Download presentation
Presentation is loading. Please wait.

3
REFRACTIVE SURGERY Refractive surgical techniques have evolved rapidly over the past three decades. Emerging as safer and more reliable means of treating myopia, hyperopia and astigmatism,thus reducing the need for corrective lenses Although a wide range of refractive procedures exists, we will discuss the following refractive procedures : ....

4
A) Radial keratotomy. B) Excimer laser photorefractive keratectomy ( PRK ) C) Laser assisted in situ keratomiliuses (LASIK) D) Laser assisted subepithelial keratomiliuses ( LASEK ) E) Laser thermokeratoplasty (LTK ) D) Intracorneal ring segments (ICRS) G) Phakic intraocular lenses (IOLs )
 Excimer laser photorefractive keratectomy ( PRK ) C) Laser assisted in situ keratomiliuses (LASIK) D) Laser assisted subepithelial keratomiliuses ( LASEK ) E) Laser thermokeratoplasty (LTK ) D) Intracorneal ring segments (ICRS) G) Phakic intraocular lenses (IOLs ).")
5
History of keratorefractive surgery Radial keratotomy to correct myopia was introduced in Japan in the 1940s using anterior and posterior corneal incisions. This approach fell into disfavor 10 to 20 years later when resulting endothelial cell injury led to irreversible corneal oedema. Russian investigators improved the procedure in the 1970s by using only anterior incisions.

6
Since it's introduction to the United States in 1978, RK underwent continual refinement,but long term studies showed significant instability and progressive hyperopic shifts that led to virtual abandonment of this surgical procedure in the late 1990s. Excimer laser which makes pulses of invisible ultraviolet light of 193 nm,each pulse of light can removes a microscopic layer from the front surface of the cornea, was introduced in ophthalmology to reshape the anterior corneal surface.

7
Early excimer laser was used in the PRK operation, establishing it's efficacy for the correction of myopia, hyperopia, and astigmatism.later excimer laser was used in the operations of LASIK,LASEK and LTK. The preoperative evaluation is of great importance in these circumstances, like patient selection,motivation, contraindications,physical and ocular examination,cycloplegic refraction, and screening tests like pachymetry, keratometry and computerized videokeratograohy.

8
We will discuss now the main refractive procedures according to it's development : 1) Radial Keratotomy (RK ): Refers to the placement of deep paracentral and peripheral incisions in the cornea,producing central corneal flattening and thus reducing the central refractive power and myopia.
 Radial Keratotomy (RK ): Refers to the placement of deep paracentral and peripheral incisions in the cornea,producing central corneal flattening and thus reducing the central refractive power and myopia.")
10
RK is best for low myopia ( -2.00 TO -3.00 D.) The procedure has the advantage of being safe,with rapid results and high predictability in the low range of myopia. Incisions are ideally 80% to 90% of corneal depth, and should not extend to Descement membrane to avoid the danger of mechanical instabilita and perforation. In general no more than eight radial cuts was done with a 3.0 mm central clear zone

