Download presentation
Presentation is loading. Please wait.

2
Summary of results CI recipients (n=320) and their families (n=180) were contacted online, via the SCIP Facebook page and by mail and directed to an online survey Some issues existed with the survey tool used, and these results should be viewed with caution 159 responses were received, representing around one third of all CI recipients and their families with 85% of respondents completing the survey, with two thirds of respondents answering as a recipient and the remaining third answering as a parent or caregiver of a CI recipient The greatest number of responses were received from the largest centres: Christchurch (23%), Wellington (22%) and Otago (16%) and almost a fifth (18%) of those responding had received (or their child had received) an implant in the last year Overall, nearly three quarters of recipients and their families think SCIP meet their needs ‘very well’, with adults being slightly happier with services than families of children with implants – this gap is largest for assessment and ENT and surgical services. Recipients and their families were asked to provide information on the three most important improvements which should be made to SCIP services: 1.Improved communications (37 mentions) 2.Easier accessibility of services for those living outside Christchurch (20 mentions) 3.Reduced costs for recipients (13 mentions) 4.Greater frequency of appointments (12 mentions) 5.Improved facilities (7 mentions) 6.Staff improvements (7 mentions) Background and demographics Overall results …see more …see more While the results show most respondents are happy with services they or their family have received from SCIP, there are improvements which could be made to increase satisfaction among these groups Improvements to future surveys can also be made to increase the value of data collected and ensure respondents don’t suffer survey fatigue Conclusions …see more
 2.Easier accessibility of services for those living outside Christchurch (20 mentions) 3.Reduced costs for recipients (13 mentions) 4.Greater frequency of appointments (12 mentions) 5.Improved facilities (7 mentions) 6.Staff improvements (7 mentions) Background and demographics Overall results …see more …see more While the results show most respondents are happy with services they or their family have received from SCIP, there are improvements which could be made to increase satisfaction among these groups Improvements to future surveys can also be made to increase the value of data collected and ensure respondents don’t suffer survey fatigue Conclusions …see more.")
3
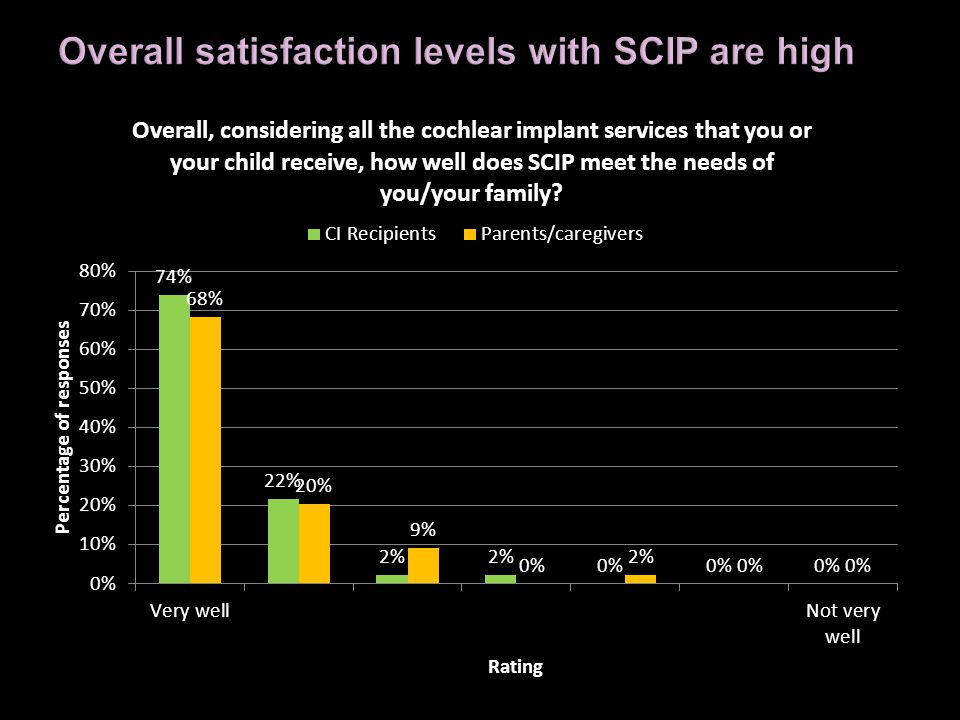
Overall, just over two thirds (68%) of parents/caregivers reported SCIP met their family’s needs ‘very well’, a good result Among service areas, ENT and surgical services scored highest while assessment and audiology services rated lowest Relatively poor scores: Information about the assessment process, habilitation services after 12 months post implant and audiology services received as part of the assessment Relatively good scores: audiology services in the first 12 months after implantation, services from the ENT surgeon and habilitation services received as part of their assessment Parents rated clinic based services most useful but many also noted the high importance of written reports, email communications and home based services Overall, nearly three quarters (74%) of CI recipients reported SCIP met their needs ‘very well’, a good result Among service areas, ENT and surgical services scored highest while assessment rated lowest Relatively poor scores: Rehabilitation services after 12 months post implant, repairs, and referral to SCIP Relatively good scores: ENT and surgical services, including those received as part of their assessment were rated as the best Clinic based services were rated the most useful by CI recipients, with email contact coming second Parents and caregivers CI Recipients …see more Clear segmentation of groups of respondents, showing only relevant questions to each Collection of information on current services, not those received historically Collection of further demographics from respondents Distribution to sample retaining anonymity of individual responses Improved clarity of instructions for respondents Use of scales with descriptions for each response option Improvements for future research …see more
