Download presentation
Presentation is loading. Please wait.

1
Orbit, Lid and Lacrimal disorders
Dr Mahmood Fauzi Ansari ASSIST PROF OPHTHALMOLOGY AL MAAREFA COLLEGE

2
Objectives Review the clinical anatomy and physiology of Eyelids and Adenexa Describe disorders of eyelids (infections, malposition, tumors and congenital conditions) Describe disorders of lacrimal system (obstruction ,infection) Enumerate causes and management of Epiphora and Dry eye Outline Diagnosis and management of orbital infection Compare between pre-septal and septal cellulitis Develop the Differential diagnoses of Orbital Inflammatory Disease
 Describe disorders of lacrimal system (obstruction ,infection) Enumerate causes and management of Epiphora and Dry eye. Outline Diagnosis and management of orbital infection. Compare between pre-septal and septal cellulitis. Develop the Differential diagnoses of Orbital Inflammatory Disease.")
3
The orbit Function Anatomy protection to the globe
attachments which stabilize the ocular movement; transmission of nerves and blood vessels.

4
The orbit

5
The orbit

6
The orbit Clinical features of orbital disease
Eyelid and conjunctival changes Reduced visual acuity Pain Proptosis Enophthalmos Diplopia

7
Proptosis (exopthalmos)
Protrusion of the eye caused by a space-occupying lesion Measured with an exophthalmometer. 3 mm difference between the two eyes is significant. Direction of proptosis Transient proptosis (orbital varices) Fast onset proptosis (malignant, inflammatory) Slow onset proptosis (benign) Pain associated with proptosis ( orbital cellulitis)
 Fast onset proptosis (malignant, inflammatory) Slow onset proptosis (benign) Pain associated with proptosis ( orbital cellulitis)")
8
Thyroid ophthalmopathy
Clinical features Pathogenesis Proptosis (most common cause in adults) Lid retraction (characteristic stare) Lid lag Double vision Red painful eye (exposure) Reduced visual acuity (optic nerve) Disorders of the thyroid gland can be associated with an infiltration of the extraocular muscles with lymphocytes and the deposition of Glycosaminoglycans. An immunological process is suspected but not fully determined.
 Lid retraction (characteristic stare) Lid lag. Double vision. Red painful eye (exposure) Reduced visual acuity (optic nerve) Disorders of the thyroid gland can be associated with an infiltration of the extraocular muscles with lymphocytes and the deposition of Glycosaminoglycans. An immunological process is suspected but not fully determined.")
9
Grading system for thyroid associated ophthalmopathy
Pneumonic NO SPECS N: no signs O: only sign = upper lid retraction; Dalrymple S: soft tissue involvement (edema, chemosis, lagophthalmos) P: proptosis E: EOM involvement C: corneal involvement (SPK) S: sight loss (optic nerve compression)
 P: proptosis E: EOM involvement C: corneal involvement (SPK) S: sight loss (optic nerve compression)")
10
Thyroid Eye Disease

11
Thyroid ophthalmopathy

12
Thyroid ophthalmopathy
Treatment of associated ocular emergencies (optic nerve compression and corneal exposure) 1- systemic steroid 2- radiotherapy 3- orbital decompression 4- heavy lubrication Long term treatment Only after stabilization, muscle and lid surgery
 1- systemic steroid. 2- radiotherapy. 3- orbital decompression. 4- heavy lubrication. Long term treatment. Only after stabilization, muscle and lid surgery.")
13
Diplopia (Muscle pathology)
Thyroid ophthalmopathy (Graves’ ophthalmopathy) Idiopathic Orbital Inflammatory Disease( orbital pseudotumor)
 Idiopathic Orbital Inflammatory Disease( orbital pseudotumor)")
14
Enophthalmos Congenital (small eye) After trauma ( blow out fracture)
 After trauma ( blow out fracture)")
15
Orbital tumors Lacrimal gland tumors Optic nerve gliomas Meningiomas
Lymphomas Rhabdomyosarcoma (most common orbital malignancy in childhood) Metastasis from other systemic cancers (neuroblastomas in children, the breast, Lung, prostate or gastrointestinal tract in the adult).
 Metastasis from other systemic cancers (neuroblastomas in children, the breast, Lung, prostate or gastrointestinal tract in the adult).")
16
The orbital septum The orbital septum is the fascia behind that portion of the orbicularis muscle that lies between the orbital rim and the tarsus; it serves as a barrier between the lid and the orbit. The superior orbital septum blends with the tendon of the levator palpabrae superioris and the superior tarsus; the inferior orbital septum blends with the inferior tarsus.

