Download presentation
Presentation is loading. Please wait.

1
Endocannabinoids: Basic Physiology and Function Eliot L. Gardner New York Society of Addiction Medicine 7th Annual Conference NYC - February 2011 Eliot L. Gardner, Ph.D. Chief, Neuropsychopharmacology Section Intramural Research Program National Institute on Drug Abuse National Institutes of Health egardner@intra.nida.nih.gov443.740.2516

2
Cannabis Many species exist: Cannabis Sativa (European plant), Cannabis indica (Indian plant) and Cannabis ruderalis (Siberia and central Asia plant) 460 known chemical constituents of cannabis 66 constituents have a cannabinoid structure Δ 9 -THC most important constituent: principal psychoactive component of cannabis Many species exist: Cannabis Sativa (Europe), Cannabis Indica (India) and Cannabis ruderalis (Siberia and central Asia) 460 known chemical constituents of cannabis 66 constituents have a cannabinoid structure Δ 9 -Tetrahydrocannabinol (Δ 9 -THC or THC) most important constituent Δ 9 -THC is the principal psychoactive component of cannabis
, Cannabis indica (Indian plant) and Cannabis ruderalis (Siberia and central Asia plant) 460 known chemical constituents of cannabis 66 constituents have a cannabinoid structure Δ 9 -THC most important constituent: principal psychoactive component of cannabis Many species exist: Cannabis Sativa (Europe), Cannabis Indica (India) and Cannabis ruderalis (Siberia and central Asia) 460 known chemical constituents of cannabis 66 constituents have a cannabinoid structure Δ 9 -Tetrahydrocannabinol (Δ 9 -THC or THC) most important constituent Δ 9 -THC is the principal psychoactive component of cannabis")
4
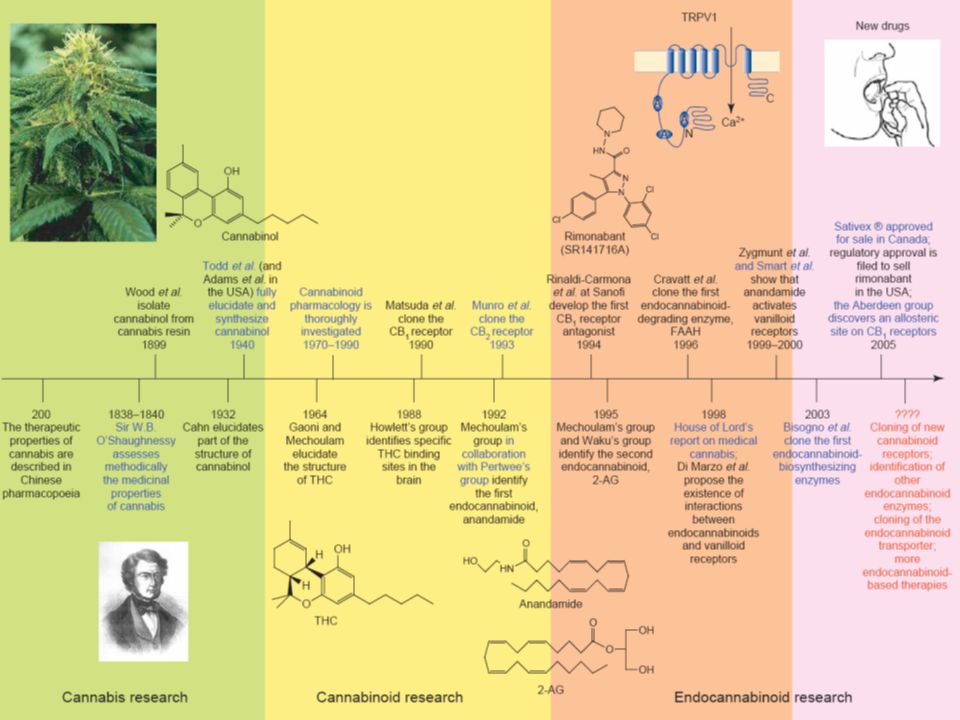
Era of Cannabis Research: 200-1940 ● Circa 200 AD: Therapeutic properties of cannabis described in Chinese pharmacopoeia ● 1838-1840: Sir W.B. O’Shaughnessy methodically assesses medicinal properties of cannabis, and publishes findings ● 1899: Wood et al. isolate cannabinol from cannabis resin ● 1932: Cahn elucidates part of the structure of cannabinol ● 1940: Todd et al. and Adams et al. simultaneously elucidate the full structure of cannabinol and successfully synthesize it