11
2) Astigmatic keratotomy : constitutes the placement of transverse or arcuate incisions perpendicular to the steepest corneal meridian to correct astigmatism, the incised meridian flattens while the meridian 90 degrees away steepens by nearly the same amount.Incisions are ideally between 5 and 7mm from the pupil center.
 Astigmatic keratotomy : constitutes the placement of transverse or arcuate incisions perpendicular to the steepest corneal meridian to correct astigmatism, the incised meridian flattens while the meridian 90 degrees away steepens by nearly the same amount.Incisions are ideally between 5 and 7mm from the pupil center.")
12
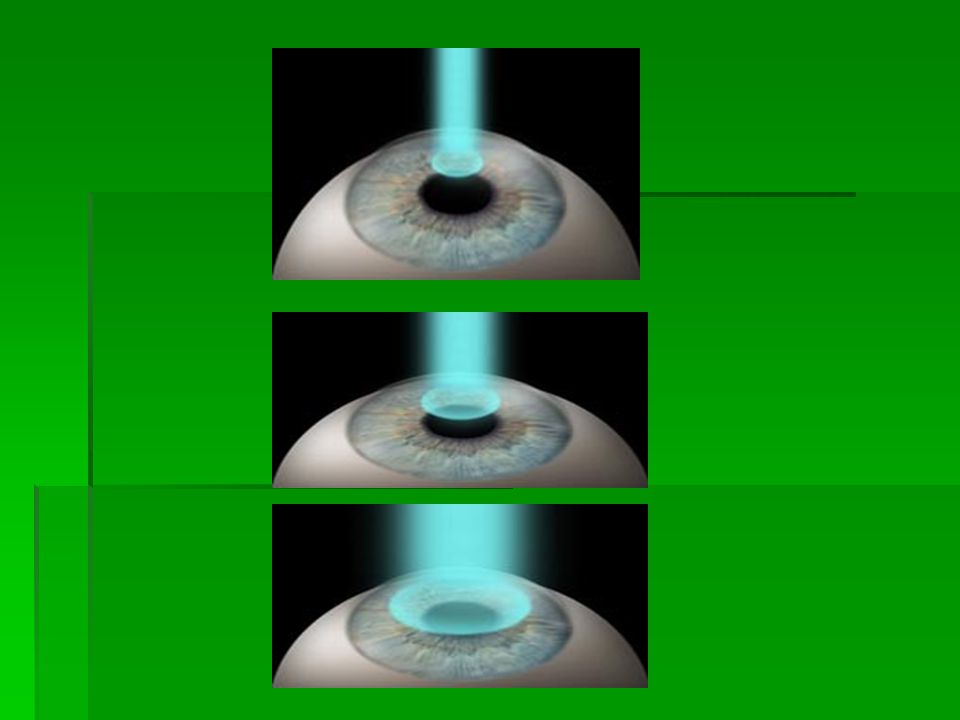
3) Excimer laser PRK : Photorefractive keratectomy uses the cool beam of the excimer laser to reshape the front of the eye by treating the surface of the cornea so that the rays focus more sharply on the retina. The outer surface of the cornea, called epithelium, must be removed, this is accomplished by carefully scraping it away. The laser is then applied directly to Bowman membrane and anterior corneal stroma to remove microscopic amounts of these tissues measured in microns.

14
The epithelium grows back over the treated area within several days. A (bandage ) contact lens is placed on the eye to minimize discomfort during this healing period. Complete healing and visual recovery can take as long as 3-6 months with PRK. RESULTS : In FDA Phase III trials for PRK in low myopia (-1 to -6 D),88 to 92% of patients had uncorrected vision of 20/40 or better at 1 year with 50 to 60% better than or equal to 20/20, and 70 to 80% within 1.0 D of the intended refraction.
 contact lens is placed on the eye to minimize discomfort during this healing period. Complete healing and visual recovery can take as long as 3-6 months with PRK. RESULTS : In FDA Phase III trials for PRK in low myopia (-1 to -6 D),88 to 92% of patients had uncorrected vision of 20/40 or better at 1 year with 50 to 60% better than or equal to 20/20, and 70 to 80% within 1.0 D of the intended refraction..")
15
Excimer laser PRK for higher levels of myopia is somewhat less predictable. LASIK has virtually replaced PRK for the treatment of hyperopia and higher degrees of myopia.