17
Disorders of the Orbit- infections
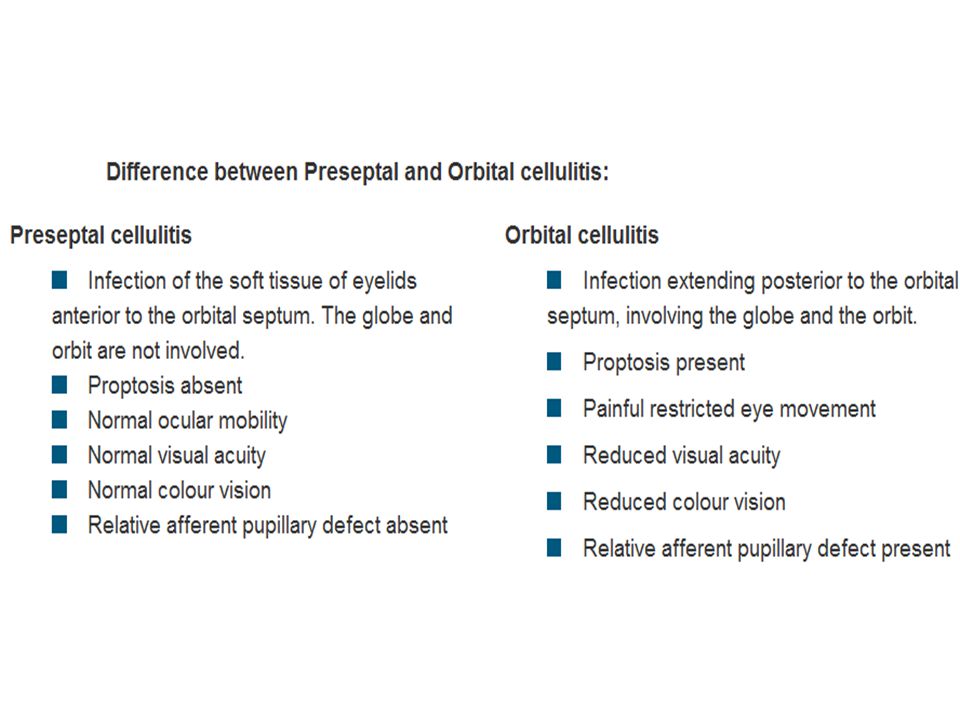
Pre-septal Cellulitis (Periorbital cellulitis) Post-septal Cellulitis (Orbital cellulitis)
 Post-septal Cellulitis (Orbital cellulitis)")
18
Orbital cellulitis

20
ORBITAL INFLAMMATORY DISEASE(OID)
Idiopathic/non specific orbital inflammatory disease - inflammation of the orbital tissues of unknown cause resulting in orbital pain, diplopia and proptosis Orbital myositis - inflammation of extraocular muscles, most commonly the superior or lateral rectus, causing orbital pain on movement of affected muscles, diplopia, proptosis Dacryoadenitis - inflammation of the lacrimal gland causing painful swollen lacrimal gland and reduced tear production; may be isolated or as part of diffuse idiopathic orbital inflammatory disease Wegener's granulomatosis - systemic small-vessel vasculitis characterised by necrotising granulomatous inflammation; c-ANCA positive in most cases; ocular involvement can include conjunctivitis, episcleritis, uveitis, retinal artery occlusion, nasolacrimal duct occlusion and optic nerve vasculitis.