 of parents/caregivers reported SCIP met their family’s needs ‘very well’, a good result Among service areas, ENT and surgical services scored highest while assessment and audiology services rated lowest Relatively poor scores: Information about the assessment process, habilitation services after 12 months post implant and audiology services received as part of the assessment Relatively good scores: audiology services in the first 12 months after implantation, services from the ENT surgeon and habilitation services received as part of their assessment Parents rated clinic based services most useful but many also noted the high importance of written reports, communications and home based services Overall, nearly three quarters (74%) of CI recipients reported SCIP met their needs ‘very well’, a good result Among service areas, ENT and surgical services scored highest while assessment rated lowest Relatively poor scores: Rehabilitation services after 12 months post implant, repairs, and referral to SCIP Relatively good scores: ENT and surgical services, including those received as part of their assessment were rated as the best Clinic based services were rated the most useful by CI recipients, with contact coming second Parents and caregivers CI Recipients …see more Clear segmentation of groups of respondents, showing only relevant questions to each Collection of information on current services, not those received historically Collection of further demographics from respondents Distribution to sample retaining anonymity of individual responses Improved clarity of instructions for respondents Use of scales with descriptions for each response option Improvements for future research …see more")
4
Overall satisfaction Background and demographics CI Recipients Parents and caregivers Improving future surveys Conclusions Click here at the end of each section to return to this index

5
This SCIP designed survey asked people to respond to most questions using the scale below: On this scale, the strongly agree response is at the far left, and is accorded a low score Please be aware of this when reading the results of this survey This also means that lower average ratings for these questions are better than higher average ratings Who answered the questions: It is worth noting that some CI recipients answered questions about habilitation and some parents answered questions about adult services such as rehabilitation In both cases, this may have been legitimate (e.g. a parent answering as such whose child is now receiving services in the adult programme) but the author of this report suspects some of these responses were made in error, as respondents did not carefully read the instructions Samples labeled as “CI Recipients” are most likely to be those receiving adult services, and “Caregivers/Parents” or “families” are most likely to be responding with regard to paediatric services You can read about proposed improvements for future surveys here.here
 but the author of this report suspects some of these responses were made in error, as respondents did not carefully read the instructions Samples labeled as CI Recipients are most likely to be those receiving adult services, and Caregivers/Parents or families are most likely to be responding with regard to paediatric services You can read about proposed improvements for future surveys here.here.")