5
Era of Cannabinoid Research: 1960-1994 ● 1960: Mechoulam (Hebrew University) identifies THC as the principal psychoactive component of cannabis ● 1964: Gaoni and Mechoulam (Hebrew University) elucidate the chemical structure of THC ● 1970-1990: Cannabinoid pharmacology is thoroughly studied ● 1985: Gardner shows cannabinoid-opioid interaction in brain ● 1986: Gardner shows THC activates brain-reward systems ● 1988: Howlett’s group finds specific THC binding sites in brain ● 1990: Matsuda et al. clone the CB1 receptor ● 1992: Mechoulam’s group (Hebrew University) in collaboration with Pertwee’s group (Scotland) identify the first endocannabi- noid – Mechoulam names it “anandamide” from the Sanskrit word “anand” meaning “bliss” ● 1993: Munro et al. clone the CB2 receptor
 in collaboration with Pertwee’s group (Scotland) identify the first endocannabi- noid – Mechoulam names it anandamide from the Sanskrit word anand meaning bliss ● 1993: Munro et al. clone the CB2 receptor.")
6
Era of Endocannabinoid Research: 1994-2000 ● 1994: Scientists at Sanofi Recherche (France) develop the first CB1 receptor antagonist – SR141716A (Rimonabant) ● 1995: Mechoulam (Hebrew University) isolates and identifies the second endocannabinoid – 2-Arachidonoylglycerol (2-AG) ● 1996: Cravatt et al. (Scripps) clone the first endocannabinoid degrading enzyme – fatty acid amide hydrolase (FAAH) ● 1998: House of Lords report on medical cannabis ● 1998: Di Marzo et al. propose interactions between endocan- nabinoids and vanilloid receptors ● 1999: Zygmunt et al. and Smart et al. show that anandamide activates vanilloid receptors
 clone the first endocannabinoid degrading enzyme – fatty acid amide hydrolase (FAAH) ● 1998: House of Lords report on medical cannabis ● 1998: Di Marzo et al. propose interactions between endocan- nabinoids and vanilloid receptors ● 1999: Zygmunt et al. and Smart et al. show that anandamide activates vanilloid receptors.")
7
Current Endocannabinoid Research: 2000- ● 2003: Bisogno et al. clone the first endocannabinoid bio- synthesizing enzymes ● 2005: Pertwee et al. (Scotland) discovers an allosteric site on CB1 receptors ● 2005: Sativex ® approved for sale in Canada ● 2010: Gardner shows psychoactive (and potentially therapeu- tic) effects of cannabidiol ● ????: Discovery of new cannabinoid receptors ● ????: Discovery of new endocannabinoids ● ????: Discovery of new endocannabinoid enzymes ● ????: Cloning of new endocannabinoid transporters ● ????: Discovery of new cannabinoid-based therapies
 discovers an allosteric site on CB1 receptors ● 2005: Sativex ® approved for sale in Canada ● 2010: Gardner shows psychoactive (and potentially therapeu- tic) effects of cannabidiol ● : Discovery of new cannabinoid receptors ● : Discovery of new endocannabinoids ● : Discovery of new endocannabinoid enzymes ● : Cloning of new endocannabinoid transporters ● : Discovery of new cannabinoid-based therapies.")
8
What is a cannabinoid? Initially, compounds extracted by Cannabis spp producing characteristic psychoactivity Later, compounds with a characteristic terpenoid structure Currently, most any compound that produces cannabinoid psychoactivity, natural or synthetic Occasionally, just compounds that will interact with cannabinoid receptors

9
Natural cannabinoids

10
Representative cannabinoids Classical cannabinoidsNon-classical cannabinoidAminoalkylindole CB 1 antagonists

11
Anandamide 2-Arachidonoylglycerol O HO O O HN HO Noladin ether N-Arachidonoyldopamine O HO O HN HO O NH 2 O Virodhamine Endocannabinoids