21
(d) Tumour in region of the lacrimal gland, note S-shaped ptosis.
The differential diagnosis of OID includes infection, inflammation, and tumor. Orbital cellulitis in patient who presented with acute onset orbital inflammation post-foreign body. (b) Idiopathic OID in patient who presented with acute onset of orbital inflammation. (c) Thyroid orbitopathy in patient who presented with a several months history of increasing proptosis. (d) Tumour in region of the lacrimal gland, note S-shaped ptosis.
 Idiopathic OID in patient who presented with acute onset of orbital inflammation. (c) Thyroid orbitopathy in patient who presented with a several months history of increasing proptosis. (d) Tumour in region of the lacrimal gland, note S-shaped ptosis.")
22
Anatomy and Physiology of the Eyelids and Adnexa
The eyelids are composed of several layers of tissue which protect the anterior eyeball. From superficial to deep, they are the skin layer, a layer of striated muscle (orbicularis oculi), areolar tissue, fibrous tissue (tarsal plates), and a layer of mucous membrane (palpebral conjunctiva). The main supporting structure of the eyelids is a dense fibrous tissue layer, called the tarsal plate. The palpebral conjunctiva is the mucous membrane which adheres firmly to the tarsal plates and lines the posterior eyelids. The sensory nerve supply to the eyelids is derived from the first and second divisions of the trigeminal nerve (V). The blood supply to the lids is derived from the lacrimal and ophthalmic arteries by their lateral and medial palpebral branches.
, areolar tissue, fibrous tissue (tarsal plates), and a layer of mucous membrane (palpebral conjunctiva). The main supporting structure of the eyelids is a dense fibrous tissue layer, called the tarsal plate. The palpebral conjunctiva is the mucous membrane which adheres firmly to the tarsal plates and lines the posterior eyelids. The sensory nerve supply to the eyelids is derived from the first and second divisions of the trigeminal nerve (V). The blood supply to the lids is derived from the lacrimal and ophthalmic arteries by their lateral and medial palpebral branches.")
23
Layers of eyelid

24
Muscles of eyelids

25
The lid margins are divided into the anterior and posterior margins at the mucocutaneous junction.
Glands of Zeis and glands of Moll are both found on the anterior margin. Glands of Zeis are small, modified sebaceous glands that open into the hair follicles at the base of the eyelashes; whereas glands of Moll are modified sweat glands that open in a row near the base of the eyelashes. The posterior lid margin is in close contact with the globe, and along this margin are the small orifices of modified sebaceous glands, called meibomian glands.

26
Summary of Eyelid Pathology

27
Disorders of the Eyelids
EYELID INFECTIONS Blepharitis: Inflammation of lid margins

28
Anterior blepharitis

29
Posterior Blepharitis
Involving the meibomian gland orifices (meibomitis) Associated with acne rosacea Symptoms: similiar to anterior blepharitis Signs: thickening and telangiectasia of lid margins, decreased tear break-up time, rosacea Management Lid massage after heat Topical antibiotics/steroids Tear film supplements Systemic tetracyclines in persistent or severe cases
 Associated with acne rosacea. Symptoms: similiar to anterior blepharitis. Signs: thickening and telangiectasia of lid margins, decreased tear break-up time, rosacea. Management. Lid massage after heat. Topical antibiotics/steroids. Tear film supplements. Systemic tetracyclines in persistent or severe cases.")
30
LID LUMPS

31
Anterior Lamella External hordeolum (stye) - acute abscess within lash follicle and its associated glands of Moll or Zeis Signs: tender, warm, swollen, red eyelid lump Management - warm compression, topical antibiotic; add oral antibiotic in preseptal cellulitis Cyst of Moll - translucent cyst arises from blockage of gland of Moll (apocrine sweat gland) Cyst of Zeis - poorly translucent cyst arises from blockage of gland of Zeis (modified sebaceous gland) Xanthelasma - deposition of lipids within perivascular xanthoid cells which may be idiopathic or associated with hyperlipidaemia, hypothyroidism or primary biliary cirrhosis.
 Cyst of Zeis - poorly translucent cyst arises from blockage of gland of Zeis (modified sebaceous gland) Xanthelasma - deposition of lipids within perivascular xanthoid cells which may be idiopathic or associated with hyperlipidaemia, hypothyroidism or primary biliary cirrhosis.")
32
Posterior Lamella Internal hordeolum - acute abscess within a meibomian gland resulting in tender lump with inflammation Usually caused by Staphylococcus aureus Management - warm compression, oral antibiotics in preseptal cellulitis Chalazion - chronic lipogranulomatous inflammation of blocked meibomian glands. Often evolving from an internal hordeolum Common in patients with chronic marginal blepharitis, rosacea, seborrhoeic dermatitis. Management - small chalazion tends to resolve itself; persistent and symptomatic chalazion can be surgically removed by incision and curettage.

