Download presentation
Presentation is loading. Please wait.

1
Neonatal Jaundice Dezhi Mu MD/PhD
Department of Pediatrics, West China Second University Hospital, Sichuan University

2
Introduction Jaundice is quite common (5mg/dl).
Full term infants: at least 50% Preterm infants: over 80% Elevated blood bilirubin levels: 97%

3
Introduction continued
When? in the first week of life Where? skin , mucosa and white of eye How many? blood bilirubin concentrations is ≥5-7mg/dl.

4
Introduction continued

5
Why Jaundice occurred? Producing Excreting

7
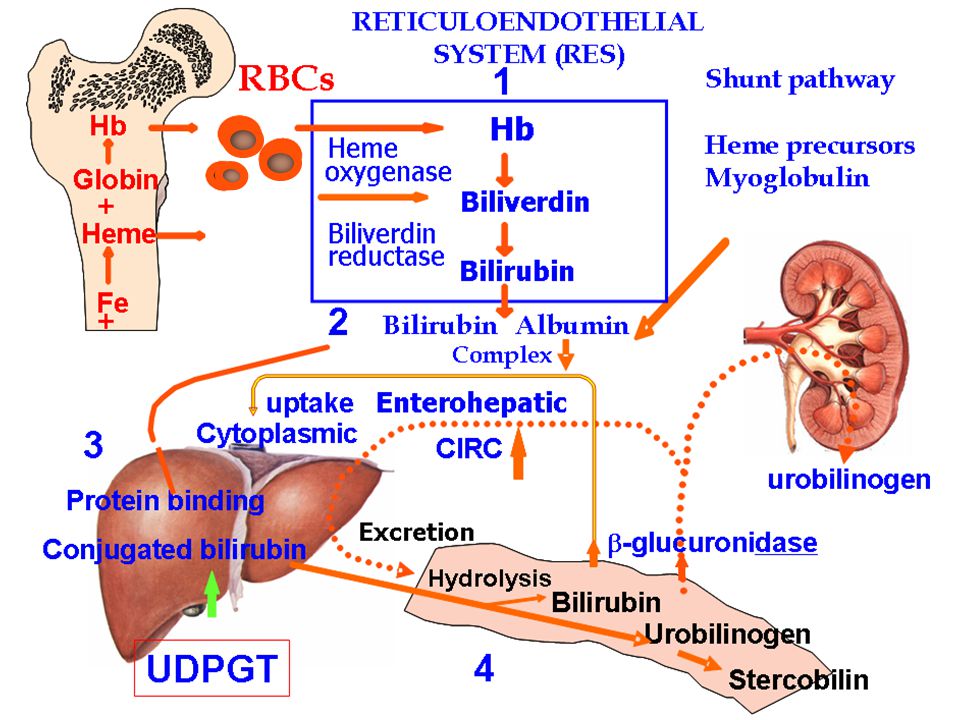
Bilirubin Metabolism:
1. RBC: Heme bilirubin (UCB) 2. Blood: carried by bound to albumin 3. Liver: uptaken : Y protein, Z protein conjugated: UDPGT excreted: to the biliary system 4. Intestine: stercobilins -glucuronidase enterohepatic circulation
 2. Blood: carried by bound to albumin. 3. Liver: uptaken : Y protein, Z protein. conjugated: UDPGT. excreted: to the biliary system. 4. Intestine: stercobilins. -glucuronidase enterohepatic. circulation.")
8
The metabolic characteristics of bilirubin in newborns:
1. Bilirubin production 8.8mg/Kg/d in newborns 3.8mg/Kg/d in adults 2. Bilirubin-albumin complex formation a. preterm infant; b. acidosis

