Download presentation
Presentation is loading. Please wait.

1
Dr Sam Gausden FY2 February 2015 Inflammatory bowel disease

2
Contents/aims/objectives Definition Presentation Investigations Management Clinical scenario Explanation station

3
Definition

4
Umbrella term

5
Definition Umbrella term Chronic

6
Definition Umbrella term Chronic Relapsing-remitting

7
Definition Umbrella term Chronic Relapsing-remitting Acute non-infectious inflammation

8
Differences

9
Distribution

10
Differences

11
Distribution Smoking

12
Smoking in IBD 2/3 Crohn’s pts are smokers and cessation halves relapse 95% of UC pts are non- smokers or ex-smokers

13
Smoking in IBD YOU SEE people smoking with UC Smoking in Crohn’s makes you want to GROAN

14
Differences Distribution Smoking Histology

15
UC histology

16
Hyperaemic/haemorrhagic colonic mucosa Pseudopolyps Usually on affects mucosal layer Absence of goblet cells

17
Crohn’s histology Transmural granulomatous inflammation Cobblestoning MACROSCOPICALLY: Strictures, abscesses, fistulae, skip lesions

18
Systemic manifestations

19
Hepatic - autoimmune hepatitis (UC), gallstones (Cr), PSC (UC)
, gallstones (Cr), PSC (UC)")
20
Systemic manifestations Hepatic Other - VTE, osteoporosis (Cr), amyloidosis (Cr )
, amyloidosis (Cr )")
21
Systemic manifestations Hepatic Other Rheum - arthritis, sacro-ileitis, AS

22
Systemic manifestations Hepatic Other Rheum Skin – EN and PG (UC>Cr)
")
23
Systemic manifestations Hepatic Other Rheum Skin Eyes – iritis, uveitis

24
Eyes Uveal tract = iris, ciliary body and choroid

25
Systemic manifestations H epatic O ther R heum S kin E yes

26
Symptoms - UC

27
Diarrhoea + blood/mucous Faecal urgency/incontinence Tenesmus Lower abdominal pain Tiredness/malaise Weight loss/failure to thrive or grow Fever

28
Symptoms – Crohn’s

29
Symptoms - Crohn’s Diarrhoea +/- blood/mucous Malabsorption Abdominal pain (crampy) Mouth ulcers Bowel obstruction Fistulas (perianal) Abscesses (perianal/intrabdominal ) Tiredness/malaise Weight loss/failure to thrive or grow Fever
 Mouth ulcers Bowel obstruction Fistulas (perianal) Abscesses (perianal/intrabdominal ) Tiredness/malaise Weight loss/failure to thrive or grow Fever")
30
Signs - UC

31
Clubbing Pallor Eyes Legs Abdominal tenderness PR

32
Signs – Crohn’s

33
Clubbing Pallor Eyes Mouth Legs Abdominal tenderness Mass in RIF PR – skin tags, abscesses, fistulas

34
Investigations

35
Bedside tests

36
Faecal calprotectin Protein common in neutrophil cytoplasm Bacteriostatic and resistant to enzyme degredation NICE guideline: 1) To differentiate IBD from IBS in pts where cancer is NOT suspected Also: can also be used to evaluate IBD Rx and predict flares
 To differentiate IBD from IBS in pts where cancer is NOT suspected Also: can also be used to evaluate IBD Rx and predict flares")
37
Blood tests

38
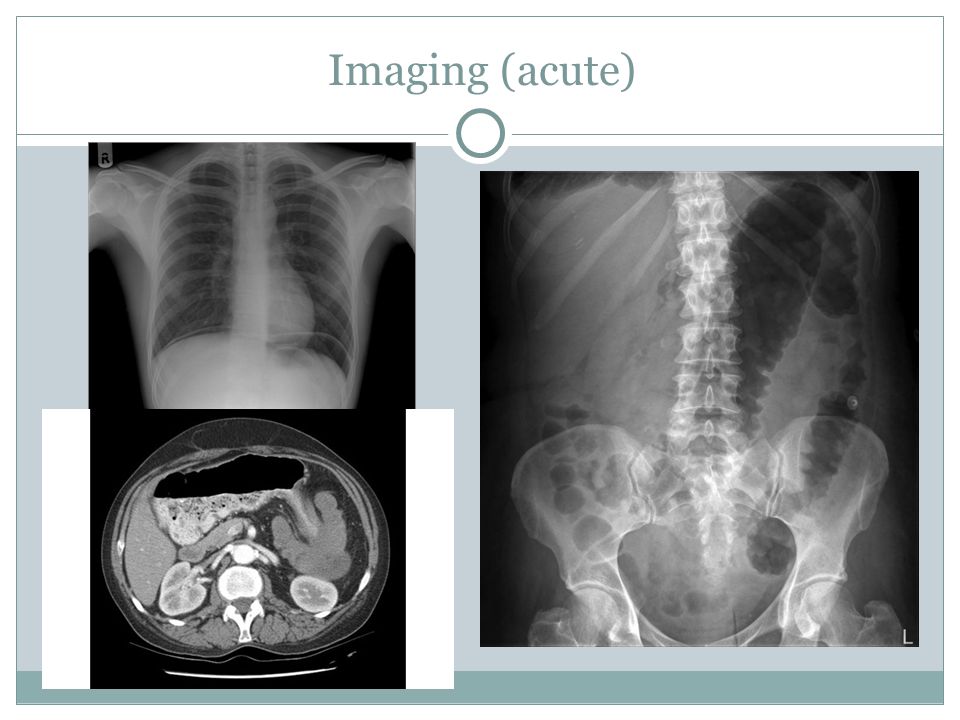
Imaging (acute)
")
40
Special test (acute)
")
41
Special tests (acute)
")
42
Management (long-term)
")
43
Conservative

