Download presentation
Presentation is loading. Please wait.

1
Orthopedic review 930-943

2
930

3
931 reconstructive ladder A term coined by reconstructive plastic surgeons to describe levels of increasingly complex management of wounds Rung 1: healing by secondary intention Rung 2: primary closure Rung 3: delayed primary closure Rung 4: split thickness graft Rung 5: full thickness skin graft Rung 6: tissue expansion Rung 7: random pattern flap Rung 8: pedicled flap Rung 9: free flap D. E. Boyce Reconstructive surgery 2006

4
932

5
933 Operative sequence for digital and hand replantation: Locate and tag the vessels and nerves Debride Shorten and fix the bone Repair the extensor tendons Repair the flexor tendons Anastomose the arteries Repair the nerves Anastomose the veins Obtain skin coverage

6
934 Z-plasty Basic pattern: Z with limbs of equal length, with the peripheral limbs forming an angle of 60° with central limb Check length of limb of Z Green’s operative hand surgery 4 th ed 1999

7
935 Campbell 2007 11th ed Vol 4

8
936 skin graft The thicker the skin graft, the poorer quality of donor site The thicker portion of body, as posterolateral aspects of trunk and thigh, afford the best chance of good healing The thinner areas, as inner aspect of thigh, are generally unsuitable for donor site; poor healing and tendency of skin graft to hyperpigment in its new area Most wounds area best covered by grafts 0.015 inch in thickness Graft > 0.018 inch are seldom indicated due to donor site morbidity The thicker the skin graft, the more hair follicles in the graft; a relatively hairless area should be selected as a donor site for hand Green’s operative hand surgery 4 th ed 1999

9
937 skin graft When the graft is expected to be permanent, “the thicker the graft, the better the function.” Free skin grafts are to be obtained, “the thinner the graft, the better the take” A thick graft is better able to withstand friction and constant use than a thin one and contracts only about 10%; Thin graft may contract 50% to 75% Campbell 11th ed 2007

10
938 FTSG V.S. STSG Split-thickness skin grafts (STSGs): Contain epidermis and a portion of dermis 12 to 18/1000-inch thickness Thinner grafts require less nutrients to remain viable, contract more when healing Full-thickness skin grafts (FTSGs): Epidermis and dermis Better color match, texture, contour, and less contracture but decreased success rates compared to STSGs Sabiston 17th ed 859
: Contain epidermis and a portion of dermis 12 to 18/1000-inch thickness Thinner grafts require less nutrients to remain viable, contract more when healing Full-thickness skin grafts (FTSGs): Epidermis and dermis Better color match, texture, contour, and less contracture but decreased success rates compared to STSGs Sabiston 17th ed 859.")
11
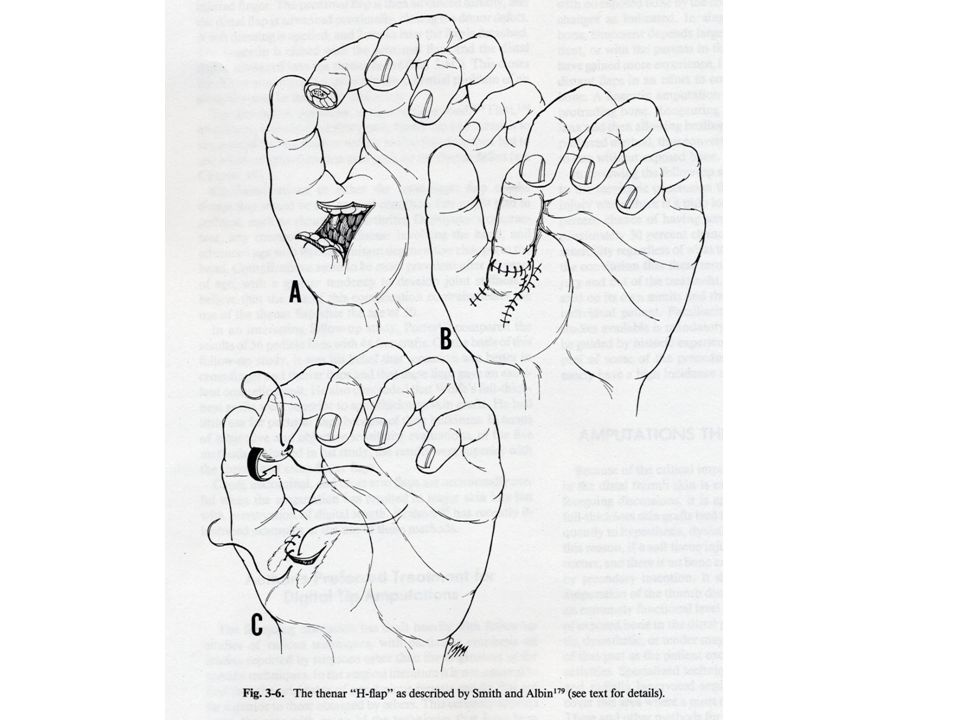
939 thenar flap Thenar H-flap When length preservation is important and other flaps not appropriate For index & long, ulnar digits won’t reach With thumb held in abduction, flex injured finger so that its tip touches the middle of the thenar eminence At 2 weeks, the base of the flap is detached Complications: flexion contracture, scar at donor area Green’s operative hand surgery 4th ed 1999

