Download presentation
Presentation is loading. Please wait.

1
A Rehospitalization Reduction Program on a Geriatric Skilled Nursing Unit Randi Berkowitz, MD Hebrew SeniorLife

2
Why decrease readmissions? I.Excellence in care – errors – patient satisfaction – staff satisfaction II.Financial – referrals – subacute beds long-term care – census – reimbursement/patient

3
Learning Objectives Define the scope of the issue of rehospitalization in subacute care nationally Describe innovative programs to reduce transfer out to the hospital Show how CQI process involving transfer can lower hospital readmission rates whole improving patient safety and quality of care

5
Large geographic variation

6
Hospital Readmissions within 30 days from SNFs are common Of ~1.8 million SNF admissions in the U.S. in 2006, 23.5% were re-admitted to an acute hospital within 30 days In Massachusetts the rate is 26% Cost of these readmissions = $4.3 billion

7
Common Reasons for Transfers Medical instability Availability of: On-site primary care providers Stat tests, IVs Inadequate assessments to identify early changes Communication gaps Family issues/preferences Lack of advance directives (DNR, DNH )
")
8
Do They Have to Go? As many as 45% of admissions of nursing home residents to acute hospitals may be inappropriate Saliba et al, J Amer Geriatr Soc 48:154-163, 2000 In 2004 in NY, Medicare spent close to $200 million on hospitalization of long- stay NH residents for “ambulatory care sensitive diagnoses” Grabowski et al, Health Affairs 26: 1753-1761, 2007

9
Adverse Events Common Coming and Going 46% of hospitalized patients have 1 or more regularly taken medications omitted without explanation. Potential for harm estimated at 39%. –Cornish Arch Int Med 2005; 165: 424-9 Transfers from NH to hospital have an average of 3 med changes. 20% lead to adverse drug events. –Boockvar Arch Int Med 2004 (164) 545-50
")
10
Conclusion Rehospitalizations are going to be a prime focus coming years New system paradigm will be needed to meet the demand for prevention of readmissions Focus of enhancing care in the SNF and community treatment will take precedence

11
It’s a new world Obamacare! Center for Medicare Medicaid Innovation $10 billion Triple aim –better health –better care –lower cost Innovation Advisors Program - Current fellow

12
How? 1.Admission 2.Stay on unit 3.Discharge

13
Bucket #1: Problems on Admission Ineffective communication of prognosis / options PCP out of loop Inadequate care plans for recurrent symptoms

14
Reduce AVOIDABLE hospital transfers Approach to the Problem: Admission MD standardized discussions Communication family and PCP High risk patients –Automatic Palliative Care consult –Flag for entire team

15
Bucket #2: Stay on Unit: Problems With Team Operation Disciplines operating in silos Failure to identify problems early Failure to learn from mistakes

16
Reduce AVOIDABLE hospital transfers Approach to the Problem: Stay on the Unit Team Improvement for the Patient and Safety (TIPS) conference Call to hospital Root cause analysis
 conference Call to hospital Root cause analysis")
17
Bucket #3: Problems With Home Discharge Poor hand off to next team No teach back with patient/HCP No standardized discharge summary/ nursing process

18
Reduce AVOIDABLE hospital transfers Approach to the Problem: Home Discharge Project RED –Written home care plan from electronic medical record –Making specific for geriatric use E.g. advance directives, diet, VNA, assistive devices Standardized discharge summaries

19
Target Population All admissions to the RSU subacute unit 1000 admissions a year 3NP/3MD- geriatric and palliative care certified

20
Process and Outcome Measures Admission –90% patients have discussion with MD Prognosis Rehospitalizations past 6 months Communication family and PCP –Patient/ family satisfaction survey

21
Advisory Committee Family Involvement - Daughter Outside institutions - Director Subacute Care- Partners Biostatistician Information Technologist Continuum - homecare Senior leadership at HSL Rabbi from palliative care Staff nurse, unit coordinator, therapy, social work, aide, administration

22
Process and Outcome Measures Middle - Stay on the unit –Unplanned discharge rates –Benchmarked staff safety survey for staff AHRQ –Attendance TIPS

23
Process and Outcome Measures Discharge Home 30 day readmission rates after discharge from SNF Satisfaction survey of discharge preparedness

