Download presentation
Presentation is loading. Please wait.

1
Improving outcomes in Atrial Fibrillation GLOS CCG AGM Jim Moore 18 th September 14

3
+ =

5
Projected Number of Patients With AF by 2050 Olmsted County data, 2006 (assuming a continued increase in the AF incidence) ATRIA study data, 2000 Olmsted County data, 2006 (assuming no further increase in the AF incidence) MarketScan & Thomson Reuters Medicare databases, 2009 3.03 7.56
 ATRIA study data, 2000 Olmsted County data, 2006 (assuming no further increase in the AF incidence) MarketScan & Thomson Reuters Medicare databases,")
6
Prevalence AF by practice

7
Prevalence AF a linear Relationship to over 65yrs

9
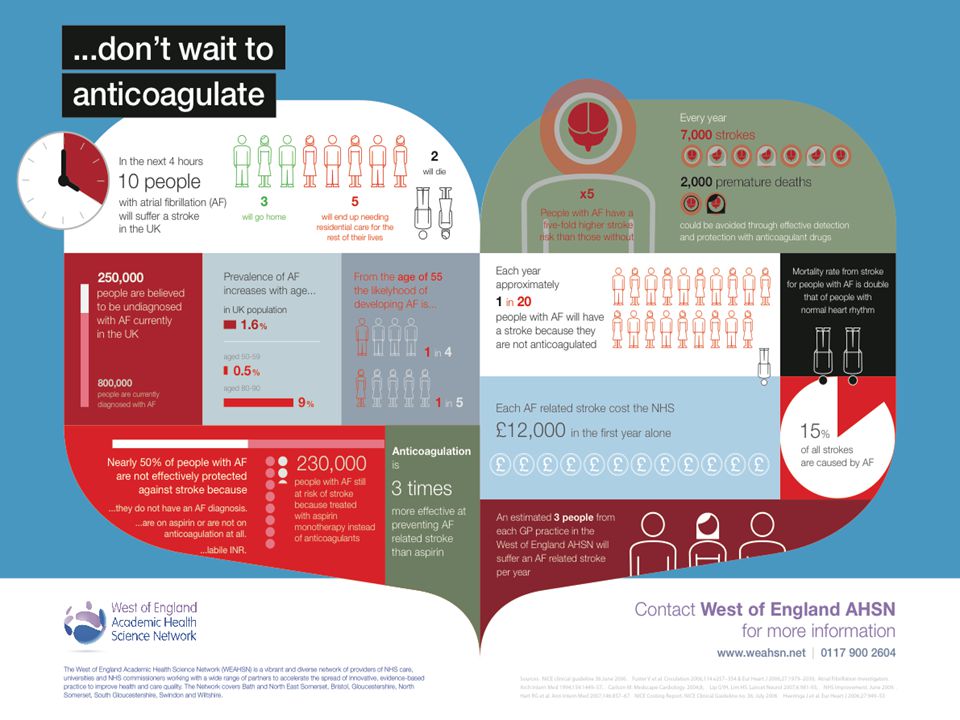
Stroke is a serious complication of AF AF stroke is usually more severe than stroke due to other causes 1 Compared with other stroke patients, those with AF are more likely to: – Have cortical deficit (e.g. aphasia), severe limb weakness and diminished alertness, and be bedridden on admission 2 – Have longer in-hospital stay with a lower rate of discharge to their own home 3 The mortality rate for patients with AF is double that in people with normal heart rhythm 4 9 1. Savelieva I et al. Ann Med 2007;39:371–91; 2. Dulli DA et al. Neuroepidemiology 2003;22:118–23; 3. NICE clinical guideline 36.June 2006. Available at http://www.nice.org.uk/guidance/CG36/?c=91497; accessed April 2010;http://www.nice.org.uk/guidance/CG36/?c=91497 4. Benjamin EJ et al. Circulation 1998;98:946–52
, severe limb weakness and diminished alertness, and be bedridden on admission 2 – Have longer in-hospital stay with a lower rate of discharge to their own home 3 The mortality rate for patients with AF is double that in people with normal heart rhythm Savelieva I et al. Ann Med 2007;39:371–91; 2. Dulli DA et al. Neuroepidemiology 2003;22:118–23; 3. NICE clinical guideline 36.June Available at c=91497; accessed April 2010; c= Benjamin EJ et al. Circulation 1998;98:946–52.")
10
Plan Personalised package of care Identifying patients with AF Assessing and managing stroke risk