13
940 rotation flap All rotation flaps are random pattern The flap should be made as large as is reasonably possible; “Think of a flap and then double it” Burow’s triangle: normal skin excised to facilitate movement of a flap Green’s operative hand surgery 4th ed 1999

14
Burow’s triangle

15
Back-cut On flap side of incision Length of rotation flap side has been increased by twice the length of back-cut

16
941 regional flap Regional flaps derive from tissues not immediately adjacent to the primary defect but from its vicinity 2 type: random and axial pattern Axial flap require one surgical procedure Random flap require at least 2: 1 st,flap is raised and applied to the primary defect, 2 nd, pedicle is divided and inset Cross finger flap, thenar flap, neurovascular island flap Green’s operative hand surgery 4th ed 1802

17
942 groin flap A axial pattern flap Axial vessel: superficial circumflex iliac artery and vein An area with sparse hair distribution

18
943 Groin Flap 優點 Advantages : Potentially large size Location in an area with sparse hair distribution Minimal donor site morbidity Multiple arterial and venous systems Potential for incorporating bone with the overlying skin Applications as a traditional pedicle flap before the development of microvascular surgical techniques Campbell 2007 11th ed Vol 4

20
944-958

21
944 Groin Flap 缺點 Disadvantages: Potential excessive thickness in obese patients Problems with color matching Short vascular pedicle Difficulty in dissection of the vessels Lack of satisfactory innervation Likelihood that previous surgical procedures in the inguinal region might have damaged the essential vessels Campbell 2007 11th ed Vol 4

22
945 filleted graft Tissue fashioned from a nearby part, usually a finger, from which the bone has been removed, with more neurovascular bundles Indication: at hand, only when deep tissues, such as tendons, nerves, and joints, are exposed, and when a nearby damaged finger is to be sacrificed because it is not salvageable Never used at the expense of a salvageable, useful part

23
Filleted graft Advantages It can be applied in a one-stage procedure Its survival is almost ensured because one or more of its neurovascular bundles are preserved Its skin is similar to that which is to be replaced It is not attached to a distant part, and consequently after surgery the hand may be splinted in the position of function and elevated It provides an adequate thumb web when the index finger is the donor Campbell 2007 11th ed Vol 4

24
946 moniter Currently techniques: Ultrasound and laser Doppler scanning Digital plethysmography Transcutaneous oxygen tension monitoring Continuous temperature monitoring: simplest method Fluorescein perfusion monitoring Radioisotope clearance assays Photoplethysmography Normal digital temperature: 30 ~ 35°C Replanted digits: temperatures within 2 ~ 3°C of control digit If < 30°C thrombosis on arterial or venous side, reexploration of replanted part or free flap

25
947 Great Toe Wraparound Flap 1980, Morrison et al: a free vascularized composite tissue transfer from the great toe to wrap around a traditional, nonvascularized autogenous iliac crest bone graft for thumb reconstruction A good reconstructive procedure for thumb amputated at or distal to metacarpophalangeal joint Advantages: Restoration of length, overall size, sensibility, movement, and thumb cosmesis Reliable neurovascular supply Only a single-stage procedure required Preservation of foot skeleton Minimal to no gait disturbance Minimal donor site morbidity Campbell 2007 11th ed Vol 4

26
Great Toe Wraparound Flap Disadvantages: Requirements for two-team approach Potential loss of entire flap because of thrombosis Potential for bone graft resorption Loss of interphalangeal motion Potential for significant donor site morbidity should the skin graft fail or if dissection is carried too far proximally Inability to use in young children because of the impossibility of estimating appropriate length. Campbell 2007 11th ed Vol 4

