Download presentation
Presentation is loading. Please wait.

1
LASIK Complication A. Al-Muammar

2
LASIK Complication Intraoperative Poor exposure ► Deep orbit, small eye, narrow palpebral fissure, drape, and lid speculum Difficulty in placing suction ring Lid injury Poor centration during laser ablation Water pooling ► Lateral canthotomy, facial nerve block, retrobulbar block, converting to PRK, or abandoning surgery

3
LASIK Complication Intraoperative Inadequate suction ► Good suction ( IOP > 75 mmHg) would provide depth control during microkeratome pass ► Poor or broken suction can result in thin, buttonholes, or free cap ► Inadequate suction can be due to suction ports clogging by debris, drape, speculum, chemotic or redundant conjunctiva, or defect in suction line
 would provide depth control during microkeratome pass ► Poor or broken suction can result in thin, buttonholes, or free cap ► Inadequate suction can be due to suction ports clogging by debris, drape, speculum, chemotic or redundant conjunctiva, or defect in suction line")
4
LASIK Complication Intraoperative Flap complication ► Thin flap The incidence of thin flap reported to vary between 0.3% and 0.75% Flap considered to be thin when keratome cuts within or above Bowman’s layer Recognized by shinny reflex on the stromal surface It tends to occur with flat cornea or poor suction Reposition the flap and abort the procedure Deeper flap (20-60 micrm) maybe recut 10-12 weeks
 maybe recut weeks")
5
LASIK Complication Intraoperative ► Buttonholes flap A buttonholed flap occurs when microkeratome blade travels more superficially than intended and enters the epithelium/Bowman’s complex Buttonholes maybe partial thickness if they transect Bowman’s layer or full thickness if they exit through the epithelium. The incidence of buttonholes ranges between 0.2% and 0.56% Buttonholes flap tend to occurs in case of steep cornea >48 D, resistance to cutting, or lack of synchronization between keratome movement and oscillatory blade movement

6
LASIK Complication Intraoperative ► Tx Reposition the flap And wait 3 to 6 months before recutting Transepithelial PRK within 2 weeks

7
LASIK Complication Intraoperative Irregular flap ► Abnormal shape/diameter/ or thickness flap ► Result from damaged microkeratome blades, irregular oscillation speed, or poor suction ► Incidence 0.09%-0.2% ► Reposition the flap and abort the procedure

9
LASIK Complication Intraoperative ► Incomplete flap Created when the microkeratome blade comes to halt prior to reaching the intended location of the hinge Incidence ranges between 0.3% and 1.2% Microkeratome jamming due to either electrical failure or mechanical obstacles as lashes, drape, or loose epithelium Unless enough space exists for ablation( 1mm space between ablation and the edge), incomplete flap are best managed by immediate repositioning and postponing the procedure
, incomplete flap are best managed by immediate repositioning and postponing the procedure")
11
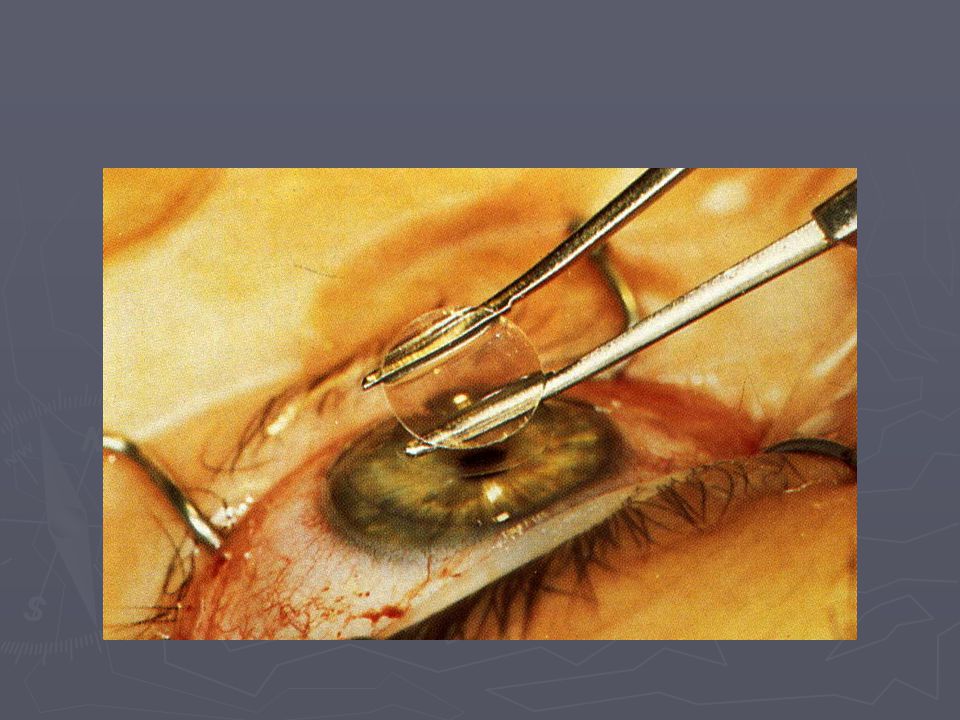
LASIK Complication Intraoperative ► Free flap Unintended free flap can occur with corneas flatter than 38D prior to surgery, poor suction, or migration of suction ring. Recent studies report an incidence between 0.01% and 1% If the flap is not visible on the surface of the cornea, then the flap could be inside the microkeratome head Marking the cornea prior to surgery is very important for proper placement of free flap If the cap has normal thickness and diameter, the ablation can still be performed. Flap repositioned using placed marks. A BCL applied to tamponade the cap. Suturing rarely necessary Abnormal thin/irregular flap which is the usual case should be repositioned using sutures, and laser should be delayed Early removal of sutures is important to minimize scarring If the flap cant be retrieved, epithelium is allowed to heal as in PRK