6
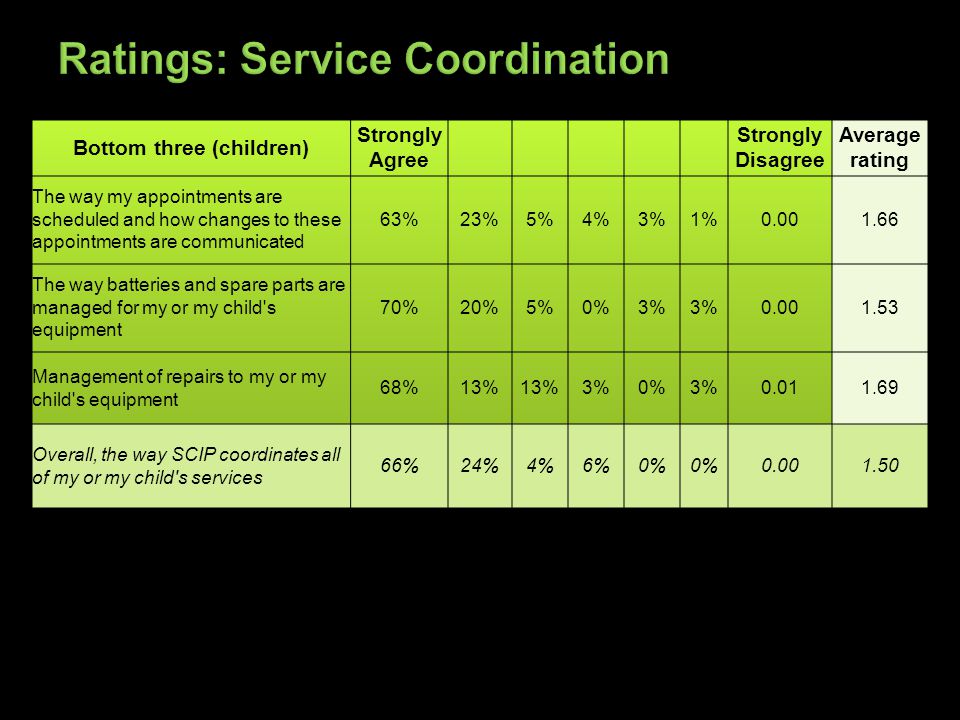
Proportion of respondents selecting each rating Average rating (smaller number the better the average) Overall rating for the service area (e.g. audiology) Tables and comments in green relate to CI recipients (likely to be adults or young adults, while those in yellow are from parents and caregivers
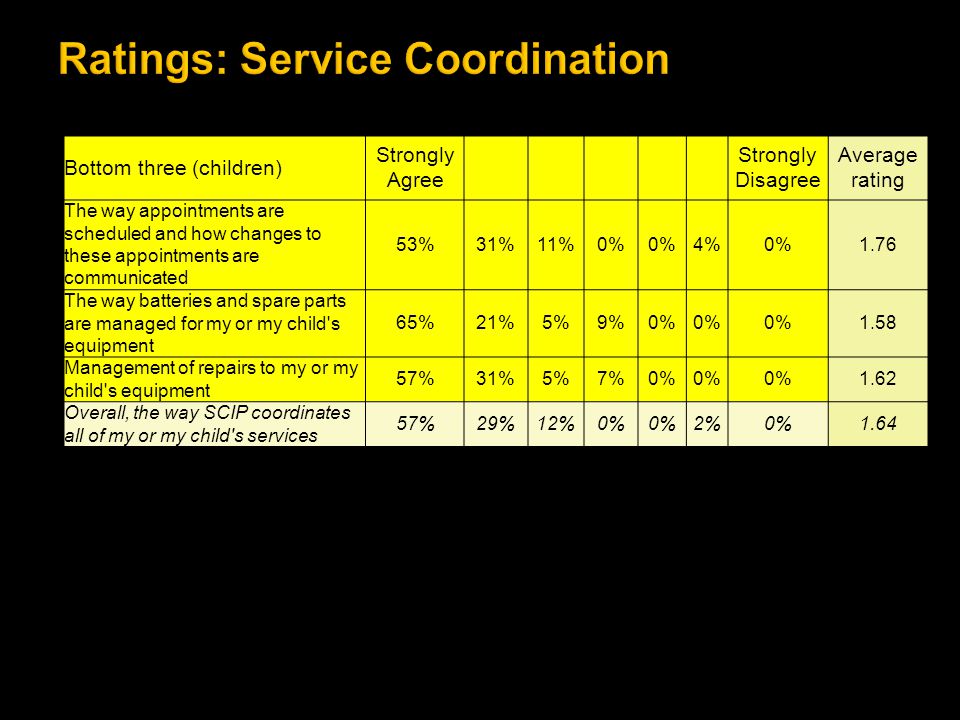
 Tables and comments in green relate to CI recipients (likely to be adults or young adults, while those in yellow are from parents and caregivers.")