29
948 absolute contraindications for free flap Neither microsurgical training nor microsurgical experience Institutional support for a reconstructive microsurgical program is insufficient No suitable recipient vessels are available in the area requiring coverage or tissue reconstruction Previous trauma or irradiation to the recipient area If only one major artery to the foot or the hand is present, the use of it as the recipient vessel for a free flap may jeopardize the viability of the foot or hand Age, major systemic illnesses create a major anesthetic risk for the patient, an alternative method of treatment should be considered Obesity makes dissection of vascular pedicles difficult or impossible If systemic illnesses, such as atherosclerosis, vasculitis, or other lesions, have caused damage to the vascular system, microvascular procedures, although not certain to fail If previous operative procedures have been done in the donor area, the donor vessels may have been damaged Campbell 2007 11 th ed Vol 4

30
949 Healthy flap: pink, warm, minimally edematous, capillary refill time of 1-3 seconds. The prick test will produce 1-3 drops of bright red blood Venous anastomotic thrombosis: > 90% of flap failures Dark blue, congested appearance of cutaneous portion of transferred tissue Concurrent hematoma within operative site Christopher, UTMB, Dept. of Otolaryngology 2002

31
950 flap blood supply Pectoralis major muscle flap: pectoral branch of thoracoacromial artery Rectus abdominis muscle: deep superior and inferior epigastric arteries Latissimus dorsi flap: musculocutaneous perforators branch from thoracodorsal artery Groin flap: superficial circumflex iliac artery and vein Iliac crest bone flap: deep circumflex iliac artery and vein Christopher, UTMB, Dept. of Otolaryngology 2002

32
951 free vascularized bone graft Fibula Rib Ileum

33
952 Toe-to-hand transfer Transfer of the great toe to the hand: reconstruct the thumb after amputations from the level of the metacarpal base to the interphalangeal joint Indication: hands with multiple injuries and multiple amputations because it provides an opposable thumb for remaining digits To reconstruct thumb lost at or near metacarpophalangeal joint with no adjacent digits available for pollicization Great toe transfer was preferred over pollicization of an intact finger Gordon et al: posttraumatic thumb loss + entire loss of 1 st metacarpal is better treated by pollicization or second toe transfer, because of impairment in ambulation caused by loss of 1 st metatarsal

34
953 Tendon Transfers Median Nerve Palsy Classification 1) High Above Origin Of Anterior Interosseous Nerve Pronator Teres And Quadratus, FCR, FDS (II – V), FDP(II & III) And FPL Paralyzed 2) Low Thenar Intrinsic Muscles Paralyzed – Abductor Pollicis Brevis, Opponens Pollicis, And Superficial Head Of Flexor Pollicis Brevis
 High Above Origin Of Anterior Interosseous Nerve Pronator Teres And Quadratus, FCR, FDS (II – V), FDP(II & III) And FPL Paralyzed 2) Low Thenar Intrinsic Muscles Paralyzed – Abductor Pollicis Brevis, Opponens Pollicis, And Superficial Head Of Flexor Pollicis Brevis")
35
Tendon Transfers Low Median Nerve Palsy Standard Opponensplasties 1) FDS Opponensplasty Royle-Thompson Technique Bunnell Technique 2) Extensor Indicis Proprius Opponensplasty 3) Huber Transfer Abductor Digiti Minimi 4) Camitz Procedure Palmaris Longus
 FDS Opponensplasty Royle-Thompson Technique Bunnell Technique 2) Extensor Indicis Proprius Opponensplasty 3) Huber Transfer Abductor Digiti Minimi 4) Camitz Procedure Palmaris Longus")
36
Tendon Transfers Low Median Nerve Palsy Royle-Thompson – FDS Brought Around Ulnar Border Of Palmar Aponeurosis – FDS : Large Potential Excursion Adjusting Tension Not As Critical Margin For Error

37
Tendon Transfers Low Median Nerve Palsy Bunnel Technique – Ring Finger FDS Divided – FCU Exposed 4cm Proximal To Pisiform Insertion – Tendon Split Into Two Halves – Free End Looped Back Onto Its Base Ensure Loop Not Too Tight

39
Tendon Transfers Low Median Nerve Palsy 3. Huber Transfer – Difficult Procedure Neurovascular Pedicle Easily Damaged – Dorsoradial Aspect Insertions Divided – Base Of Prox. Phalynx And Ext. Apparatus Freed Off Pisiform – Attachments To FCU Retained Attached To Abductor Pollicis Brevis Insertion