12
Cannabinoid CB1 and CB2 Receptors

13
Characteristics of CB1 and CB2 Receptors Both densely distributed throughout the body CB1 highly enriched in central nervous system Located on axon terminals Mediate retrograde signaling (Dendrite → Axon) G-protein coupled CB2 highly enriched in periphery –Especially in immune system CB2 also in brain and CNS –Fewer than CB1; ~ Same density as μ opioid –Nonetheless, CB2s modulate neural signaling
 G-protein coupled CB2 highly enriched in periphery –Especially in immune system CB2 also in brain and CNS –Fewer than CB1; ~ Same density as μ opioid –Nonetheless, CB2s modulate neural signaling")
14
CB1 and CB2 Receptors not the only Receptors Activated by Cannabinoids Cannabidiol (CBD) receptors Transient Receptor Potential Cation V1 receptors (TRPV1; Capsaicin receptors) G-coupled Protein Receptor 55 (GPR55) G-coupled Protein Receptor 119 (GPR119) Peroxisome Proliferator-Activated receptors (PPARs) Others
 receptors Transient Receptor Potential Cation V1 receptors (TRPV1; Capsaicin receptors) G-coupled Protein Receptor 55 (GPR55) G-coupled Protein Receptor 119 (GPR119) Peroxisome Proliferator-Activated receptors (PPARs) Others")
15
CB 1 Ca 2+ K+K+ 5-HT 3 AC ATP AMPc MAPK PKA Gene expression AA NO NA+/H+ exchanger NO Guindon, Beaulieu and Hohmann (2009) Pharmacology of the cannabinoid system, IASP Press CB1-Mediated Signal Transduction
 Pharmacology of the cannabinoid system, IASP Press CB1-Mediated Signal Transduction")
16
CB 1 localization Antibodies Distinctive pattern of distribution Cortex, hippocampus, basal ganglia, SN, cerebellum Low in thalamus and most of brainstem H.-C. Lu Eggan S. and Lewis D. Cerebral Cortex 2007; 17:175 Monkey Mouse

17
CB 1 receptor localization (hippocampus) mRNAprotein István Katona In the forebrain, the majority of CB 1 protein arises from a minority of interneuons (CCK + GABAergic)
 mRNAprotein István Katona In the forebrain, the majority of CB 1 protein arises from a minority of interneuons (CCK + GABAergic)")
18
CB 1 receptor localization (hippocampus) protein Jim Wager-Miller CB 1 heavily expressed on some axons & terminals István Katona EM
 protein Jim Wager-Miller CB 1 heavily expressed on some axons & terminals István Katona EM")
19
CB 1 receptor localization (VTA) István Katona CB 1 expressed on two populations of terminals Functionally, multiple VTA synapses are modulated by cannabinoids
 István Katona CB 1 expressed on two populations of terminals Functionally, multiple VTA synapses are modulated by cannabinoids")
20
CB 1 agonists modulate neurotransmission The signaling pathways of CB1 suggest cannabinoids might decrease neurotransmission: Inhibition of calcium channel, adenylyl cyclase Activation of potassium channels, MAP kinase Appropriate localization of the receptors Multiple studies show inhibition of neurotransmitter release

21
CB 1 agonists modulate neurotransmission CB 1 receptor activation inhibits evoked GABA IPSC’s Hájos Measure GABAergic currents in CA1 record VcVc stimulate Typical experiment: Hippocampal slices Patch clamp recording Bath apply drugs

