Download presentation
Presentation is loading. Please wait.

1
AF and the New Oral Anti-Coagulants
Evidenced based approach. Adapted from ESC guidelines. Dr Raj Chahal, Cardiology Trainee November 2013

2
Current State Of Play Atrial Fibrillation (AF) is not a benign condition. Increased risk of stroke. Risk of stroke varies with risk factors. Increase mortality hazard ratio aside from stroke risk.

3
Clinical Events (outcomes) affected by AF
3

4
Prevalence The most common sustained cardiac arrhythmia
Hospital based prevalence data probably underestimates as often asymptomatic. Prevalence doubles with each decade of age from 0.5% at age to 9% at years. Risks factors of developing AF: Age (OR 2.1 Men, 2.2 Women) Diabetes (OR 1.4 Men, 1.6 Women) Hypertension (OR 1.5 Men, 1.4 Women) Valve disease (OR 1.8 Men, 3.4 Women)
 Diabetes (OR 1.4 Men, 1.6 Women) Hypertension (OR 1.5 Men, 1.4 Women) Valve disease (OR 1.8 Men, 3.4 Women)")
5
Conditions predisposing to, or encouraging progression of AF
5

6
Stroke Risk CHADS2 Cardiac Failure Hypertention Age over 75 Diabetes
Stroke/TIA (2 points)
")
7
CHADS2 score and stroke rate
*The adjusted stroke rate was derived from the multivariable analysis assuming no aspirin usage; these stroke rates are based on data from a cohort of hospitalised AF patients, published in 2001, with low numbers in those with a CHADS2 score of 5 and 6 to allow an accurate judgement of the risk in these patients. Given that stroke rates are declining overall, actual stroke rates in contemporary non-hospitalised cohorts may also vary from these estimates. Adapted from Gage BF et al. AF = atrial fibrillation; CHADS2 = cardiac failure, hypertension, age, diabetes, stroke (doubled). 7
. 7.")
8
Risk factors for stroke and thrombo-embolism in non-valvular AF
AF= atrial fibrillation; EF = ejection fraction (as documented by echocardiography, radionuclide ventriculography, cardiac catheterization, cardiac magnetic resonance imaging, etc.); LV = left ventricular; TIA = transient ischaemic attack. 8
; LV = left ventricular; TIA = transient ischaemic attack. 8.")
9
Adjusted stroke rate according to CHA2DS2-VASc score
9

10
The HAS-BLED bleeding risk score
*Hypertension is defined as systolic blood pressure > 160 mmHg. INR = international normalized ratio. 10

11
European Society of Cardiology (ESC)
CURRENT GUIDELINES…

19
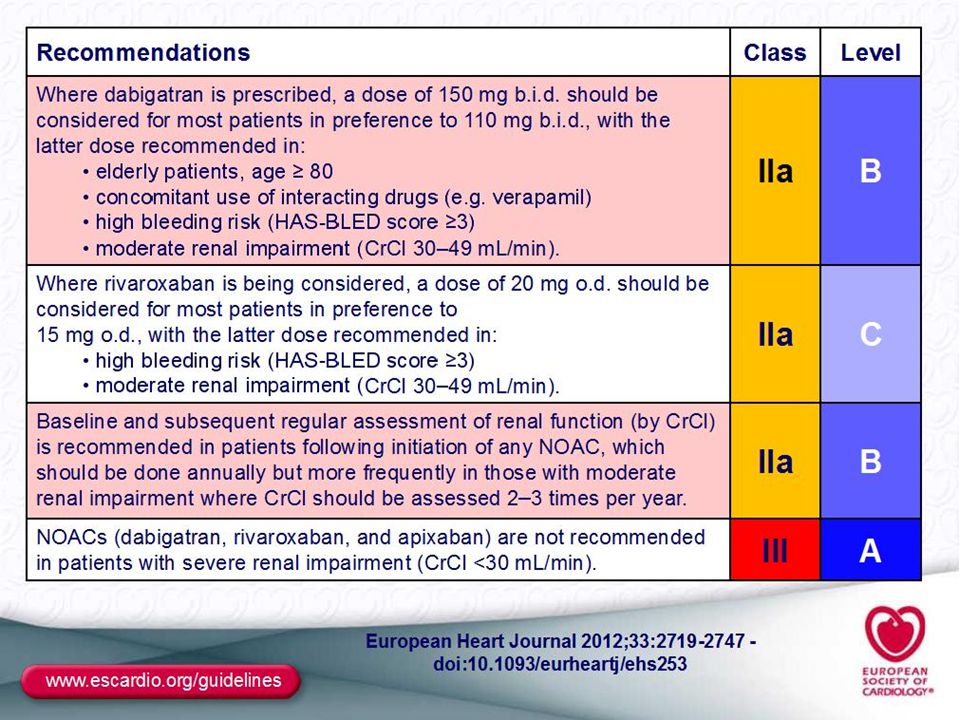
Choice of NOAC All have similar large studies with evidence of non- inferiority to warfarin. Dosing DABIGATRAN 150mg/110mg bd RIVAROXABAN 20mg/15mg od APIXABAN 5mg/2.5mg bd Reasons for reduced dose include Age >80 CrCl <50 for Dabigatran/Rivaroxaban CrCl <30 for Apixaban