16
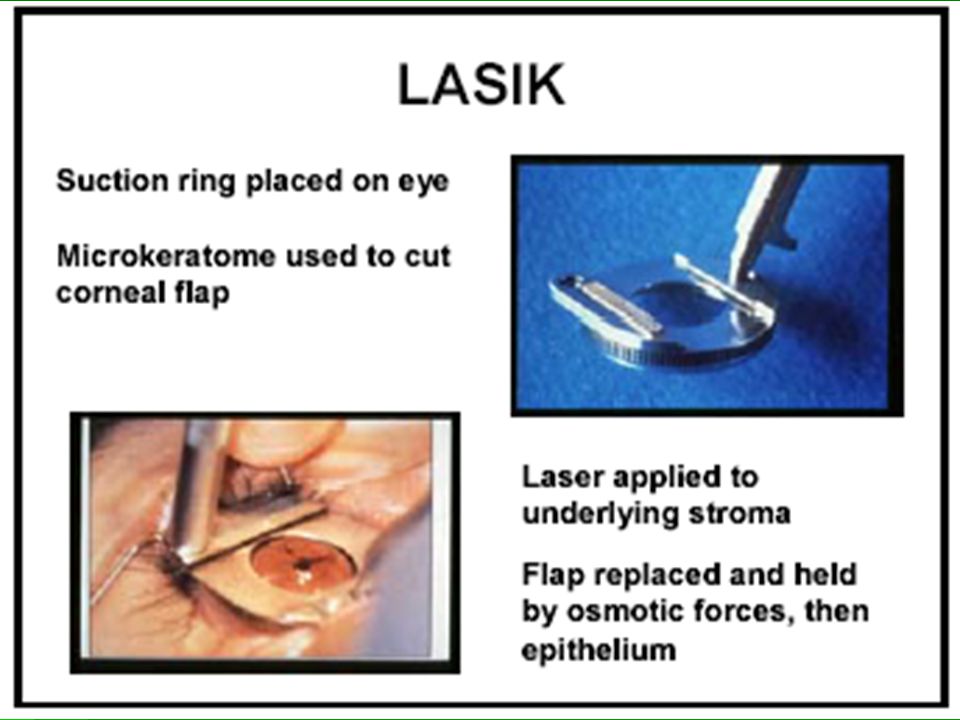
4) LASIK( Laser assisted in-situ Keratomileusis Is a refractive surgical procedure that results in rapid recovery of vision and has the capability to benefit patients with myopia, hyperopia, and astigmatism. Millions of people worldwide have already this exciting and marvelous procedure. Candidates must be at least 18 years of age. In this procedure the eye surgeon creates a thin surface flap of the cornea using a microkeratome to expose the underlying tissues ( stromal bed ) in which the surgeon applies the excimer laser beam to create the refractive ablation. Once the laser ablation is completed, the surgeon gently replaces the corneal surface flap to restore surface integrity of the eye.
 in which the surgeon applies the excimer laser beam to create the refractive ablation. Once the laser ablation is completed, the surgeon gently replaces the corneal surface flap to restore surface integrity of the eye..")
19
The results are often dramatic and very rapid, with most patients seeing well enough to drive a car without correction the very next day. However, the best post-operative visual acuity may not be obtained until 2 to 3 weeks, or in some cases, even a few months after the procedure. Visual results with LASIK : LASIK nearly always results in improved vision without correction.However LASIK is an imperfect procedure, and does not always result in 20/20 or even 20/40 visual acuity.

20
Patients in the extreme range of myopia generally have less favorable outcomes with LASIK. In a study results of the American Society of Cataract and Refractive Surgery from 1736 eyes with myopia and myopic astigmatism that underwent LASIK operation, they showed the following results : Post-op 1 month 3 months 6 months 20/20 or better 45% 46% 50% 20/40 or better 87% 89% 93%

21
The best candidate for LASIK is an individual who desires to be less dependant on glasses or contact lenses, is willing to accept the risk of the procedure, and understands that an enhancement procedure may sometimes be required. We now know that dry eye syndrome commonly follows LASIK procedures, at least transiently. This make the patient feels dry or gritty or even blurring vision. Many surgeons advise using non- preserved artificial tears for the first few weeks after LASIK.

22
5) LASEK(Laser Subepithelial Keratomileusis ) LASEK is a relatively new procedure that sits somewhat between LASIK and PRK,is used mostly for people with corneas that are too thin or too flat for LASIK. It was developed to reduce the chance of complications that occur when the flap created during LASIK is not of the ideal thickness or diameter. In LASEK instead of using a microkeratome, a blade called a trephine is used

23
LASEK is a procedure that takes about the same amount of time as LASIK. A topical anesthetic is applied to the eye, then the trephine is used to create the epithelium flap. After the flap is made, the surgeon covers the eye with a dilute alcohol solution (20% ). The solution loosens the edges of the epithelium. After the eye has been soaked for roughly 30 seconds, the surgeon uses a tiny hoe to peel back the epithelium and fold it back so it is out of the way.
. The solution loosens the edges of the epithelium. After the eye has been soaked for roughly 30 seconds, the surgeon uses a tiny hoe to peel back the epithelium and fold it back so it is out of the way..")
24
At this point the doctor employs an excimer laser in the same way as in LASIK or PRK,and molds the corneal tissue to the desired shape. After the shaping is finished, the surgeon replaces the epithelium flap. The recovery time for LASEK is slightly longer than it is for LASIK, as it takes approximately 4 to 7 days to recover good vision.The flap itself heals within a day, but the eye can still feel irritated for up to three days.