22
CB 1 receptor summary Abundantly expressed throughout the brain Majority on axons and synaptic terminals Primarily G i/o coupled (not only!) CB 1 activation inhibits synaptic transmission
 CB 1 activation inhibits synaptic transmission")
23
Endogenous cannabinoids Receptors suggest endogenous ligands Two main families identified Both arachidonic acid derivatives Precursors in membranes “Made on demand” Amides (anandamide) Esters (2-AG) Significant differences –Routes of synthesis –Mode of degradation (FAAH vs MAGL) –Efficacy
 Esters (2-AG) Significant differences –Routes of synthesis –Mode of degradation (FAAH vs MAGL) –Efficacy")
25
CB1 agonist efficacy is variable Many studies have found 2-AG to be more efficacious than anandamide (or THC) at CB1 (GIRK activation in oocytes shown here) Luk, et al, 2004 2-AG MEA THC
 at CB1 (GIRK activation in oocytes shown here) Luk, et al, AG MEA THC")
26
eCB summary Acyl ethanolamides (diverse; anandamide, AEA) More promiscuous --- many targets Acyl glycerol esters (2-AG) Both are “Made on demand” 2-AG ~100x more bulk levels, similar “signaling”(?) Differing efficacies Metabolic diversity, with “core” pathways
 More promiscuous --- many targets Acyl glycerol esters (2-AG) Both are Made on demand 2-AG ~100x more bulk levels, similar signaling ( ) Differing efficacies Metabolic diversity, with core pathways")
27
What are the physiological effects of eCB’s on neuronal activity? Exogenous cannabinoids inhibit neurotransmission eCB’s are synthesized following increases in intracellular calcium and/or activation of G q/11 - linked receptors Might eCB’s synthesized in this fashion modulate neurotransmission? Yes Transient effects Long lasting effects

28
Six Types of eCB-Mediated Synaptic Plasticity Have Been Clearly Identified Depolarization-induced suppression of inhibition Depolarization-induced suppression of excitation Metabotropic-induced suppression of inhibition Metabotropic-induced suppression of excitation Long-Term Depression (LTD) Slow self-inhibition (SSI) Additional types are being constantly discovered
 Slow self-inhibition (SSI) Additional types are being constantly discovered")
29
Important Take-Home Messages Endocannabinoids are neurotransmitters Cannabinoids (e.g., THC) modulate neural activity Endocannabinoids are involved in synaptic re- modeling Cannabinoids (e.g., THC) can modulate synaptic re- modeling Depending upon the specific CNS circuits involved, cannabinoids can have a host of actions on brain, cognition, and behavior (some beneficial, some not)
 modulate neural activity Endocannabinoids are involved in synaptic re- modeling Cannabinoids (e.g., THC) can modulate synaptic re- modeling Depending upon the specific CNS circuits involved, cannabinoids can have a host of actions on brain, cognition, and behavior (some beneficial, some not)")
30
Cannabinoids and pain ● central ● spinal ● periphery

31
Ständer et coll. J Dermatol Sci 2005 Hohmann & Herkenham Neuroscience 1999 Bridges et coll. Neuroscience 2003 Peripheral and spinal localization of cannabinoid receptors Farquhar-Smith et coll. Mol Cell Neurosci 2000