8
Generally respondents rated the SCIP highly, with an average rating from recipients and parents of 1.38 on a 0-6 scale where 1 is ‘Very well’ and 6 is ‘not very well’ Recipients rated the programme slightly better than parents and caregivers and approximately three quarters of respondents overall (72%) reported the programme met them or their families needs ‘very well’. The smaller the average, the better for these ratings questions

11
A high number of respondents (n=77/159) gave one or more suggestions on how to improve SCIP services. Of those who did respond, 17 stated that no improvements were needed within the service. The remaining respondents gave one or more suggestions for improvement of services. Most frequently mentioned improvements were, in order: 1.Improved communications (37 mentions) 2.Easier accessibility of services for those living outside Christchurch (20 mentions) 3.Reduced costs for recipients (13 mentions) 4.Greater frequency of appointments (12 mentions) 5.Improved facilities (7 mentions) 6.Staff improvements (7 mentions) 7.More funding for CI (5 mentions) Other issues: Reduced waiting times at clinic before appointments Better battery life for devices Waterproof devices Review infection control procedures Update colour charts Process referrals more quickly More warmth from the organisation SCIP to do all the habilitation work More focus on NZSL Less focus on NZSL
 2.Easier accessibility of services for those living outside Christchurch (20 mentions) 3.Reduced costs for recipients (13 mentions) 4.Greater frequency of appointments (12 mentions) 5.Improved facilities (7 mentions) 6.Staff improvements (7 mentions) 7.More funding for CI (5 mentions) Other issues: Reduced waiting times at clinic before appointments Better battery life for devices Waterproof devices Review infection control procedures Update colour charts Process referrals more quickly More warmth from the organisation SCIP to do all the habilitation work More focus on NZSL Less focus on NZSL.")
12
This topic was mentioned 37 times. All comments related to recipients and their families wanting more information, not less Comments focused mainly on: More frequent communications from the programme to recipients and their families Faster, accurate communications with individual recipients and their families Communication with recipients and potential recipients when they are making key decisions Other comments included: Communication to the general public Better information for those travelling overseas regarding what to do in an emergency

13
General communication with recipients and their families was mentioned 17 times by recipients and their families, of these the two most noted areas were: Appointments – reminders, flexibility re times (n=7) Bring back newsletters/more regular information to keep recipients and those waiting informed (n=7) Since appointments are usually so far in the future, an email or phone call when the appointment is due would be helpful. – Parent or caregiver Other comments related to communication with recipients and their families: More regular progress updates Website – more detail and more content More information in writing Information about personnel changes

14
Communications with individual recipients and their family (n=13) More information for those before surgery e.g. side effects, how long likely to be in hospital (n=3) Quicker responses to emails requested (n=3) More information about new developments and services (n=2) More information on child’s progress (n=1) Communication with those on waiting lists (n=1) More information about the type of implant/processor prior to implantation (n=1) More regular information about upgrade timeframes (n=1) Send appointment information to the correct person (n=1) Communication with those making decisions (n=4) Better information on costs of equipment (n=2) Better information on second implants (n=1) Provide parents with a ‘road map’ explaining what will happen (n=1) “Provide more information about CIs - cost, complications so on, a lot of that is discovered the hard way ourselves, information in writing as it is an overwhelming experience that things can be forgotten.” Adult CI recipient
 Quicker responses to s requested (n=3) More information about new developments and services (n=2) More information on child’s progress (n=1) Communication with those on waiting lists (n=1) More information about the type of implant/processor prior to implantation (n=1) More regular information about upgrade timeframes (n=1) Send appointment information to the correct person (n=1) Communication with those making decisions (n=4) Better information on costs of equipment (n=2) Better information on second implants (n=1) Provide parents with a ‘road map’ explaining what will happen (n=1) Provide more information about CIs - cost, complications so on, a lot of that is discovered the hard way ourselves, information in writing as it is an overwhelming experience that things can be forgotten. Adult CI recipient.")