11
NICE AF Key priorities for implementation Personalised package of care and information Assessment of stroke and bleeding risks Interventions to prevent stroke

12
Plan Personalised package of care Identifying patients with AF Assessing and managing stroke risk

13
Personalised package of care and information Offer people with atrial fibrillation a personalised package of care. Ensure that the package of care is documented and delivered, and that it covers: o stroke awareness and measures to prevent stroke o rate control o assessment of symptoms for rhythm control o who to contact for advice if needed o psychological support if needed o up ‑ to ‑ date and comprehensive education and information on: ……………..

14
Personalised package of care and information (cont) o Offer people with atrial fibrillation a personalised package of care. Ensure that the package of care is documented and delivered, and that it covers: o up ‑ to ‑ date and comprehensive education and information on: cause, effects and possible complications of atrial fibrillation management of rate and rhythm control anticoagulation practical advice on anticoagulation support networks ( e.g. cardiovascular charities)[new2014]
[new2014].")
15
Who are West of England AHSN? The West of England Academic Health Science Network is a vibrant and diverse network of providers of NHS care, universities and NHS commissioners working with a wide range of parties to accelerate the spread of innovating evidence- based practice to improve health and care quality www.weahsn.net 2.4M people Bath,Bristol, Swindon South Gloucestershire, North and North East Somerset, Gloucestershire, Wiltshire (West & North)
.")
16
PLAN Personalised package of care Identifying patients with AF Assessing and managing stroke risk

17
Identifying patients with AF Targeted/Opportunistic -hypertension, -CVD assessment, -Diabetes -Symptoms commonly seen in AF - when taking blood pressure Whole population screening Routine clinical practice

18
SAFE study Hobbs et al 2005 A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. To determine the most cost-effective method of screening for atrial fibrillation (AF) in the population aged 65 years and over, as well as its prevalence and incidence in this age group. Fifty primary care centres across the West Midlands, UK. Multi-centred randomised controlled trial. Purposefully selected general practices were randomly allocated to 25 intervention practices and 25 control practices 10,00 patients in intervention practices - 5,000 systematic screening and 5,000 opportunistic screening GPs and nurses in intervention practices educated around the identification of AF and the interpretation of ECGS.
 in the population aged 65 years and over, as well as its prevalence and incidence in this age group. Fifty primary care centres across the West Midlands, UK. Multi-centred randomised controlled trial. Purposefully selected general practices were randomly allocated to 25 intervention practices and 25 control practices 10,00 patients in intervention practices - 5,000 systematic screening and 5,000 opportunistic screening GPs and nurses in intervention practices educated around the identification of AF and the interpretation of ECGS..")
19
SAFE study results Hobbs et al 2005 Baseline prevalence of AF 7.2% Incidence of AF/year - Opportunistic screening 1.64% -Systematic screening 1.62% -Control 1.04% As far as screening programmes for atrial fibrillation in patients 65 and over, the only strategy that improved on routine practice was opportunistic screening 60% probability that annual opportunistic screening was cost effective The lowest incremental cost was for the opportunistic arm, with an incremental cost-effectiveness ratio of £337 for each additional case of AF detected compared to the control arm. ECG interpretation - computerised decision support software (CDSS) gave a sensitivity of 87.3%, a specificity of 99.1% and a positive predictive value (PPV) of 89.5%
 gave a sensitivity of 87.3%, a specificity of 99.1% and a positive predictive value (PPV) of 89.5%.")
20
Identification of patients with AF at Stoke Road Surgery Patients presenting with clinical features of AF Secondary/Tertiary care diagnosis of AF Hypertension monitoring (irregular pulse) ECG undertaken for other reasons
 ECG undertaken for other reasons")
21
Hypertension monitoring HCA/PN assessment of radial/ brachial pulse prior to taking BP(on every occasion) in all patients as per Hypertension Protocol Patients with irregular pulse have 12 lead ECG undertaken at the same appointment and are then reviewed by Duty GP No BP monitors will accurately measure BP in AF
 in all patients as per Hypertension Protocol Patients with irregular pulse have 12 lead ECG undertaken at the same appointment and are then reviewed by Duty GP No BP monitors will accurately measure BP in AF")
22
QOF AF Statistics (March 14) Stoke Road Practice AF prevalence - 2.6% (see footnote) National AF prevalence range from 1.3 - 1.7% Note present SR practice AF prevalence at June 14 = 3.0 %
 Stoke Road Practice AF prevalence - 2.6% (see footnote) National AF prevalence range from % Note present SR practice AF prevalence at June 14 = 3.0 %")
23
AGENDA Personalised package of care Identifying patients with AF Assessing and managing stroke risk