20
Other Considerations Limit of CrCl Storage Drug interactions
Dabigatran 30 Rivaroxaban 15 Apixaban 15 Storage Dabigatran cannot be put into blister packs Drug interactions Amiodarone, Clarithromycin, Verapamil, ‘conazoles

21
Comparison of NOAC Trials
DABIGATRAN RIVAROXABAN APIXABAN patients 18,113 14,264 18,201 f/u 2 yrs 707 days 1.8 yrs Primary outcome (Hazard ratio) 150mg- 1.11% (0.66) 110mg- 1.53% (0.74) 1.7% (0.79) 1.27% Major bleeding 150mg- 3.11% (0.93) 110mg- 2.71% (0.69) 3.6% (vs 3.4%) 2.13% (0.69) Haemorragic stroke 150mg- 0.30% (0.41) 110mg- 0.23% (0.31) 0.5% (0.67) 0.24% (0.51) GI bleeding Higher
 150mg- 1.11% (0.66) 110mg- 1.53% (0.74) 1.7% (0.79) 1.27% Major bleeding. 150mg- 3.11% (0.93) 110mg- 2.71% (0.69) 3.6% (vs 3.4%) 2.13% (0.69) Haemorragic stroke. 150mg- 0.30% (0.41) 110mg- 0.23% (0.31) 0.5% (0.67) 0.24% (0.51) GI bleeding. Higher.")
22
Bleeding… There is no antidote… In Dabigatran dialysis may be helpful…
No clear evidence for use of Octiplex/Beriplex/Tranaxamic Acid…

23
Discontinuation of NOACs
“Hi is that the medics?… Surgeons here… just wanted some advice about…”

24
DISCONTINUATION OF DABIGATRAN
Timing of discontinuation after last dose of dabigatran before surgery Renal function Half-life Standard risk High risk (CrCl mL/min) (hours) of bleeding bleeding ≥ (11-22) 24 hours 2 days ≥ 50 to < (12-34) 24 – 48 hours 2-3 days >30 to < (13-23) 48 – 72 hours 4 days 30* 27 (22-35) 2 – 5 Days > 5 days *contra-indicated
 (hours) of bleeding bleeding. ≥ (11-22) 24 hours 2 days. ≥ 50 to < (12-34) 24 – 48 hours 2-3 days. >30 to < (13-23) 48 – 72 hours 4 days. 30* 27 (22-35) 2 – 5 Days > 5 days. *contra-indicated.")
25
DISCONTINUATION OF RIVAROXABAN
If an invasive procedure or surgical intervention is required, rivaroxaban should be stopped at least 24 hours before the intervention, if possible and based on the clinical judgement of the physician. If the procedure cannot be delayed the increased risk of bleeding should be assessed against the urgency of the intervention. Rivaroxaban should be restarted after the invasive procedure or surgical intervention as soon as possible provided the clinical situation allows and adequate haemostasis has been established.

26
DISCONTINUATION OF APIXABAN
Apixaban should be discontinued at least 48 hours prior to elective surgery or invasive procedures with a moderate or high risk of bleeding Apixaban should be discontinued at least 24 hours prior to elective surgery or invasive procedures with a low risk of bleeding including interventions for which any bleeding that occurs is expected to be minimal, non-critical in its location or easily controlled. If surgery or invasive procedures cannot be delayed, appropriate caution should be exercised, taking into consideration an increased risk of bleeding against the urgency of intervention. Apixaban should be restarted after the invasive procedure or surgical intervention as soon as possible provided the clinical situation allows and adequate haemostasis has been established.

Similar presentations














 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")