15
This topic was the most important for 17 of the 20 people mentioning it, indicating it was highly important for those people Of those mentioning this issue, clinics outside Christchurch were commonly requested: Services closer to home (specifically mentioned were Wellington, the Southern North Island, Dunedin) Audiology/repair services closer to where recipients and their families live Access to batteries at more locations More regular tests [would be useful] after mapping - to make sure the implant is working properly before you go back home. – CI recipient
![This topic was the most important for 17 of the 20 people mentioning it, indicating it was highly important for those people Of those mentioning this issue, clinics outside Christchurch were commonly requested: Services closer to home (specifically mentioned were Wellington, the Southern North Island, Dunedin) Audiology/repair services closer to where recipients and their families live Access to batteries at more locations More regular tests [would be useful] after mapping - to make sure the implant is working properly before you go back home.](http://images.slideplayer.com/13/3721261/slides/slide_15.jpg "– CI recipient.")
16
This topic was the most important for 6 of the 13 people mentioning it, with six rating it their second most important issue. Of those mentioning this issue, the following topics were noted: Free batteries or free ear-moulds (n=6) Cheaper or free repairs/parts (n=2) Cheaper or free funding for those who have paid privately for implants/ Cheaper rehabilitation for adults (n=2) More funding for upgrades (n=2) Free second implant (n=1) Many respondents were cognisant of the fact that funding from government is limited, and suggested limited support for those who had limited means “Offer the procedure to all adults, with a sliding scale of personal contribution according to means testing and perceived benefit.”
 Cheaper or free repairs/parts (n=2) Cheaper or free funding for those who have paid privately for implants/ Cheaper rehabilitation for adults (n=2) More funding for upgrades (n=2) Free second implant (n=1) Many respondents were cognisant of the fact that funding from government is limited, and suggested limited support for those who had limited means Offer the procedure to all adults, with a sliding scale of personal contribution according to means testing and perceived benefit. .")
17
This topic was the most important for 6 of the 13 people mentioning it, with five rating it their second most important issue. Of those mentioning this issue, the following topics were noted: More appointments for prelingual children and for those who have had their implant for some time (n=5) More frequent audiological assessments after mapping (n=3) Increased frequency of audiological services/yearly hearing measure (n=2) More appointments (n=1) More appointments in year 2 and 3 (n=1) More rehabilitation (n=1) More regular contact would be beneficial to know that we are on the right track, once the initial visits are over it's a long time between confirmation that 'we're doing the right thing'. – Parent or caregiver Disliked the fact it discontinued after a period of time - now on a "request" basis, when it is better to receive it in an informal setting. – CI recipient