24
Thromboembolic risk assessment is a priority! ………..local guidance

25
………..international guidance!

28
When assessing stroke risk ask the question …………why should I not anticoagulate this patient ?

29
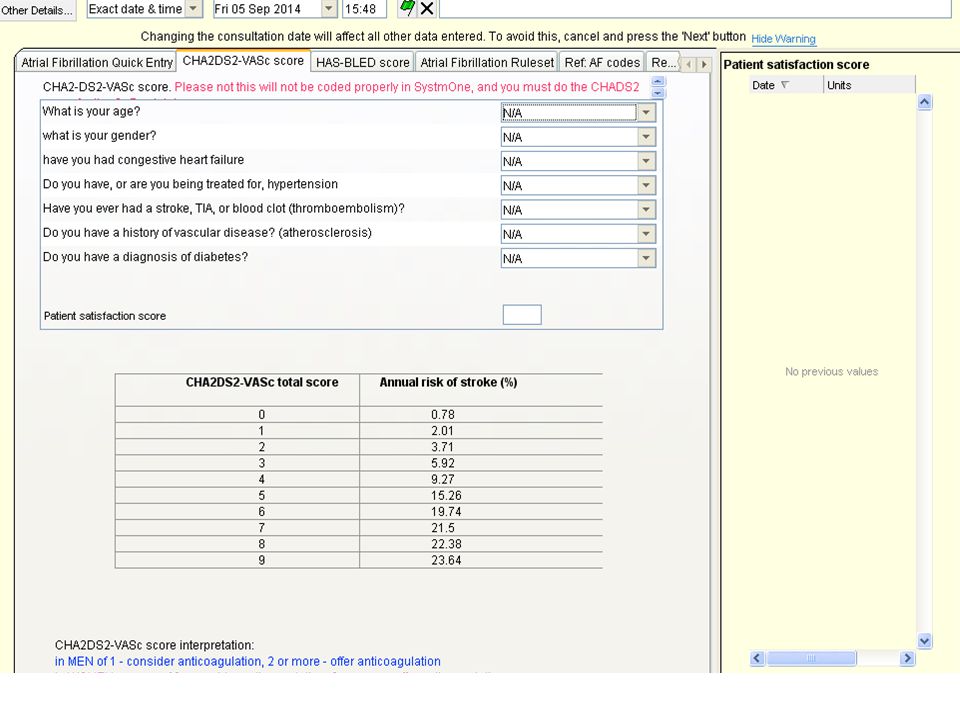
Stroke risk assessment with CHADS 2 and CHA 2 DS 2 -VASc

30
CHADS score % AF popltn 0 low risk 16.3 1 moderate risk 26.7 2(+) high risk 57 Cowan C et al. Heart doi:10.1136/heartjnl-2012-303472

31
Oral anti-coagulation: benefit–risk improves with increasing age Singer DE et al. Ann Intern Med 2009;151:297–305 Net clinical benefit: events prevented per 100 person-years 1 1.00 Better with warfarinWorse with warfarin Age, years 2.34 3.301.29 ≥85 1.400.44 75–84 0.11 0.40–0.37 65–74 –0.25 0.08–0.65 <65 –1–0.50.511.522.533.5 0