33
Ptosis - Abnormally low position of the upper lid
EYELID MALPOSITION Ectropion - Abnormal eversion of eyelid (usually the lower) away from the globe Entropion - Abnormal inversion of eyelid (usually lower) towards the globe Ptosis - Abnormally low position of the upper lid Horner's Syndrome (ptosis+meiosis+anhydrosis+enopthalmos)
 away from the globe. Entropion - Abnormal inversion of eyelid (usually lower) towards the globe. Ptosis - Abnormally low position of the upper lid. Horner s Syndrome. (ptosis+meiosis+anhydrosis+enopthalmos)")
34
Ectropion Abnormal eversion of eyelid (usually the lower) away from the globe Congenital - rare Paralytic - due to orbicularis weakness secondary to seventh cranial nerve palsy Involutional - due to age-related tissue laxity Cicatricial - due to shortened anterior lamella resulting from scarring Mechanical Management Lubricants and artificial tears Taping lower and upper eyelids together overnight Corrective surgery

35
Entropion Congenital - rare
Acute spastic - caused by sustained eyelid orbicularis contraction secondary to ocular irritation Involutional - due to inferior refractor dysfunction/tissue laxity Cicatricial - due to shortened posterior lamella resulting from scarring Management Taping eyelid to the cheek Botulinum injection Corrective surgery

36
Ptosis Management Involutional/aponeurotic ptosis –
most common form of ptosis; arises from disinsertion, dehiscence or attenuation of levator palpebrae superioris Neurogenic ptosis - third nerve palsy (dilated pupil, inability to elevate and adduct the globe), Horner's syndrome (constricted pupil; partial ptosis due to weakness of Muller's muscle) Myasthenic ptosis - Myasthenia gravis (fatiguable ptosis) Myopathic ptosis - chronic progressive external ophthalmoplegia, myotonic dystrophy Mechanical ptosis - masses, infiltration, oedema of upper lid Dermatochalasis (a form of pseudoptosis) - excess skin of upper lids Management Conservative Surgery - depending on the amount and type of ptosis, degree of levator function. There are three main approaches including anterior (transcutaneous/external) posterior (transconjunctival/internal) brow/frontalis suspension surgery
, Horner s syndrome (constricted pupil; partial ptosis due to weakness of Muller s muscle) Myasthenic ptosis - Myasthenia gravis (fatiguable ptosis) Myopathic ptosis - chronic progressive external ophthalmoplegia, myotonic dystrophy. Mechanical ptosis - masses, infiltration, oedema of upper lid. Dermatochalasis (a form of pseudoptosis) - excess skin of upper lids. Management Conservative. Surgery - depending on the amount and type of ptosis, degree of levator function. There are three main approaches including anterior (transcutaneous/external) posterior (transconjunctival/internal) brow/frontalis suspension surgery.")
37
Viral Infections Treatment Varicella zoster –
Widespread vesicular rash, primarily affecting the head neck and trunk. Reactivation of virus gives rise to shingles Herpes zoster ophthalmicus(shingles) Occurring in the first division of the trigeminal nerve Characteristic unilateral maculopapular rash, Associated with marked pain and systemic malaise (1 week prior to the development of the rash) Common in older patient . Hutchinson's sign: cutaneous involvement of the tip of the nose suggests an increased likelihood of ocular complications). Treatment Systemic Antivirals (eg famciclovir ) Management of lid involves cool compresses and topical lubrication ± topical antibiotics for secondary infections Herpes simplex primary infection is usually not clinically apparent unless occurring in the neonate or when associated with immunodeficiency. Secondary infection frequently manifests as a dendritic corneal ulcer
 Occurring in the first division of the trigeminal nerve. Characteristic unilateral maculopapular rash, Associated with marked pain and systemic malaise (1 week prior to the development of the rash) Common in older patient . Hutchinson s sign: cutaneous involvement of the tip of the nose suggests an increased likelihood of ocular complications). Treatment. Systemic Antivirals (eg famciclovir ) Management of lid involves cool compresses and topical lubrication ± topical antibiotics for secondary infections. Herpes simplex. primary infection is usually not clinically apparent unless occurring in the neonate or when associated with immunodeficiency. Secondary infection frequently manifests as a dendritic corneal ulcer.")
38
Malignant tumours Basal cell carcinoma (rodent ulcer)
>90% of all neoplastic eye lesions Frequently occurs on the lower lid Indurated Plaque ± Lid distortion and Lash Abnormalities. Treatment is with wide local excision. Is Basal Cell Carcinoma Serious? …Yes, Basal Cell Carcinoma can kill if left untreated.