 More frequent audiological assessments after mapping (n=3) Increased frequency of audiological services/yearly hearing measure (n=2) More appointments (n=1) More appointments in year 2 and 3 (n=1) More rehabilitation (n=1) More regular contact would be beneficial to know that we are on the right track, once the initial visits are over it s a long time between confirmation that we re doing the right thing . – Parent or caregiver Disliked the fact it discontinued after a period of time - now on a request basis, when it is better to receive it in an informal setting. – CI recipient.")
18
Of those mentioning this issue, the following improvements were requested: More qualified/experienced staff (n=4) More continuity of care (n=2) Better backup when staff away or on leave (n=1) Have same mapper, so they know your history, that's very important. – CI recipient Haven't had many habilitation appointments due to staff illness, also habilitation appointments need to be more regular as the gap between appointments is too great after the first 3 months. – CI recipient

20
Objectives To establish the views of CI recipients and their families about the SCIP and its services and to understand what areas of the programme could be the focus of future improvement efforts Method The Southern Cochlear Implant Programme has 180 children and 320 adults on its database. Those for whom email addresses were not held received letters alerting them to the survey. The survey was also publicised through the programme’s Facebook page, which has 215 members and is a closed group The survey was conducted online, via a web-link to a SurveyMonkey survey Incentive: Respondents were put in the draw to win a $100 petrol voucher Responses were collected between the 4 th of August 2012 and the 6 th of September 2012. 159 responses were collected, which is likely to represent around 32% of those recipients and their families who were notified of its existence Janet Digby of Levare Limited was contracted to analyse the data collected via SurveyMonkey 84.9% of respondents completed the survey, writing more than 10,000 words in their verbatim comments

21
Two thirds of respondents (67.7%) were answering questions as the recipient of a cochlear implant, while one third (32.3%) answered as the caregiver or parent of a child with a cochlear implant This represents a response rate of approximately 28% of families and 33% of CI recipients
 were answering questions as the recipient of a cochlear implant, while one third (32.3%) answered as the caregiver or parent of a child with a cochlear implant This represents a response rate of approximately 28% of families and 33% of CI recipients")
24
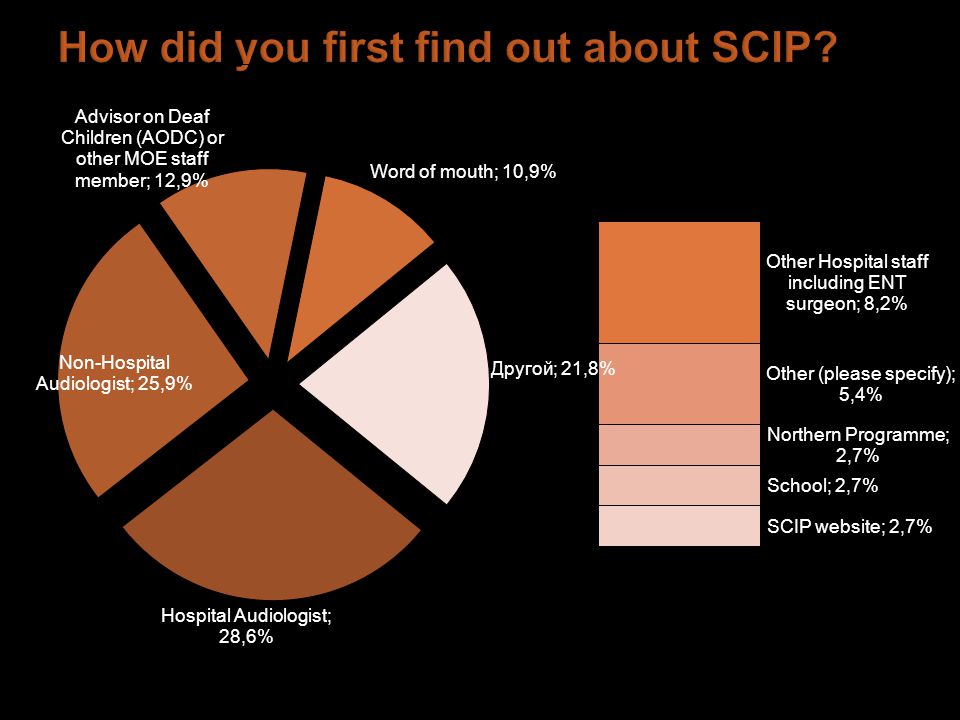
85% listed one agency or individual as the source of referral, while 13% listed two, and 2% listed three. Further clarity on this question would be useful for respondents for any subsequent surveys.

26
CI recipients were asked to rate individual service areas and then to provide an overall rating for that area e.g. assessment services The table above shows these top level ratings for service areas CI recipients rated ENT and surgical services received the highest service top level ratings, while assessment services and service coordination received the lowest ratings The final overall rating (at the bottom of the table) shows how CI recipients rated the programme overall. This rating was 1.33, indicating that there were likely to be other areas which contributed to satisfaction which were not listed within the survey (as only one area rating was higher than this one)
 shows how CI recipients rated the programme overall. This rating was 1.33, indicating that there were likely to be other areas which contributed to satisfaction which were not listed within the survey (as only one area rating was higher than this one).")
