Download presentation
Presentation is loading. Please wait.

1
Dr. Richard Bwana Ombachi Lecturer and Consultant Spine & Orthopaedic surgeon

2
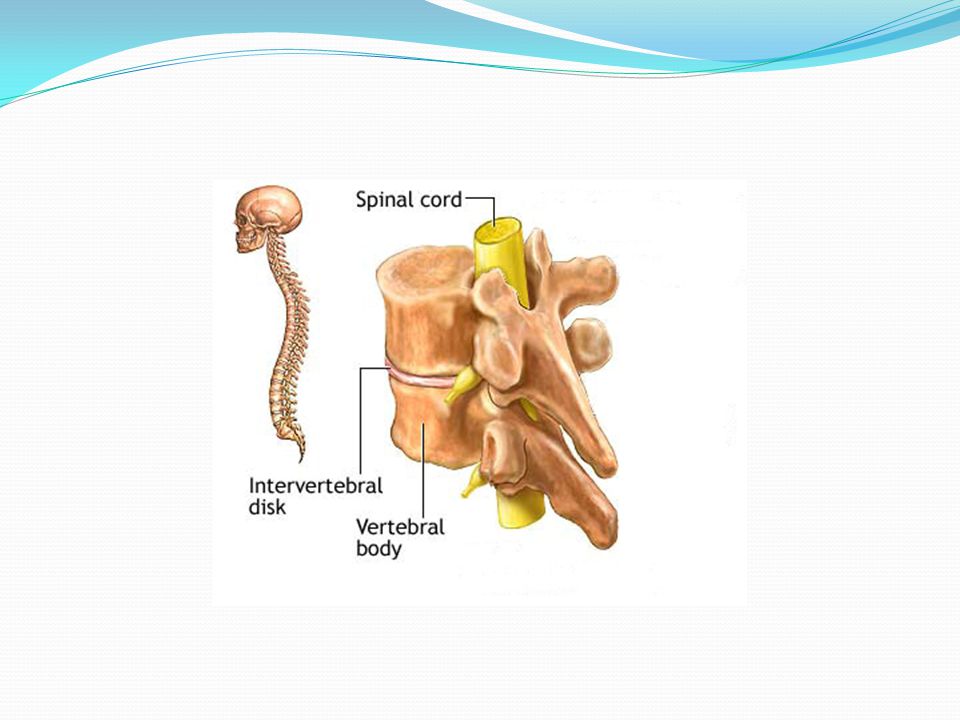
Introduction Spine -Vertebral Column/Nervous Tissue 5% worsen in the hospital Protection is priority –Diagnosis a secondary priority Treat the spine of an alive patient – Identify live threatening conditions Effects of spinal injury Inadequate ventilation Compromised abdominal evaluation Mask compartment syndrome Patient Referral

3
Trauma Vertebral Column Trauma and Nervous Tissue Trauma Somatic Nervous System Spinal Cord tracts Nerve roots / Nerves Autonomic Nervous System sympathetic

5
Spinal Injuries Devastating effect Protection primary priority Management starts at the scene of the accident

6
Spinal Cord Injury Primary Injury- physical injury by mechanical forces Contusion Compression Stretch Laceration – penetrating foreign bodies, missiles, fragments or displaced bone

7
Secondary Injury Additional neural tissue damage from biologic response Changes local blood flow Tissue oedema Metabolite concetration lethal to the neural tissues leading to further injury

8
Statistics Aetiology RTA 45% ( motor cycle accidends ) Falls 20% Sports 15 % Assault 15% Gender ratio M: F 4:1 Neurologic Injury Cervical 40% Thoracolumbar 20%
 Falls 20% Sports 15 % Assault 15% Gender ratio M: F 4:1 Neurologic Injury Cervical 40% Thoracolumbar 20%")
9
PRINCIPLES OF MANAGEMENT Suspect Spinal Injuries and Protect further injury Immobilize the spine Assess the patient (ATLS Protocal) Manage live threatening conditions while caring for spine Image patient to identify the injuries Manage/Reffer injuries as appropriate
 Manage live threatening conditions while caring for spine Image patient to identify the injuries Manage/Reffer injuries as appropriate")
10
Suspect Spinal Injuries History of transient neurological symptoms Neck pain or back pain Multiply Injured patient An inconsolable child Inability to assess pain because of a secondary distracting injury or intoxication Head injury or severe facial or scalp lacerations or neck injuries Trauma +Unconscious : assume spinal injury until proven otherwise Abnormal neurological finding Diaphragmatic breathing Physical signs of spinal trauma (e.g., ecchymosis and abrasions, step deformity, gap deformity. hypotension, hypothermia, and bradycardia- upper thoracic/ cervical injuries neurogenic shock Penile erection and incontinence of the bowel or bladder suggest a significant spinal injury