12
LASIK Complication Intraoperative ► Decentered flap Flap decenterations are attributable to an inexperienced surgeon improperly aligning the suction ring with the limbus or migration of the ring on the corneal surface when suction applied Most surgeon will not proceed with laser unless the ablation can be placed 1 mm of the bed is left between the ablation peripheral bed and the flap margin The Introduction of microkeratome with large diameter flap have reduced this problem

13
LASIK Complication Intraoperative ► Corneal perforation and anterior segment damage Result from error in placing the plate that control the depth of the cut into instruments Newer designs have eliminated the potential for these severe complications since they have a fixed depth plate and components of the microkeratome cannot be inserted incorrectly.

14
LASIK Complication Intraoperative ► Intraoperative bleeding Corneal neovascularization from pannus, decentered flap, and large flap are the most common causes of intraoperative bleeding Topical vasoconstrictors can be applied 3 to 5 minutes prior to surgery in high risk group Tamponade any bleeding prior to flap lifting Any blood that might interfere with laser should be irrigated

15
LASIK Complication postoperative ► Epithelial complication Incidence reported to be around 5% Epithelial defects more common in patients with abnormal epithelial adhesion as in EBMD, or patient with who develop epithelial defect in the first eye Mild staining at the edge of the flap is common Large defects are worrisome especially those with connection to the flap edge Epithelial defect can increase the risk of infection, epithelial ingrowth, and DLK Treated with BCL, or patch

16
LASIK Complication postoperative ► Pain Most patients experience only mild discomfort following LASIK Severe pain may herald more severe complication such as a displaced flap, DLK, or infection

17
LASIK Complication postoperative ► Flap striae and wrinkles Reported incidence between 0.2% and 1.5% It is related to the disparity between the curvature of the posterior surface of the flap and the bed following complication Large thin flap, improper BCL placement, removal of lid speculum, and eye rubbing can increase the risk of striae Striae can be micro or macro. Retroillumination and fluorescein can help in detecting striae Visually significant striae should be treated as soon as possible to avoid fixed striae LASIK flap iron, lifting the flap =/- suture, and PTK are possible options to treat striae

21
LASIK Complication postoperative ► Displaced flap Emergency, should be repositioned as soon as possible to prevent infection, fixed folds, and epithelial ingrowth Incidence have been reported to be 1.1% and 2% (old reports) Usually occur in the first 24 hrs after surgery Eye lid rubbing, squeezing, and trauma especially with large thin flap are the main predisposing factor for displaced flap Flap should be reflected, examined for epithelial cells or debris which should be scraped, the reposition the flap and apply BCL
 Usually occur in the first 24 hrs after surgery Eye lid rubbing, squeezing, and trauma especially with large thin flap are the main predisposing factor for displaced flap Flap should be reflected, examined for epithelial cells or debris which should be scraped, the reposition the flap and apply BCL")
23
LASIK Complication postoperative ► Epithelial ingrowth Reported incidence vary between 1% and 2% Possible mechanisms ► Mechanical dragging by keratome blade during keratectomy ► Backflow during irrigation carrying floating epithelial cells ► Ingrowth at the junction of the epithelium and keratotomy ► Implantation with instruments ► Cell migration through epithelial defect

24
LASIK Complication postoperative Complications ► Decrease visual acuity ► Anterior stromal melt Treatment ► Flap lifting ► Irrigation ► Scraping ► Alcohol ► PTK ► MMC ► suture

26
LASIK Complication postoperative ► lamellar interface debris ► Oil ► Mucous ► Particles from the sponge ► Metallic fragments from the Blade ► RBC ► Powder from gloves ► Lint fibres ► Lashes Peripheral debris which not associated with keratitis or neovascularization can be left undisturbed Central debris should be removed