32
Ca 2+ K+K+ Neurotransmitter vesicles ET PLC AEA AA COX PG 2-AG MGL CB 1 DAGL Phospholipid DAG NAT ? NAPE NAPE- PLD ? FAAH Postsynaptic neuron Presynaptic neuron Ca 2+ Microglia CB 2 Phospholipid NAT NAPE AEA Phospholipid NAPE- PLD ? Guindon et al., (2009) Pharmacology of the cannabinoid system, IASP Press
 Pharmacology of the cannabinoid system, IASP Press.")
33
Evaluation of nociceptive behavior in the formalin test Time (min) Pain score Injection 50 µL Formaline 2.5 %
 Pain score Injection 50 µL Formaline 2.5 %")
34
Peripheral Antinociceptive Effects Composite Pain Score (CPS) Time (min) † # † AUC (0-15) P < 0.05 and # AUC (15-60) P < 0.001 for analgesics vs NaCl 0.9 % contralateral ipsilateral
 Time (min) † # † AUC (0-15) P < 0.05 and # AUC (15-60) P < for analgesics vs NaCl 0.9 % contralateral ipsilateral")
35
Synergistic effect of anandamide + ibuprofen Guindon et al. (2006) Pain 121: 85-93 Log dose (µg) Dose Anandamide (µg) Pain (Area Under the Curve) Dose Ibuprofen (µg)
 Pain 121: Log dose (µg) Dose Anandamide (µg) Pain (Area Under the Curve) Dose Ibuprofen (µg).")
36
Synergistic effect of anandamide + rofecoxib 0 0.05 0.1 0.15 0.2 00.0050.010.015 Anandamide Rofecoxib Mix 1:10 Add 1:10 Guindon et al. (2006) European Journal of Pharmacology 550: 58-77 Dose Anandamide (µg) Dose Rofecoxib (µg) Log dose (µg) Pain (Area Under the Curve)
 European Journal of Pharmacology 550: Dose Anandamide (µg) Dose Rofecoxib (µg) Log dose (µg) Pain (Area Under the Curve).")
37
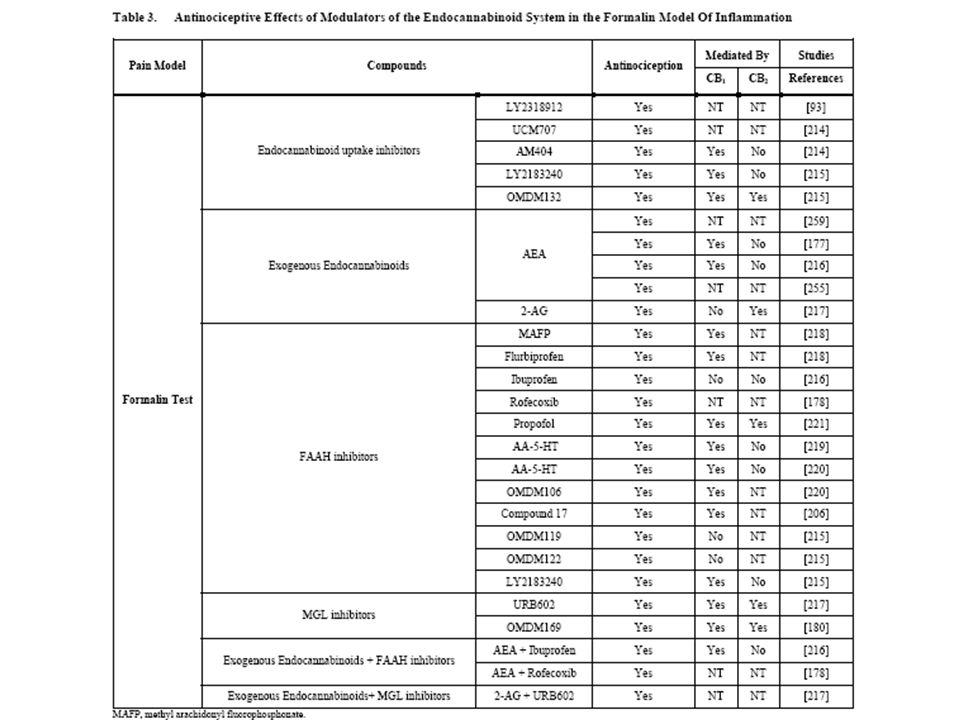
Objectives of 2-AG, JZL184 and URB602 study Compare the peripheral antinociceptive effects of 2-AG, JZL184, URB602 and their combination in the formalin test Study the mechanisms by which JZL184 and URB602 produce their effects using specific CB 1 and CB 2 receptor antagonists

38
† # Composite Pain Score (CPS) Time (min) Peripheral Antinociceptive Effects ipsilateral contralateral † P < 0.001 and # P < 0.001 for URB602 (500 µg) vs NaCl 0.9 %
 Time (min) Peripheral Antinociceptive Effects ipsilateral contralateral † P < and # P < for URB602 (500 µg) vs NaCl 0.9 %")
39
Peripheral Antinociceptive Effects Composite Pain Score (CPS) Time (min) † # † P < 0.001 and # P < 0.001 for JZL184 ((300 µg) vs NaCl 0.9 % ipsilateral contralateral
 Time (min) † # † P < and # P < for JZL184 ((300 µg) vs NaCl 0.9 % ipsilateral contralateral")
40
JZL184 with cannabinoid antagonists Inflammatory Phase * P < 0.001 for JZL184 (10 µg) vs Vehicle Area Under the Curve *
 vs Vehicle Area Under the Curve *")
41
* URB602 with cannabinoid antagonists Area Under the Curve Inflammatory Phase * P < 0.001 for URB602 (70 µg) vs NaCl 0.9 % Guindon et al. (2006) Brithish Journal of Pharmacology 150: 693-701
 Brithish Journal of Pharmacology 150:")
42
Conclusions JZL184, URB602, 2-AG and their combination reduce nociceptive behavior when given locally JZL184 is more potent than URB602 when given alone or combined with 2-AG Antinociceptive effects of JZL184 and URB602 are inhibited by AM251 and AM630