32
Coagulation pathway VKA Inactive Factor Active Factor Transformation Catalysis X IX IXa Thrombin Xa Fibrinogen Fibrin Prothrombi n VII TF VIIa Initiation Propagatio n VKA Direct Factor Xa inhibition Rivaroxaban Direct Factor IIa inhibition Dabigatran II IIa Spyropoulos AC et al. Expert Opin Investig Drugs 2007;16:431–440 (adapted from)
.")
33
NICE CG180 -Management of AF Assessment of stroke and bleeding risks CHA2DS2-VASc stroke risk score should be used to assess stroke risk in people with any of the following: symptomatic or asymptomatic paroxysmal, persistent or permanent atrial fibrillation atrial flutter a continuing risk of arrhythmia recurrence after cardioversion back to sinus rhythm. [new 2014]

34
NICE CG180 -Management of AF Interventions to prevent stroke Do not offer stroke prevention therapy to people aged under 65 years with atrial fibrillation and no risk factors other than their sex (that is, very low risk of stroke equating to a CHA2DS2-VASc score of 0 for men or 1 for women). [new 2014]CHA2DS2-VASc score of 0 for men or 1 for women). [new 2014] Anticoagulation may be with apixaban, dabigatran etexilate, rivaroxaban or a vitamin K antagonist. Consider anticoagulation for men with a CHA2DS2-VASc score of 1. Take the bleeding risk into account. [new 2014]CHA2DS2-VASc score of 1. Take the bleeding risk into account. [new 2014] Offer anticoagulation to people with a CHA2DS2-VASc score of 2 or above, taking bleeding risk into account. [new 2014]CHA2DS2-VASc score of 2 or above, taking bleeding risk into account. [new 2014] Discuss the options for anticoagulation with the person and base the choice on their clinical features and preferences. [new 2014]
. [new 2014] Anticoagulation may be with apixaban, dabigatran etexilate, rivaroxaban or a vitamin K antagonist. Consider anticoagulation for men with a CHA2DS2-VASc score of 1. Take the bleeding risk into account. [new 2014]CHA2DS2-VASc score of 1. Take the bleeding risk into account. [new 2014] Offer anticoagulation to people with a CHA2DS2-VASc score of 2 or above, taking bleeding risk into account. [new 2014]CHA2DS2-VASc score of 2 or above, taking bleeding risk into account. [new 2014] Discuss the options for anticoagulation with the person and base the choice on their clinical features and preferences. [new 2014].")
35
… and what harm !

36
NICE CG180 -Management of AF Bleeding risk Use the HAS-BLED score to assess the risk of bleeding in people who are starting or have started anticoagulation. Offer modification and monitoring of the following risk factors uncontrolled hypertension poor control of international normalised ratio (INR) ('labile INRs') concurrent medication, for example concomitant use of aspirin or a non ‑ steroidal anti ‑ inflammatory drug (NSAID) harmful alcohol consumption. [new 2014]
 ( labile INRs ) concurrent medication, for example concomitant use of aspirin or a non ‑ steroidal anti ‑ inflammatory drug (NSAID) harmful alcohol consumption. [new 2014].")
37
HAS-BLED should be used to identify modifiable risk factors for bleeding Score of ≥3 indicates need for regular clinical review Patients with a higher HAS-BLED score also have a higher CHA2DS2-VASc score There is net clinical benefit in anticoagulating CHA2DS2-VASc >0 whatever HAS-BLED score

38
NICE CG180 -Management of AF Bleeding risk When discussing the benefits and risks of anticoagulation, explain to the person that: for most people the benefit of anticoagulation outweighs the bleeding risk for people with an increased risk of bleeding the benefit of anticoagulation may not always outweigh the bleeding risk, and careful monitoring of bleeding risk is important. [new 2014] Do not withhold anticoagulation solely because the person is at risk of having a fall. [new 2014]

39
Monitoring anticoagulation control with Warfarin

40
Drug and food interactions with warfarin

41
VKAs have a narrow therapeutic window 5.06.08.01.02.03.04.07.0 5 15 10 Ischaemic stroke Intracranial bleeding 1 20 Odds ratio for event International normalized ratio Adjusted odds ratios for ischaemic stroke and intracranial bleeding in relation to intensity of anticoagulation Target INR Adapted from Wann et al. Circulation 2011;123;e269-e367