28
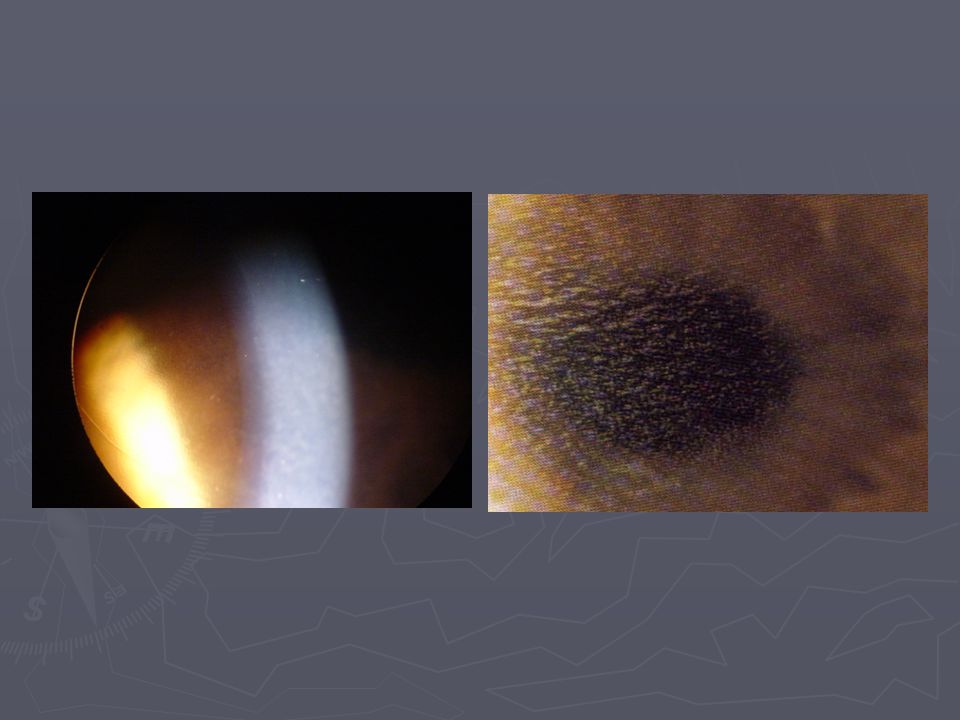
LASIK Complication postoperative ► Diffuse Lamellar Keratitis (DLK) Diffuse non-infectious inflammation at the level of the interface during the first few days after LASIK Reported incidence is highly variable, between 0.2% and 3.2% Possible causes, most of these are based on speculation without supporting data ► Betadine ► Impure BSS ► Retained meibomian secretions ► Metallic debris ► Talc from gloves ► Thermal effect from the laser ► Lubricants on the microkeratome or blades ► Topical medications such as anesthetics ► Bacterial cell wall components (lipopolysaccharides) ► Endotoxins ► IL 1 released from corneal epithelial cells following cell injury or death
 Diffuse non-infectious inflammation at the level of the interface during the first few days after LASIK Reported incidence is highly variable, between 0.2% and 3.2% Possible causes, most of these are based on speculation without supporting data ► Betadine ► Impure BSS ► Retained meibomian secretions ► Metallic debris ► Talc from gloves ► Thermal effect from the laser ► Lubricants on the microkeratome or blades ► Topical medications such as anesthetics ► Bacterial cell wall components (lipopolysaccharides) ► Endotoxins ► IL 1 released from corneal epithelial cells following cell injury or death")
29
LASIK Complication postoperative Stages ► Stage I seen on day 1 as white, granular cells in the periphery with sparing of the visual axis. ► Stage II seen on day 2 or 3, shows white cells in the visual axis ► Stage III involves an aggregation of cells clumped in the visual axis and associated with haze and reduce vision ► Stage IV involves central stromal necrosis, melt, and secondary hyperopia with irregular astigmatism

31
LASIK Complication postoperative ► Tx Stage I and II, should be treated with intense topical steroid every 1 hr If inflammation progressed even with steroid or patient presented with stage III or IV ► the flap should be lifted ► Cleaning ► profuse irrigation ► Culture for bacteria and fungus ► Topical steroid =/- oral steroid ► PTK/HCL

32
LASIK Complication postoperative ► Infection Infectious agents that have been reported after LASIK include ► Virus ► Bacteria (including atypical mycobacterium and nocardia) ► Fungus ► Parasite If infiltrate noted, it should be treated as infectious until proven otherwise Infiltrate should be cultured …bacteria, fungus, acanthameoba, Ziehle-Nelson stain Tx ► Abx ► Antifungal ► Antiviral ► Flap removal
 ► Fungus ► Parasite If infiltrate noted, it should be treated as infectious until proven otherwise Infiltrate should be cultured …bacteria, fungus, acanthameoba, Ziehle-Nelson stain Tx ► Abx ► Antifungal ► Antiviral ► Flap removal")
33
LASIK Complication postoperative ► Dry eye Neurotrophic in origin Worse in patient who are known to have dry eye Present with PEE and visual fluctuation May last 6 to 8 months Tx ► Tears ► Punctum plug

34
LASIK Complication postoperative ► Corneal ectasia Iatrogenic keratoconus like condition Minimum stromal bed thickness of 250-300 microm should be left after laser ablation Present as progressive myopia, or decrease visual acuity secondary to irregular astigmatism Dx ► Orbscan ► Pachymetry Tx ► RCL ► Corneal ring ► PKP

36
LASIK Complication psotoperative Decentration Irregular astigmatism Glare, and haloes Overcorrection Undercorrection

Similar presentations














>")







thus effecting baseline evaluation.>")