48
Cannabinoids and Addiction There is now an extensive published literature showing anti- addiction efficacy for cannabinoid ligands Gardner EL. Endocannabinoid signaling system and brain reward: emphasis on dopamine. Pharmacol Biochem Behav 81:263-284, 2005 De Vries TJ & Schoffelmeer AN. Cannabinoid CB1 receptors control conditioned drug seeking. Trends Pharmacol Sci 26:420-426, 2005 Cohen C et al. CB1 receptor antagonists for the treatment of nicotine addiction. Pharmacol Biochem Behav 81:387-395, 2005 Maldonado R et al. Involvement of the endocannabinoid system in drug addiction. Trends Neurosci 29:225-232, 2006 Basavarajappa BS. The endocannabinoid signaling system: a potential target for next-generation therapeutics for alcoholism. Mini-Revs Med Chem 7:769-779, 2007 Fattore L et al. Endocannabinoid regulation of relapse mechanisms. Pharmacol Res 56:418-427, 2007 Scherma M et al. The endocannabinoid system: a new molecular target for treatment of tobacco addiction. CNS & Neurol Disorders - Drug Targets 7:468-481, 2008 Paralaro D & Rubino T. The role of the endogenous cannabinoid system in drug addiction. Drug News Perspect 21:149-157, 2008

49
CB1 Antagonist-Induced Attenuation of Cocaine-Enhanced Brain Stimulation Reward

51
CB1 Antagonism Does Not Affect Motoric Ability

52
Cocaine ? Pump PR Schedule Reward Work Demand (# Infusion) (# Lever Press) 1 1 2 2 3 4 4 6 5 9 14 77 15 95 16 118 …. ….
 (# Lever Press) …. …..")
53
CB1 Antagonist-Induced Attenuation of Incentive Motivation to Self-Administer i.v. Cocaine – Representative Animal (Progressive-Ratio Model)
.")
54
CB1 Antagonist-Induced Attenuation of Incentive Motivation to Self-Administer i.v. Cocaine (Progressive-Ratio Model) AM251 (Original Break-Point) AM251 (% Change in Break-Point)
 AM251 (Original Break-Point) AM251 (% Change in Break-Point).")
55
CB1 Receptor Antagonism Dose-Dependently Attenuates Relapse to Cocaine-Seeking Behavior (Reinstatement Model)
")
56
CB1 Receptor Antagonism Does Not Attenuate Relapse to Non-Drug Reward-Seeking Behavior (Reinstatement Model)
")
57
CB1 Receptor Antagonist Micro-Injected Into Nucleus Accumbens Attenuates Cocaine-Seeking Behavior (Reinstatement Model)
")
58
CB1 Receptor Antagonism By Itself Does Not Produce Drug-Seeking Behavior (Reinstatement Model)
")
59
CB1 Receptor Antagonism Markedly Attenuates Cocaine- Enhanced Nucleus Accumbens Glutamate (Brain Microdialysis)
")
60
CB1 Receptor Antagonism Markedly Attenuates Cocaine Sensitization

61
CB1 Receptor Gene-Deletion (CB1 Gene Knock-Out) Abolishes Cocaine’s Psychostimulant Effects
 Abolishes Cocaine’s Psychostimulant Effects")
62
CB1 Receptor Gene-Deletion (CB1 Gene Knock-Out) Abolishes Cocaine-Enhanced Nucleus Accumbens Dopamine (Dialysis)
 Abolishes Cocaine-Enhanced Nucleus Accumbens Dopamine (Dialysis)")
63
CB1 Receptor Gene-Deletion (CB1 Gene KO) Attenuates Evoked Nucleus Accumbens Dopamine Release (Voltammetry)
 Attenuates Evoked Nucleus Accumbens Dopamine Release (Voltammetry)")
65
CB1 Antagonist SR141716 (Rimonabant) By Itself Markedly Inhibits Nucleus Accumbens Dopamine (Brain Microdialysis) Other CB1 Receptor Antagonists (Either Neutral Antagonists or Inverse Agonists) Do Not Do This !!
 By Itself Markedly Inhibits Nucleus Accumbens Dopamine (Brain Microdialysis) Other CB1 Receptor Antagonists (Either Neutral Antagonists or Inverse Agonists) Do Not Do This !!")
66
Caveats Regarding Development of Cannabinoid Agonists as Potential Pharmacotherapeutic Agents CB1 and CB2 receptors are ubiquitous throughout the body – Potential for numerous side effects Some cannabinoid ligands have poor bioavailability CB1 receptor agonists have addictive potential