27
6) Thermokeratoplasty : Consists of heating the cornea to shrink the peripheral and paracentral stromal collagen to produce a peripheral flattening and a central steepening of the cornea to treat HYPEROPIA. Solid state infrared lasers, such as the holmium:yttrium,aluminum, and garnet (Ho:YAG ) laser of 480-530nm,have been used in a peripheral intrastromal radial pattern ( Laser Thermokeratoplasty ), to treat hyperopia of 2.50D.and less.
 laser of nm,have been used in a peripheral intrastromal radial pattern ( Laser Thermokeratoplasty ), to treat hyperopia of 2.50D.and less..")
29
7) Another form of thermokeratoplasty is the so called ( Conductive Keratoplasty ) which used a handheld radiofrequency probe to shrink the peripheral collagen. The shrinkage temperature of the corneal collagen is between 55-58 degrees. Despite the instability of corrections and regressions, laser thermokeratoplasty and conductive keratoplasty have the major advantage of untouched the central cornea.

30
8) Intracorneal ring segments (ICRS): ICRS are placed in the peripheral cornea and act by compressing the peripheral cornea and changing the radius of curvature of the central cornea. When the anterior surface of the cornea is lifted focally over the ring, a compensatory flattening of the central cornea occur for treatment of myopia.ICRS are threaded into a peripheral midstromal tunnel

32
A potential advantage of intracorneal segments over other refractive surgical techniques is reversibility. The main drawback is the limited range of correction ( up to -3D )in myopia and ( up to +2D ) in hyperopia. There are another new approaches to refractive surgery like :
in myopia and ( up to +2D ) in hyperopia. There are another new approaches to refractive surgery like :.")
33
1) Refractive lensectomy : The extraction of the clear lens in the correction of high myopia, originally performed in 1890, was later abandoned because of an unacceptable high rate of complications. With more recent operative techniques, such as phacoemulsification, and better IOLs, there has been renewed interest in managing high refractive errors by clear lens extraction. One drawback of this procedure is the loss of accomodation.The use of accommodating or multifocal IOLs could obviate this problem.

34
2) Phakic intraocular lenses : --Anterior chamber phakic IOL, named as iris claw lens to correct high myopia in phakic patients, enclaved in the midperipheral iris. Long term follow- up has reported progressive pupil ovalization with an older model. -- Posterior chamber phakic IOL, it must accommodate to the space between the posterior iris and the crystalline lens. If it vaults too much, pigment dispersion and even pupillary block glaucoma could result.If it lies against the anterior surface of the crystalline lens, cataract could result.

35
3) Gel injection adjustable keratoplasty : Consist in injecting gel in the paracentral corneal stroma in order to flatten the central cornea and reduce myopia. The gel was extremely well tolerated with no evidence of inflammation.It can correct myopia above 5 or 6 diopters as well as astigmatism. What is most exciting about this procedure is that it make it possible to adjust patients, refractive errors throughout their lives. Gel can either be added or removed

36
4) Procedures that modify the axial length of the eye either by resection of the sclera or by reinforcement of the posterior pole in case of high myopia,have had a greater role in the management of staphyloma than in the management of the patient's refractive error. 5) Customized corneal ablation through Wavefront mapping : This is accomplished by mapping the profile of the whole eye through wavefront sensing devices, this sophisticated method identifies abberations in the entire optical system and not only the corneal surface. With the use of advanced lasers and wavefront deformation measuring devices, the correction of these distortions of the human eye will continue to gain widespread use.
 Customized corneal ablation through Wavefront mapping : This is accomplished by mapping the profile of the whole eye through wavefront sensing devices, this sophisticated method identifies abberations in the entire optical system and not only the corneal surface. With the use of advanced lasers and wavefront deformation measuring devices, the correction of these distortions of the human eye will continue to gain widespread use..")
Similar presentations