42
Why time in therapeutic range(TTR) matters
 matters")
43
NICE CG180 -Management of AF Assessing anticoagulation control with vitamin K antagonists Calculate the person's time in therapeutic range (TTR) at each visit. When calculating TTR: use a validated method of measurement such as the Rosendaal method for computer ‑ assisted dosing or proportion of tests in range for manual dosing exclude measurements taken during the first 6 weeks of treatment calculate TTR over a maintenance period of at least 6 months. [new 2014]

44
NICE CG180 -Management of AF Assessing anticoagulation control with vitamin K antagonists Reassess anticoagulation for a person with poor anticoagulation control shown by any of the following: 2 INR values higher than 5 or 1 INR value higher than 8 within the past 6 months 2 INR values less than 1.5 within the past 6 months TTR less than 65%. [new 2014]

45
NICE CG180 -Management of AF Assessing anticoagulation control with vitamin K antagonists When reassessing anticoagulation, take into account and if possible address the following factors that may contribute to poor anticoagulation control: cognitive function adherence to prescribed therapy Illness interacting drug therapy lifestyle factors including diet and alcohol consumption. [new 2014] If poor anticoagulation control cannot be improved, evaluate the risks and benefits of alternative stroke prevention strategies and discuss these with the person. [new 2014]

46
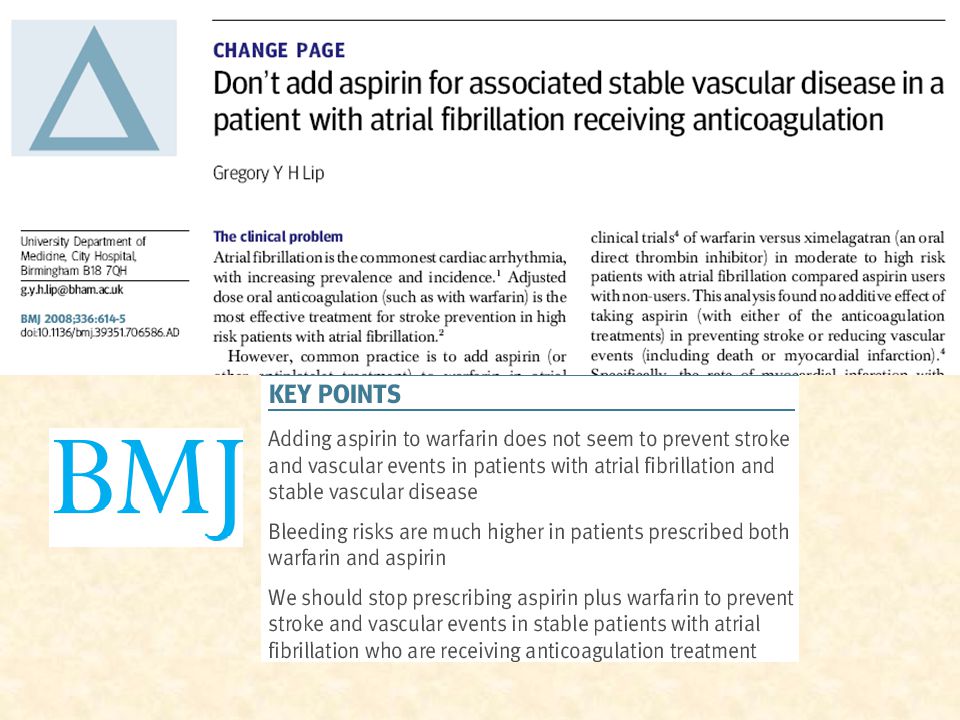
NICE CG180 -Management of AF Antiplatelets Do not offer aspirin monotherapy solely for stroke prevention to people with atrial fibrillation. [new 2014]

48
Management of the patient with AF 1)Thromboprophylaxis 2)Symptom control 3)LV protection Decreasing importance
Thromboprophylaxis 2)Symptom control 3)LV protection Decreasing importance")
49
What informs current practice ?