24
Perceived Facilitators/Barriers Pt acceptance of less aggressive approaches Increased liability Increase cost keeping sicker patients Difficulty obtaining information from hospital Time needed to engage primary care Lack of practitioner access to computer systems in key referral sites Limited IT resources for Project RED

25
RSU Acute Transfer/Total Discharges

26
Data Unplanned Transfers January 2008- June 2009 compared with post TIPS July 2009-November 2009 Massachusetts 30 day 22-28% Pre-intervention16.5% Post-intervention13.3% Rate Reduction-20%

27
Pre and Post Discharge Dispositions Pre N=862 Community 68.6% Died1.2% LTC13.8% Hospital16.5% Post N=8863 73% 2.2% 11.6% 13.3%

28
When staff report something that could harm a resident, someone takes care of it Agree and Strongly Agree

29
On this unit, we talk about ways to keep incidents from happening again Agree and Strongly Agree

30
Staff ideas and suggestions are valued on this unit Agree and Strongly Agree

31
It is easy for staff to speak up about problems on this unit Agree and Strongly Agree

32
Staff feel like they are part of a team Agree and Strongly Agree

33
Staff are blamed when a resident is harmed Disagree and Strongly Disagree

34
Implications for HSL Family/patient involvement Create culture of system management rather than blame Share knowledge learned across sites/teams True multidisciplinary team- swarm the problem and front line solutions which can be used organizational wide Use of run/control charts to guide CQI into frontlines and understand common cause variability

35
Why take on this pain financially? Census, census, census Hospital care! CMS demonstration project Preferred provider network

36
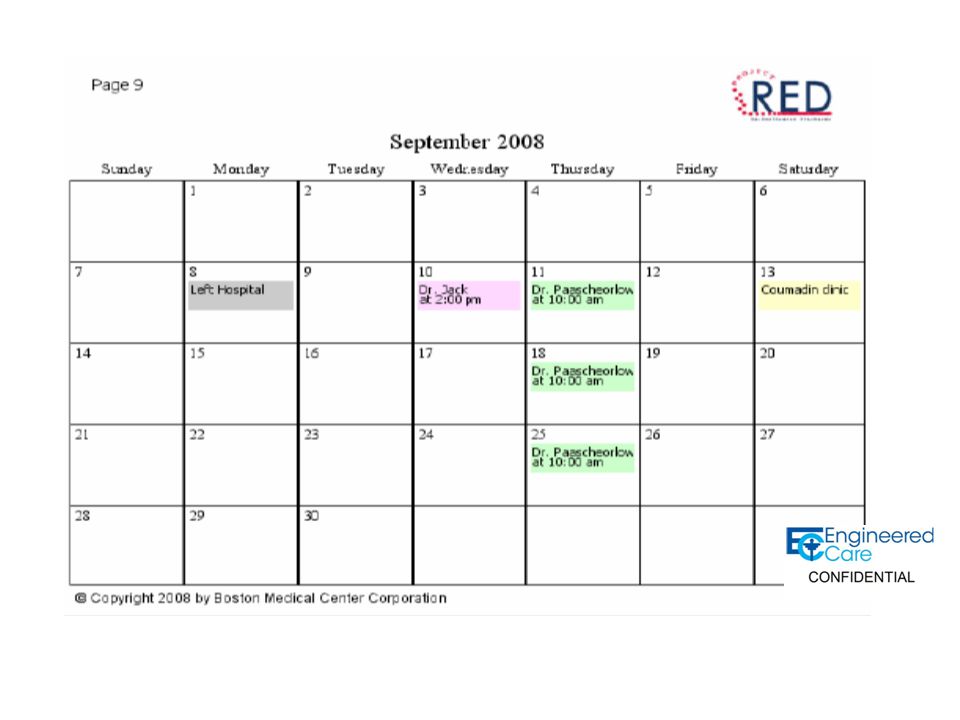
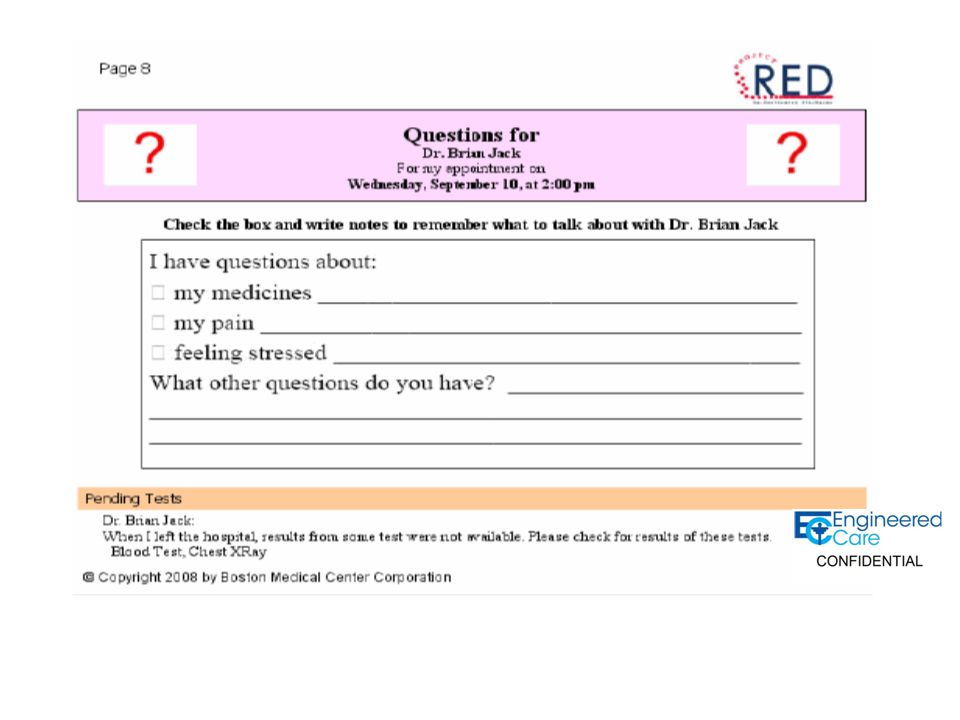
RED Computerized After Hospital Care Plan –Code status, meds, VNA info, PCP info, speech and therapy directions –Is Meditech good for something? –Phone number to call with questions with picture care coordinator and name –Give at first care plan meeting and on discharge update