27
The three areas rated lowest by CI recipients are found in the table below:

28
The three areas rated highest by CI recipients are found in the table below The following slides contains details of specific ratings split by topic

30
26 comments were received related to the fact that staff were happy, knowledgeable, caring, good communicators, had good listening skills or that there were no improvements to services they could think of Other comments included: Wait too long for audiological assessment (n=3) More careful consideration of side for implant (n=3) I had to wait almost 3 years for the initial assessment. I wish I was told that I could have gone earlier & paid for it instead of waiting too long – CI recipient And there were again a number of comments about the need for more information delivered in an appropriate way: Need more information on how recipients may feel post surgery (n=3) Need more information re assessment process and how it works at the beginning (n=3) Need more information on waiting time for implant (n=2) More general information through newsletters and other communications (n=2) Wasn’t told of private option for assessment (n=2) Couldn’t understand or hear important information provided as voices soft or too many voices in meeting to inform client (n=1) Wasn’t told about processors needing replacement (n=1) Need more information on criteria for implant (n=1) Bay audiologists not experienced (n=1) More information useful to inform brand choice (n=1) As far as I can recall the assessment process wasn't explained enough prior to appt. What would happen and what sort of questions would be asked etc. I had planned my husband to leave for the duration of the appt. as I assumed it was just going to be more hearing tests etc. In fact we were both very much needed there together to get the overall big picture together. It was a successful assessment though but prior info would have been better. The meeting before going ahead with the operation..........was hard to follow...lots of people and that usually means people talking from different directions...although things were written on a white board and conversation afterwards was with I think too many people........but maybe that is not always done with so many
 Need more information re assessment process and how it works at the beginning (n=3) Need more information on waiting time for implant (n=2) More general information through newsletters and other communications (n=2) Wasn’t told of private option for assessment (n=2) Couldn’t understand or hear important information provided as voices soft or too many voices in meeting to inform client (n=1) Wasn’t told about processors needing replacement (n=1) Need more information on criteria for implant (n=1) Bay audiologists not experienced (n=1) More information useful to inform brand choice (n=1) As far as I can recall the assessment process wasn t explained enough prior to appt. What would happen and what sort of questions would be asked etc. I had planned my husband to leave for the duration of the appt. as I assumed it was just going to be more hearing tests etc. In fact we were both very much needed there together to get the overall big picture together. It was a successful assessment though but prior info would have been better. The meeting before going ahead with the operation was hard to follow...lots of people and that usually means people talking from different directions...although things were written on a white board and conversation afterwards was with I think too many people but maybe that is not always done with so many.")
31
One respondent mentioned the lack of an NZSL focus for children and adults: The SCIP programme does not provide the natural inclusion of NZ Sign Language as part of the assessment and habilitation process. Since everybody with an implant is still deaf without it on, and a number of children have a far better success rate of language acquisition using NZSL in conjunction with speech training, this is a severe shortcoming. It shows the hearing prejudice and lack of understanding of how NZSL may help children make better use of their implant, and reduce the communication barriers and frustration they experience, especially while their brains learn to recognise sound. It is not a case of either or, NZSL and speech can be used together. A number of comments were also received relating to non-SCIP services: Audiologist was reluctant or had never referred to SCIP (n=3) DHB travel reimbursement process difficult (n=1) ENT surgeon in local area had a lack of knowledge re CI (n=1) Having to pay for travel to Christchurch (n=1) Getting to Christchurch for assessment was pure chance. My audiologist said a CI was not for me until I had exhausted all conventional hearing aid possibilities. The hospital audiologist only suggested assessment for a CI after I vented a bit-'I've lost my job, lost some friends, can't use phones, watch TV etc. etc.'. I had little idea what a CI was (I though it was a 'Cochlear Transplant') until I arrived for assessment, and knew zip about the assessment process. From the time I arrived in Christchurch things were just brilliant. It was clear, well explained, everyone was patient and sympathetic.
 DHB travel reimbursement process difficult (n=1) ENT surgeon in local area had a lack of knowledge re CI (n=1) Having to pay for travel to Christchurch (n=1) Getting to Christchurch for assessment was pure chance. My audiologist said a CI was not for me until I had exhausted all conventional hearing aid possibilities. The hospital audiologist only suggested assessment for a CI after I vented a bit- I ve lost my job, lost some friends, can t use phones, watch TV etc. etc. . I had little idea what a CI was (I though it was a Cochlear Transplant ) until I arrived for assessment, and knew zip about the assessment process. From the time I arrived in Christchurch things were just brilliant. It was clear, well explained, everyone was patient and sympathetic..")