51
QOF 2014-15

52
Warfarin reduces the risk of stroke in patients with AF Error bars = 95% CI; *Relative risk reduction for all strokes (ischaemic and haemorrhagic) Warfarin betterPlacebo better Relative risk reduction (%)* 100–100500–50 AFASAK SPAF BAATAF CAFA SPINAF EAFT All trials RRR = 64% 95% CI: 49 to 74% Hart RG et al. Ann Intern Med 2007;146:857–67

53
Limited efficacy of aspirin in reducing the risk of stroke in patients with AF Aspirin betterPlacebo better Relative risk reduction (%)* 100–100500 –50 RRR = 19% 95% CI: –1 to 35% All trials JAST UK-TIA 300 mg/d 1200 mg/d LASAF 125 mg/d 125 mg QOD ESPS II EAFT SPAF AFASAK Error bars = 95% CI; *Relative risk reduction for all strokes (ischaemic and haemorrhagic) Hart RG et al. Ann Intern Med 2007;146:857–67

54
Stroke risk and aspirin use 52% of patients diagnosed with AF are treated with antiplatelet treatment such as aspirin Prescription of aspirin increases steeply with increasing CHADS 2 score Lee S et al. BMJ Open 2011;1:e000269. Percentage of patients CHADS 2 score 0.9 0 0 125 0.7 0.5 0.3 0.1 34 0.8 0.6 0.4 0.2 Anticoagulants – Male Anticoagulants – Female Anti platelets – Male Anti platelets – Female p<0.001 p=0.12 p=0.57

55
Copyright © BMJ Publishing Group Ltd & British Cardiovascular Society. All rights reserved. Cowan C et al. Heart doi:10.1136/heartjnl-2012-303472 Proportion (95% CI) of atrial fibrillation patients prescribed anticoagulant therapy (A) and antiplatelet therapy (B) by CHADS 2 score for patients aged 80 years and over, and for patients aged under 80 years
 of atrial fibrillation patients prescribed anticoagulant therapy (A) and antiplatelet therapy (B) by CHADS 2 score for patients aged 80 years and over, and for patients aged under 80 years.")
56
Not all clots are the same Thrombi in patients with AF are predominately fibrin-rich Thrombi in coronary artery disease (CAD) tend to be platelet-rich Anticoagulants reduce the conversion of fibrinogen to fibrin Aspirin, and other antiplatelets, inhibit aggregation of thrombi caused by CAD but do not impact upon fibrin production ridge.icu.ac.jp Lip GYH. Nature Reviews Cardiology 2011:8;602–606

57
What the guidelines say about aspirin in AF-related stroke Royal College of Physicians, Edinburgh UK Consensus: March 2012 Aspirin should not be used for stroke prevention in AF European Society of Cardiology: Management of AF 2012 Aspirin should not be used for stroke prevention in AF

58
Aspirin in Stroke Prevention 18.6.14 Key message:

60
Oral anticoagulation for stroke prevention in AF Antiplatelet therapy with aspirin plus clopidogrel or – less effectively – aspirin only, should be considered in patients who refuse any OAC or cannot tolerate anticoagulation for reasons unrelated to bleeding. If there are contraindications to OAC or antiplatelet therapy, left atrial appendage occlusion, closure or excision may be considered Colour CHA 2 DS 2 -VASc: green = 0, blue = 1, pink ≥2; line: solid = best option; dashed = alternative option *Includes rheumatic valvular disease and prosthetic valves; NOAC = novel oral anticoagulant; VKA = vitamin K antagonist Camm AJ, et al. Eur Heart J doi:10.1093/eurheartj/ehs253 Yes Atrial fibrillation Valvular AF* <65 years and lone AF (including females) Assess risk of stroke CHA 2 DS 2 -VASc score Assess bleeding risk (HAS-BLED score) Consider patient values and preferences No antithrombotic therapy Oral anticoagulant therapy NOAC VKA No (i.e. nonvalvular) Yes No 0 0 1 1 ≥2
 Assess risk of stroke CHA 2 DS 2 -VASc score Assess bleeding risk (HAS-BLED score) Consider patient values and preferences No antithrombotic therapy Oral anticoagulant therapy NOAC VKA No (i.e. nonvalvular) Yes No ≥2.")
61
Diagnosis of AF and management of associated thromboembolic risk in Primary care Stoke Road Surgery Bishops Cleeve Dr Jim Moore GP

62
Assessment of patients with confirmed AF by GP Admit if evidence of decompensation Follow AGWS AF guidelines Assess and discuss thromboembolic risk (CHADS2VASC2) at first assessment. Provide written information on stroke risk /bleeding risk Arrange follow up in practice CVD clinic (provides urgent appointments for newly diagnosed AF )
.")
63
……………use template!