67
Potential Cannabinoid Therapies - Tools Endocannab Uptake Inhibitors – AM404, UCM707, AM1172 FAAH Inhibitors – URB597, OL135, BMS1, SA47, PF750 MAGL Inhibitors – URB602, OMDM169, JZL184 Dual CB1/CB2 Agonists – WIN55512, CP55940, HU210 Anandamide Analogues – Methanandamide, Metfluoroanand. Selective CB1 Agonists – ACEA, ACCP Selective CB2 Agonists – HU308, JWH015, JWH133, AM1241 2-AG Synthesis Inhibitors – O3640, O3891, OMDM188, O5596 CB1 Antagonists/Inverse Agonists – SR141716A, AM251 CB1 Neutral Antagonists – AM4113, PIMSR1 CB2 Antagonists/Inverse Agonists – SR144528, AM630 CB1 Receptor Allosteric Modulators – ORG27596, ORG29647

68
Potential Cannabinoid Therapies – Clinical Indications Diseases of Energy Metab. –Appetite Dysregulation –Obesity –Dyslipidemia –Periph Energy Metab Dysreg –Cachexia –Anorexia –Type 2 Diabetes Pain –Somatosensory Pain –Neuropathic Pain Inflammation CNS Disorders –Closed Head Brain Trauma –Neurotoxicity –Stroke –Spinal Cord Injury –Multiple Sclerosis –Parkinson’s Disease –Huntington’s Disease –Tourette’s Syndrome –Tardive Dyskinesia –Dystonia –Amyotrophic Lateral Sclerosis –Alzheimer’s Disease –Epilepsy –Anxiety –Depression –Insomnia –Post-Traumatic Stress Disorder –Schizophrenia

69
Potential Cannabinoid Therapies – Clinical Indications CNS Disorders – con’t –Nausea & Emesis –Drug & Alcohol Addiction Cardiovascular & Respiratory –Hypertension –Hypotension –Circulatory Shock –Myocardial Reperfusion Injury –Atherosclerosis –Cardiopathies –Asthma Eye Disorders –Glaucoma –Retinopathy –Intraocular Pressure Cancer –Cancer Cell Proliferation –Colorectal Cancer GI and Liver Disorders –Inflammatory Bowel Disease –Ulcerative Colitis –Hepatitis –Cirrhosis – Encephalopathy –Cirrhosis – Liver Fibrosis –Cirrhosis – Vasodilatation Musculoskeletal Disorders –Arthritis –Osteoporosis –Post-Fracture Bone Healing Reproductive Disorders

70
Acknowledgments Ken Mackie, MD – Dept of Psychological and Brain Sciences, Indiana University Bloomington Josée Guindon, PhD – Dept of Psychology, Univ of Georgia Andrea G. Hohmann, PhD – Neuroscience and Behavior Program, Univ of Georgia Raphael Mechoulam, PhD – Dept of Medicinal Chemistry, Hebrew University of Jerusalem Roger Pertwee, PhD – School of Medical Sciences, Univ of Aberdeen, Scotland Steven Goldberg, PhD – Behavioral Neuroscience Research Branch, NIDA, NIH Javier Fernández-Ruiz, PhD – Facultad de Medicina, Universi- dad Complutense, Madrid Vincenzo Di Marzo, PhD – Endocannabinoid Research Group, Consiglio Nazionale delle Ricerche, Naples, Italy

71
Neuropsychopharmacology Section, Intramural Research Program National Institute on Drug Abuse, National Institutes of Health

72
Acknowledgment Raphael Mechoulam, PhD Dept of Medicinal Chemistry, Hebrew Univ of Jerusalem

Similar presentations














>")




 The anatomy of the reward pathway defines the road to drug abuse (?) Cellular.>")