11
Tale Tell Signs on Examination Patient should be log rolled by at least 4 people for back examination leakage of CSF or blood behind the tympanic membrane- a skull fracture. paraplegia/ quadriplegia Painful spinous process Palpable defects ( gaps or steps) indicate disruption of the supporting ligamentous complex. Scalp wounds, neck injuries, seat belt marks etc. Diaphragmatic Breathing
 indicate disruption of the supporting ligamentous complex. Scalp wounds, neck injuries, seat belt marks etc. Diaphragmatic Breathing.")
12
Immobilize the Spine Protection Priority Neck immobilization firm collar + head strapped to bolsters/ sand bags on either side to the board Immobilize in neutral position don’t correct deformities- ? AS, ? RS children, ? Spondylosis Children - board should have a depression to accomodate big head – avoid flexing neck. Patients should not be kept on the board longer than two hours as pressure sores start to develope two hours on the board (Spine board transporting tool)
.")
16
NEUROLOGICAL EXAMINATION Done to determine level and severity of injury. Sensation to light touch and pain should be documented comparing each spinal level and side Motor examination using MRC grading. Deep tendon reflexes and pathological reflexes also should be checked. Motor and sensory evaluation of the rectum and perirectal area is mandatory (complete/incomplete Injuries)
.")
17
Asia Chart ASIA Chart.pdf

18
Spinal Shock Spinal dysfunction based on physiological rather than structural disruption. Recognized by return of the reflexes caudal to the level of injury usually 24 -48 hours (BCR or the anal wink)
.")
19
Neurogenic Shock Injuries above T6 disrupt the sympathetic nervous system to the heart and the vascular system – Neurogenic shock Sympathetic disruption leads to uncounterted vagal action leading to Bradycardia, Hypotension, Vasodilatation Maintain Mean Preasure above 70mmHg Do not over infuse pt use ionotropic drugs

20
Vertebral Column Examination Done in Secondary Survey Use log rolling technique Detect Bruises/ Lacerations Swellings / Bogginess Step or Gap Deformity Tenderness Remove spine board at this stage if not referring

21
Radiological Imaging Indications No x-rays if No neurological deficit Conscious Cooperative Able to concentrate If no neck or back tenderness Altered sensorium, then X-ray the whole spine Pain or tenderness, no neurological deficit Xray affected areas consider flex-ext

22
X-rays AABBCCDs Adequacy, Alignment, Bony abnormality, Base of Skull, Cartilage, contours, Disc space, Soft tissues - Cross-Table Lateral: 85% sensitive -AP + Lat 92 % sensitivity -excludes most fractures -Swimmer’s for C7-T1 - Open mouth view upper cervical -Obliques not necessary in trauma -CXR / Abd Xrays not adequate for evaluation spine

23
CT SCAN / MRI CT Scan Clearance in patients with questionable or inadequate plain radiographs Assess occipitocervical and cervicothoracic junctions MRI Spinal cord injury – disruptions, oedema, haematomas Intervertebral disc disruption Posterior ligamentous disruption Canal compromise and neural tissue compression

24
Summary of Management High Index of Suscipicion Immobilize the spine to protect spine (Protection Priority) Examine for Spinal and none spinal injuries. Neurological Examination +Vertebral Examination Institute rescuscitation as condition demands giving preference to life threatening conditions While taking care of the spine. Do not over infuse the patient with neurogenic shock- use ionotropic agents as indicated Image the spine to identify and confirm suspected injuries. (Maintain Spine Board untill imaging is complete) Remove Spine Board within two hours to avoid decibitus ulcers Pressure sore management Bladder management Respiratory system management GIT Psychological support Definative stabilization according to the injury Steroids in some centres
 Remove Spine Board within two hours to avoid decibitus ulcers Pressure sore management Bladder management Respiratory system management GIT Psychological support Definative stabilization according to the injury Steroids in some centres.")
Similar presentations