Peripheral blood smear and bone marrow findings same as B12 deficiency

60
TREATMENT ORAL SUPPLEMENTATION WITH FOLIC ACID @ 1MG/DAY

Similar presentations





MRCP(LONDON) ASSOCIATE PROFESSOR MEDICINE.>")


