39
Sebaceous Gland Carcinoma
accounts for 5% of all malignant eyelid tumors. can originate from Meibomian glands, Zeis glands or the sebaceous glands of the caruncle. more common in the upper eyelid Squamous cell carcinoma accounts for ~2-5% of lid malignancies The tumour tends to occur on the lower lid at the margin, commonly in fair-skinned elderly people with a history of sun exposure. Plaque-like (rough, scaly erythematous patch), nodular or ulcerating with a sharply defined base and everting borders. It can be aggressive: refer early if you suspect this.
, nodular or ulcerating with a sharply defined base and everting borders. It can be aggressive: refer early if you suspect this.")
40
Congenital disorders of the lid
vertical folds of skin extending from the upper eyelids to the side of the nose These are NORMAL features in Orientals. Epicanthic folds Coloboma -uncommon condition of a partial or full thickness defect of the lid -associated with systemic conditions such as Treacher Collins' syndrome. -Treatment is surgical. Cryptophthalmos – failure of lid development

41
The lacrimal system

42
The lacrimal drainage system

43
Disorders of the Lacrimal System
CONGENITAL OBSTRUCTION OF THE NASOLACRIMAL SYSTEM Nasolacrimal duct obstruction Dacryocystocele INFECTIONS OF THE LACRIMAL SYSTEM Canaliculitis: Acute Dacryocystitis:

44
NLD obstruction

45
Congenital NLD obstruction
5% of all full-term newborns. 90% open spontaneously in the first year of life. Tx: massage and antibiotics drops if infected. Sometimes need probing and tubing

46
Adult NLD obstruction

47
Dacryocystitis

49
Nasolacrimal duct obstruction, right eye
Nasolacrimal duct obstruction, right eye. Note the build-up of tears and mucous along the lower lid margin. Congenital dacryocystocele of the lacrimal sac in a newborn baby. A dacryocystocele is located just inferior to the medial canthus and presents as a purplish or greyish-blue swelling.