67
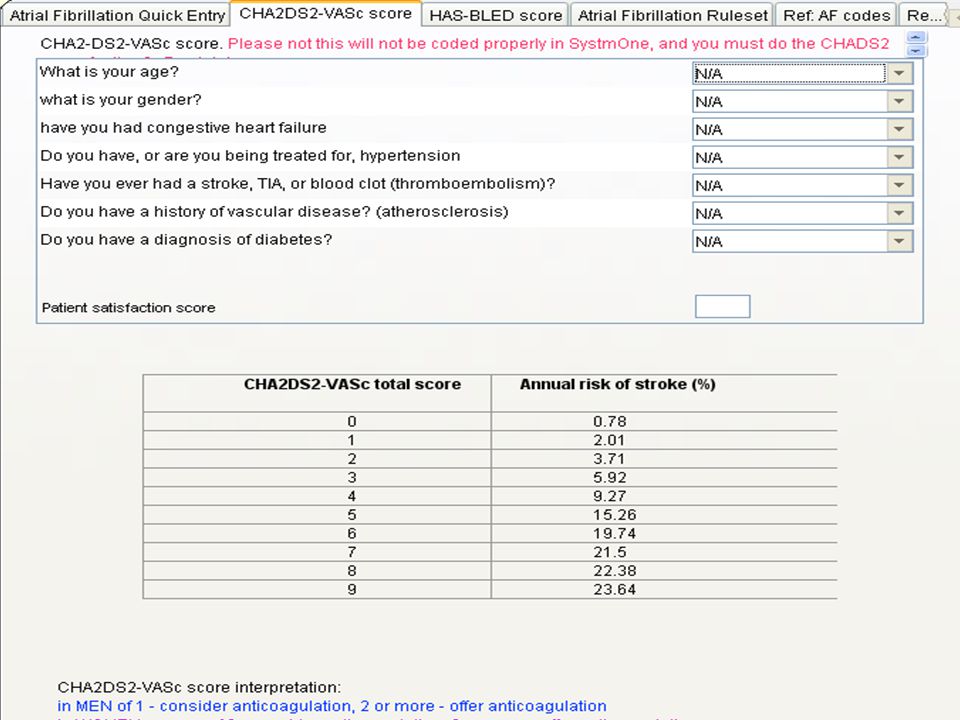
Atrial Fibrillation Quick entry Patient thought to be in AF: non acute onset and no evidence of cardiac decompensation. Confirm on ECG (same day) If ECG confirms AF, then Duty Dr to review patient Assess thromboembolic risk using CHADS2 and CHA2DS2-VASc (CHADS2 is for QOF purposes only) Using bleeding risk using HAS-BLED Discuss Stroke vs bleeding risk with patient If anticoagulation is indicated then initiate same day with: Rivaroxaban 20mg daily (if eGFR greater than 30) or Fragmin 5000 units (s/c) while starting warfarin (stop once INR 2-3) Consider rate control with bisoprolol (or verapamil if contraindication to betablockers) Give patient information leaflets about AF and long term anticoagulation options Arrange follow up appointment in one week. DO NOT OFFER ASPIRIN FOR STROKE PREVENTION IN AF
 If ECG confirms AF, then Duty Dr to review patient Assess thromboembolic risk using CHADS2 and CHA2DS2-VASc (CHADS2 is for QOF purposes only) Using bleeding risk using HAS-BLED Discuss Stroke vs bleeding risk with patient If anticoagulation is indicated then initiate same day with: Rivaroxaban 20mg daily (if eGFR greater than 30) or Fragmin 5000 units (s/c) while starting warfarin (stop once INR 2-3) Consider rate control with bisoprolol (or verapamil if contraindication to betablockers) Give patient information leaflets about AF and long term anticoagulation options Arrange follow up appointment in one week. DO NOT OFFER ASPIRIN FOR STROKE PREVENTION IN AF.")
Similar presentations



























>")