9
The metabolic characteristics of bilirubin continued
3. Bilirubin metabolism of hepatocyte a. Hepatic uptake of bilirubin b. Bilirubin conjugation: UDPGT (uridine diphosphate glucoronyl transferase) c. Defective bilirubin excretion ability to bile system 4. Enterohepatic circulation
 c. Defective bilirubin excretion. ability to bile system. 4. Enterohepatic circulation.")
10
Bilirubin toxicity 1. Conjugated bilirubin water-soluble
2. Unconjugated bilirubin lipid-soluble bilirubin-encephalopathy (kernicterus)
")
11
Clinical Manifestations
Jaundice appears When: at any time during the neonatal period Where: from face chest abdomen feet

12
Manifestations continue
Evaluation of jaundice : 1. By eyes: face, 5mg/dl ( 85μmol/L ); abdomen, 10-15mg/dl; feet, 15-20mg/dl ; 2. By transcutaneous measurement : used for screening 3. By serum levels : standard
; abdomen, 10-15mg/dl; feet, 15-20mg/dl ; 2. By transcutaneous measurement : used for screening. 3. By serum levels : standard.")
13
Manifestations continue
Classification: Physiological Jaundice Pathological Jaundice

14
Manifestations continue
Physiological jaundice : 1. General state is well 2. Appears 2-3days (>24h of age) peaks < 12.9mg/dl (full term infants) <15mg/dl (preterm infants) fades <2 week (term infants) <4 weeks (preterm infants) 3. Accumulates <5mg/dl/d 4. Direct bilirubin <2mg/dl
 peaks < 12.9mg/dl (full term infants) <15mg/dl (preterm infants) fades <2 week (term infants) <4 weeks (preterm infants) 3. Accumulates <5mg/dl/d. 4. Direct bilirubin <2mg/dl.")
15
Manifestations continue
Pathological Jaundice 1. Appears earlier (first 24 hours of life) 2. Peaks >12.9mg/dl (full term infants) >15mg/dl (preterm infants) Fades >2 weeks (term infants) >4 weeks (preterm infants) 3. Accumulates >5mg/dl/d 4. Direct bilirubin >2mg/dl 5.Jaundice recurrent
 2. Peaks >12.9mg/dl (full term infants) >15mg/dl (preterm infants) Fades >2 weeks (term infants) >4 weeks (preterm infants) 3. Accumulates >5mg/dl/d. 4. Direct bilirubin >2mg/dl. 5.Jaundice recurrent.")
16
Common causes of pathological jaundice
1. Unconjugated bilirubinemia: a. hemolytic diseases: ABO, Rh incompatibility b. G-6-PD deficiency; c. Breast milk jaundice

17
Causes of pathological jaundice continue
2. Conjugated bilirubinemia: a. Neonatal hepatitis b. Biliary obstruction (cholestatic jaundice) biliary atresia, common bile duct stenosis c. Congenital metabolic diseases α-1 antitrypsin deficiency
 biliary atresia, common bile duct stenosis. c. Congenital metabolic diseases. α-1 antitrypsin deficiency.")
18
Hemolytic disease of newborn
ABO: 85.3% Rh : 14.6% MN : 0.1%

19
Hemolytic disease of newborn continued
ABO incompatibility the mother: type O the infant: type A or B Rh incompatibility the mother: Rh(-) the infant: Rh(+)D,E,C,d,e,c
 the infant: Rh(+)D,E,C,d,e,c.")
20
Pathogenesis

21
Pathophysiology Red blood cell breakdown Hyperbilirubinemia Anemia
Jaundice Liver Spleen Heart, other organs Hydrops Kernicterus Seizures etc.