44
RED Change culture patient/family empowerment Involvement of front line staff- NASA comparison Culture of QA and monthly feedback Clear numerical goals for entire team

45
Project RED Empowering the Patient Setting goals of January, 2011 How are we doing? How good EXACTLY do we want to be?

46
Respondents Reached 305 patients 96% 30 days after discharge RSU

47
Rehospitalization Once Home 56/302 patients 18.5% GOAL- We will reduce this to 15% or 2.7%

48
How many see PCP in 30 days? 171/282 60.6% GOAL - We will increase this to 75%.

49
Understood Medications Very Well or Extremely Well 216/279 77.4% GOAL- We will increase this to 80%

50
Understood Medications Very Well or Extremely Well 216/279 77.4% GOAL- We will increase this to 80%

51
How would you rate HSL? Respondents 263 Mean number scale 1-10 (10 the best) 8.55 GOAL- We will increase this to 9
 8.55 GOAL- We will increase this to 9.")
52
The life of a RED packet Given to patient approximately 1 week after admission (“rough draft”) Nurses use RED as a tool to help educate patients about their illness, meds, etc. “Final draft” is given to patient on discharge

53
RED Data – How are we doing? 90% of patients have been reached 13% of the intervention patients have been readmitted to a hospital or had a visit to the ER compared to 17.4% of the non- intervention patients

54
Data (cont.) 73.2% or RED patients saw their PCP within 30 days compared with 45.8% non- RED 92.5% understood their medications compared to 60.5%
 73.2% or RED patients saw their PCP within 30 days compared with 45.8% non- RED 92.5% understood their medications compared to 60.5%")
55
Data (cont.) 56.5% of patients were told of side effects for new medications, compared with 16.6%
 56.5% of patients were told of side effects for new medications, compared with 16.6%")
56
RED Problems Original plan was to for social workers give RED to patients Current plan is to have nurses deliver and teach RED to each patient

57
What are you all doing? Identify high risk patients Assessment versus actual interventions- all assessed and no where to go Sharing between systems- STAAR et al Communicating across continuum –Talking, data, funding

Similar presentations









 A Community Collaboration.>")




 MassPro February, 2013 2:30p-3:30p.>")