41
Tendon Transfers Low Median Nerve Palsy 4) Camitz Procedure – Usually For Complication Of Severe Carpal Tunnel Syndrome Performed At Same Time As Carpal Tunnel Release Restores Palmar Abduction – Rather Than Opposition Not Recommended With Traumatic Median Nerve Injuries – Palmaris Longus Usually Scarred
 Camitz Procedure – Usually For Complication Of Severe Carpal Tunnel Syndrome Performed At Same Time As Carpal Tunnel Release Restores Palmar Abduction – Rather Than Opposition Not Recommended With Traumatic Median Nerve Injuries – Palmaris Longus Usually Scarred")
43
Tendon Transfers Low Median Nerve Palsy Other Options For Opponensplasty – Extensor Carpi Ulnaris – Extensor Carpi Radialis Longus – Extensor Digiti Minimi – Flexor Pollicis Longus – Extensor Pollicis Longus

44
954 chronic osteomyelitis Hyperbaric oxygen therapy: another method for Tx

45
955 CRPS Defined: a syndrome of diffuse limb pain and injury of noxious stimuli with variable sensory, motor, autonomic and trophic changes 2 components: SMP, SIP Sympathetically maintained pain: as “pain that is maintained by sympathetic efferent innervation or by circulating catecholamine” Sympathetically independent pain: describes that the subgroup of Pts who do not respond well to sympathetic blockade, suggests possibly neuropathic mechanism for pain

46
Tx of CRPS Therapeutic options include: multidisciplinary Drugs Interruption of the sympathetic supply Other interventional procedures Physical forms of treatment Psychological approaches

48
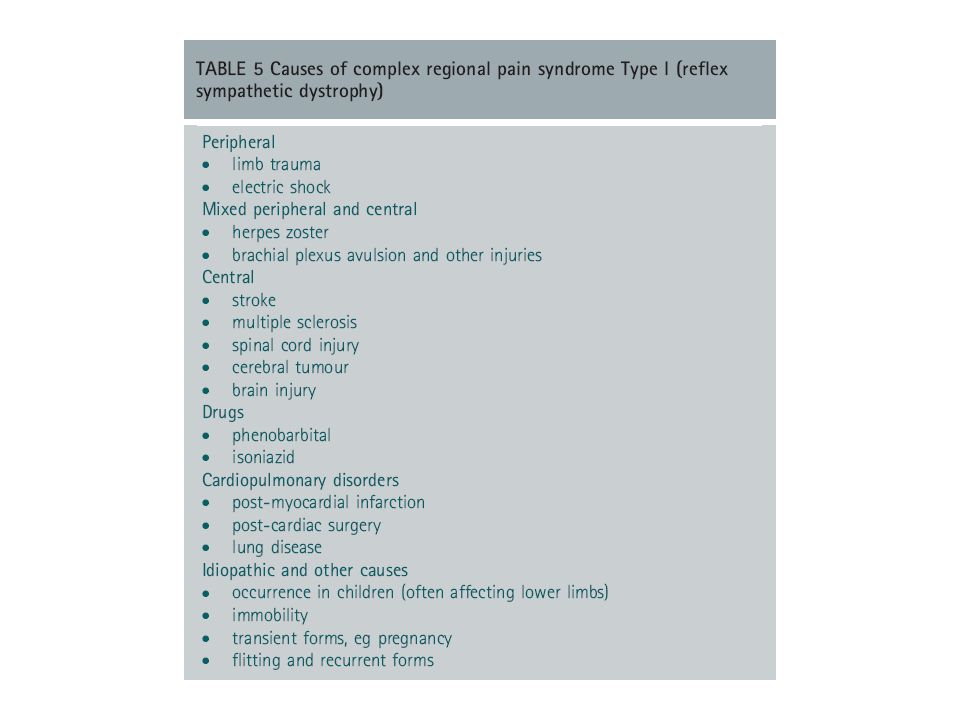
956 Type I: reflex sympathetic dystrophy Type II: causalgia Type III: other pain dysfunction problems Causalgia: usually a devastating injury has occurred, which by definition has caused a major nerve injury

49
957 Stage I: synovitis (+), joint surface maintain Stage II: mild to moderate synovitis + joint space narrowing, maintained joint contour Stage III: mild to moderate synovitis + mild to moderate alteration of joint surface, Stage IV: mechanical instability, complete joint space destructio OKU 8 324
, joint surface maintain Stage II: mild to moderate synovitis + joint space narrowing, maintained joint contour Stage III: mild to moderate synovitis + mild to moderate alteration of joint surface, Stage IV: mechanical instability, complete joint space destructio OKU 8 324")
50
958 RA of elbow Arthroscopic or open synovectomy relieve symptom Role of radial head excision + synovectomy controversial Goal of arthroscope excise syovitis, not to cut through anterior capsule OKU 8 p324

Similar presentations