22
Clinical Manifestations:
ABO Rh 1.Jaundice : mild severe 1-2 day h 2.Anemia: mild severe (3-6 weeks) heart failure 3.Hepato rare common splenomegaly
 heart failure. 3.Hepato- rare common. splenomegaly.")
23
Complication Kernicterus: Phase 1: decreased alertness Hypotonia
Poor feeding Phase 2: Hypertonia, Retrocollis, opisthotonus Phase 3: Hypotonia

24
Laboratory tests: 1. Blood type incompatibility
2. Hyperbilirubinemia : Unconjugated bilirubin level 3. Hemolytic tests 1). Hemoglobin level : low 2). Reticulocytes:10–15% 3). Nucleated RBC
. Hemoglobin level : low. 2). Reticulocytes:10–15% 3). Nucleated RBC.")
25
Laboratory tests continued
Antibody test 1). Direct Coombs test (+) confirm 2). Antibody release test (+) confirm 3). Free antibody test (+) judge
. Direct Coombs test (+) confirm. 2). Antibody release test (+) confirm. 3). Free antibody test (+) judge.")
26
Treatments 1). Phototherapy 2). Exchange transfusion
3). Internal Medicine
. Internal Medicine.")
27
Treatments continued During pregnancy
1. Intrauterine blood transfusion 2. Early delivery

28
Treatments continued After birth 1. Phototherapy
Principle : photon of light Three photochemical reactions: 1). Structure isomer 2). Geometric isomer 3). Photo-oxidation Photoproducts excretion: w/o conjugation
. Structure isomer. 2). Geometric isomer. 3). Photo-oxidation. Photoproducts excretion: w/o conjugation.")
29
Treatments continued Indications of phototherapy : Light source:
Unconjugated bilirubinemia Bilirubin level >12mg/dl Light source: Spectral outputs 420 to 500nm

30
Treatments continued Side effects of phototherapy : a. diarrhea
b. fever c. skin rash d. bronze baby syndrome (conjugated bilirubin>4mg/dl)
")
33
Treatments continued 2. Exchange Transfusions:
a. Severe hemolytic disease b. Refractory to phototherapy

34
Treatments continued Aims of transfusions: a. Remove antibodies
b. Remove bilirubin c. Correct anemia

35
Treatments continued Indication of transfusions: one of the follows
20mg/dl (340 μmol/L) >4mg/dl,Hgb<120g/L, edema 0.7mg/dl/h Kernicterus
 >4mg/dl,Hgb<120g/L, edema. 0.7mg/dl/h. Kernicterus.")
36
Treatments exchange transfusions
Source of the blood mother newborns For Rh: Rh ABO incompatibility For ABO: “AB” plasma “O” cells incompatibility packed RBC

37
Treatments exchange transfusions
Potential complications: a. Infection b. Necrotizing enterocolitis NEC c. Thromboembolic complications

38
Treatments continued 3. Pharmacological agents: a. Phenobarbital
Effects: Uptake, Conjugation Excretion b. Albumin c. IVIG

39
Preventions For ABO incompatibility: No For Rh incompatibility
300 μg of human anti-D globulin within 72 h of delivery.

40
1.Unconjugated bilirubinemia:
a. Hemolytic diseases: ABO, Rh incompatibility b. G-6-PD deficiency; c. Breast milk jaundice

41
1.Unconjugated bilirubinemia:
b. G-6-PD deficiency; male, jaundice, enzyme activity c. Breast milk jaundice causes: unclear, -glucuronidase follows physiologic jaundice: 4-7 d breast feeding persist for several weeks.

42
Conjugated bilirubinemia:
a. neonatal hepatitis b. biliary obstruction (cholestatic jaundice) biliary atresia, common bile duct stenosis c. congenital metabolic diseases α-1 antitrypsin deficiency
 biliary atresia, common bile duct stenosis. c. congenital metabolic diseases. α-1 antitrypsin deficiency.")
43
Case analysis : 24 old male infant, gravida1,para 1.
Apgar scores: 8 at 1 min Mother: blood type “O” PE: icterus appeared on face and trunk skin liver edge 1cm palpable spleen tip

44
Case analysis continued
Lab tests: Hgb:13g/dl, reticulocyte count : 7% Blood smear: nucleated RBC Blood type: A, Rh-positive Serum bilirubin: 12.9mg/ml Direct Coomb’s test: weakly positive Question: what’s the risk factor ?

45
Department of Pediatrics
Thank you! Questions?

Similar presentations















 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")