51
These structures are involved in the production and drainage of tears.
The lacrimal puncta, canaliculi, and sac, and the nasolacrimal duct form the drainage system, ultimately draining into the nose. The nose is lined by a highly vascular mucosal epithelium; consequently, topically applied medications that pass through this nasolacrimal system have direct access to the systemic circulation. Valve-like folds of the epithelial lining of the duct, called the valve of Hasner tend to resist the retrograde flow of tears and air. When the structure is imperforate, it is the most common cause of congenital nasolacrimal duct obstruction, resulting in epiphora and chronic dacryocystitis The lacrimal apparatus consists of the lacrimal gland, accessory lacrimal gland, lacrimal puncta, lacrimal canaliculi, lacrimal sac and nasolacrimal duct. These structures are involved in the production and drainage of tears. The blood supply of the lacrimal gland is derived from the lacrimal artery. The lymphatic drainage drain into the pre-auricular lymph nodes. The nerve supply of the lacrimal gland is by the lacrimal nerve (sensory), a branch of the trigeminal first division, the great petrosal nerve (parasympathetic secretory), which comes from the superior salivary nucleus and is a branch of the facial nerve; and sympathetic nerves accompanying the lacrimal artery and the lacrimal nerve.
, a branch of the trigeminal first division, the great petrosal nerve (parasympathetic secretory), which comes from the superior salivary nucleus and is a branch of the facial nerve; and sympathetic nerves accompanying the lacrimal artery and the lacrimal nerve.")
52
Any abnormality of one of the three layers produces an unstable tear film and the symptoms of dry eyes. A tear Layer frequently affected is the Aqueous Layer, Resulting in Aqueous Tear Deficiency (ATD) or lacrimal hyposecretion.
 or lacrimal hyposecretion.")
53
A tearing eye may be a nuisance but usually is not a serious problem.
Epiphora- watery eyes A tearing eye may be a nuisance but usually is not a serious problem. Successful management of the tearing patient requires the clinician to determine the underlying cause of the epiphora. Common causes of watery eyes include: Blepharitis(eyelid inflammation) Blocked tear duct Common cold Ectropion (outwardly turned eyelid) Entropion (inwardly turned eyelid) Foreign object in the eye Hay fever Infection of the tear duct Ingrown eyelash (trichiasis) Irritation of the cornea (front of the eye) conjunctivitis Trachoma some times, dry eye can be a contributing factor Medications that can cause watery eyes include: Epinephrine , Chemotherapy drugs, Cholinergic agonists, Eyedrops, especially echothiophate iodide (Phospholine Iodide) and pilocarpine Managing the ‘Tearing’ patient Dilation, punctoplasty, silicone intubation
 Blocked tear duct. Common cold. Ectropion (outwardly turned eyelid) Entropion (inwardly turned eyelid) Foreign object in the eye. Hay fever. Infection of the tear duct. Ingrown eyelash (trichiasis) Irritation of the cornea (front of the eye) conjunctivitis. Trachoma. some times, dry eye can be a contributing factor. Medications that can cause watery eyes include: Epinephrine , Chemotherapy drugs, Cholinergic agonists, Eyedrops, especially echothiophate iodide (Phospholine Iodide) and pilocarpine. Managing the ‘Tearing’ patient. Dilation, punctoplasty, silicone intubation.")
54
Dry eye Dry eye syndrome can occur if your eyes do not produce enough tears or your tears evaporate too quickly Symptoms of dry eye: Pain ,Light sensitivity, A gritty sensation, A feeling of a foreign body or sand in the eye,Itching,Redness Blurring of vision (Without tear film, good vision not possible.) What Causes Dry Eyes? The natural aging process, especially menopause Side effects of certain drugs such as antihistamines and birth control pills Diseases that affect the ability to make tears, such as Sjogren's syndrome, rheumatoid arthritis, and collagen vascular diseases Structural problems with the eyelids that don't allow them to close properly Managing the dry eye Artificial tear drops and ointments. Temporary punctal occlusion Lipiflow. use heat and pressure on the eyelids to unclog blocked glands. Restasis. (Cyclosporine Ophthalmic Emulsion) 0.05% increases eyes’ natural ability to produce tears, in Chronic Dry Eye. RESTASIS® did not increase tear production in patients using anti-inflammatory eye drops or tear duct plugs
 What Causes Dry Eyes The natural aging process, especially menopause. Side effects of certain drugs such as antihistamines and birth control pills. Diseases that affect the ability to make tears, such as Sjogren s syndrome, rheumatoid arthritis, and collagen vascular diseases. Structural problems with the eyelids that don t allow them to close properly. Managing the dry eye. Artificial tear drops and ointments. Temporary punctal occlusion. Lipiflow. use heat and pressure on the eyelids to unclog blocked glands. Restasis. (Cyclosporine Ophthalmic Emulsion) 0.05% increases eyes’ natural ability to produce tears, in Chronic Dry Eye. RESTASIS® did not increase tear production in patients using anti-inflammatory eye drops or tear duct plugs.")
55
Useful Resources Diagnosis and Management of Eyelids and Lacrimal Abnormalities. External Eye Overview - Lashes, eyelids and lacrimal system. Eyelids, Orbit and Lacrimal System.

Similar presentations












 Ahmed Almohammed 291100030 Advisor : Prof. Dr. Osama El-Bassiouny Ophthalmology course.>")