45
Inducing remission in mild-mod UC 1

46
1) Aminosalicylates 2) Steroids 3) Immunosuppression (tacrolimus)
 Aminosalicylates 2) Steroids 3) Immunosuppression (tacrolimus)")
47
Inducing remission in severe UC (inpatient) 1
 1")
48
1) IV steroids 2) Immunosuppression (ciclosporin) 3) Biologics (infliximab)
 IV steroids 2) Immunosuppression (ciclosporin) 3) Biologics (infliximab)")
49
Assessing UC severity

50
TRUELOVE AND WITTS’ CRITERIA 1

51
Inducing remission in Crohn’s 1

52
1) Steroids (oral or IV) 2) Aminosalicylates (2 nd line) 3) Immunosuppressants (aza, mercapto, methotrexate) 4) Biologics (infliximab or adalimumab)
 Steroids (oral or IV) 2) Aminosalicylates (2 nd line) 3) Immunosuppressants (aza, mercapto, methotrexate) 4) Biologics (infliximab or adalimumab)")
53
Maintaining remission in UC

54
1) Aminosalicylates 2) Immunosupressants (aza or mercapto)
 Aminosalicylates 2) Immunosupressants (aza or mercapto)")
55
Maintaining remission in Crohn’s

56
1) Immunosupressants (aza, mercapto or MTX) 2) Continue biologics 3) OR nothing
 Immunosupressants (aza, mercapto or MTX) 2) Continue biologics 3) OR nothing")
57
Surgery Indications Incidence

58
Prognosis Ca colon risk with UC approx. 15% over 20yrs with pancolitis Colonoscopy screening (after 1-5 years depending on risk)
.")
59
Scenario time 29 year old female PC: Diarrhoea HPC: 1/12 Hx 12x day now Blood and mucous mixed in Cramping LIF pain Unwell and lethargic

60
On examination Temp: 38.2C Soft Abdomen, slightly distended Tender in LIF PR exam very painful and reveals fresh blood and mucous on the glove Diagnosis?

61
On examination Temp: 38.2C Soft Abdomen, slightly distended Tender in LIF PR exam very painful and reveals fresh blood and mucous on the glove Diagnosis? Acute flare of UC

62
Differential diagnoses?

63
Infection Inflammation Neoplastic Vascular Drugs

64
Acute investigations?

65
Stool culture, pregnancy test FBC, U&Es, LFTs, CRP, ESR, clotting, G&S Erect CXR, AXR, CT abdomen ?flexi sigmoidoscopy

66
Long-term investigation?

67
Colonoscopy + biopsy Colonoscopic surveillance

68
Initial acute management

69
A-E approach NBM, IVI, transfusion depending on Hb IV hydrocortisone +/- rectal steroids If getting better – transfer to oral pred and 5-ASA If getting worse – consider ciclo/infliximab/surgery

70
Long term management

71
Aminosalicylates Azathioprine or mercaptopurine

72
Comparing Crohn’s and UC Clinical presentation Histological findings? Smoking?

73
Recap Scoring system for UC severity? Extra-intestional manifestations of IBD?

74
Explanation station Please explain a colonoscopy to the patient

75
Explanation station Check patient’s understanding Think about patient’s experience Why we do it and risks No jargon Any questions Leaflet

76
Always remember for IBD Ask about eyes, joints and skin Only ever do flexi sig in an acute flare If in doubt over diagnosis, say IBD Know difference between ileostomy and colostomy Test for TB before starting infliximab Any questions?

77
References 1) http://www.nice.org.uk/guidance/conditions- and-diseases/digestive-tract- conditions/inflammatory-bowel-disease
 and-diseases/digestive-tract- conditions/inflammatory-bowel-disease")
Similar presentations












 FY1 WARWICK A&E Inflammatory Bowel Disease.>")



 that causes a long- lasting inflammation in your digestive tract.>")


 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")