32
Most CI recipients providing written comments on hospital and ENT services reported being happy or very happy with the services they received from their ENT surgeon and the hospital Nine CI recipients reported that they did not receive their hospital and ENT services from either SCIP or from St George’s hospital Those recipients with suggestions for improvements noted issues with their expectations post surgery, with support, pain relief and surgeon contact ▪They didn’t realise how affected they would be after the surgery and how much help they would need ▪They were released too soon without support ▪They had bleeding from the head post surgery and neither they nor their doctor were sure if this was normal ▪Problems with pain relief (either in hospital or after discharge) ▪It was hard for them to contact their surgeon
 ▪It was hard for them to contact their surgeon")
33
17 positive comments were recorded by CI recipients including that they were satisfied with services, very satisfied and or happy with staff who were helpful, responsive to questions and willing to discuss concerns and ideas As with habilitation for children, a significant number of comments were received about a lack of rehabilitation services ▪CI recipients need more rehabilitation sessions (those who are newly implanted but particularly those who had their implant some time ago) ▪Rehabilitation appointments were only on request or that recipients don’t receive much at all, including one recipient who doesn’t recall receiving rehabilitation services ▪That staff illness can mean fewer appointments for recipients ▪Need more measures of access to speech sounds over time ▪The need for more follow up initially after mapping
 ▪Rehabilitation appointments were only on request or that recipients don’t receive much at all, including one recipient who doesn’t recall receiving rehabilitation services ▪That staff illness can mean fewer appointments for recipients ▪Need more measures of access to speech sounds over time ▪The need for more follow up initially after mapping")
34
Other suggestions, each mentioned once, included: Dislike of the Judy Bailey exercises* SCIP should lobby for more funding Long waits at clinic prior to appointment Need more opportunity to discuss concerns with staff Need more soundproofing in clinic That it would be good to receive more information about new technology One recipient mentioned the importance of processor upgrades, while another mentioned that processors need to be more robust. Love the programme upgrades, the hearing quality just keeps on getting better and the process smoother and easier. Appreciate the chance to discuss concerns ideas & theories about rehabilitation and using the processor to best advantage especially for music. Wish the processors could be a bit more robust in the areas getting the most wear - specifically the rubber hinge cover at the back corner. - CI Recipient *the “Judy Bailey” exercises are a series of speech perception measures using Judy Bailey as the speaker

36
Fifteen comments made were positive regarding audiology services, while the remaining 9 suggested improvements: Positive comments about staff (general and specific) (n=9) Good services/no need for improvement/satisfied (n=6) Other positive comments were: Always ready to help (n=1) Staff take time to provide appropriate service (n=1) Fast email responses to questions (n=1) Patient staff (n=1) Good prices on batteries appreciated (n=1) No restriction on number of visits good (n=1) One respondent made special mention of a staff member going the extra mile on the day of the earthquake, and how much they appreciated this: “[Staff member] arranged my flights home on the day of the earthquake seeing how traumatised I was. I thought this was more than he needed to do and was so much appreciated.”
![Fifteen comments made were positive regarding audiology services, while the remaining 9 suggested improvements: Positive comments about staff (general and specific) (n=9) Good services/no need for improvement/satisfied (n=6) Other positive comments were: Always ready to help (n=1) Staff take time to provide appropriate service (n=1) Fast responses to questions (n=1) Patient staff (n=1) Good prices on batteries appreciated (n=1) No restriction on number of visits good (n=1) One respondent made special mention of a staff member going the extra mile on the day of the earthquake, and how much they appreciated this: [Staff member] arranged my flights home on the day of the earthquake seeing how traumatised I was.](http://images.slideplayer.com/13/3721261/slides/slide_36.jpg "I thought this was more than he needed to do and was so much appreciated. .")
37
The importance of mapping and speed in refining the map The most common suggestion or issue raised related to the importance of having a good map and getting feedback after use and quick changes made if needed (n=5): - Having a check on the map, even by phone two weeks after a change would be useful - Further training for audiologists on mapping and that audiologists need to listen more to clients in mapping appointments (n=3) - Two days in Christchurch would allow changes on the second day if necessary (n=1) - Another mentioned the potential value in having the mapping completed online (n=1) The other issues mentioned were that: Services need to be closer to home/closer to Wellington/Disruptive to travel That audiological services needed to be more frequent Comfy chair in audiology room would be helpful More soundproofing for audiology room
: - Having a check on the map, even by phone two weeks after a change would be useful - Further training for audiologists on mapping and that audiologists need to listen more to clients in mapping appointments (n=3) - Two days in Christchurch would allow changes on the second day if necessary (n=1) - Another mentioned the potential value in having the mapping completed online (n=1) The other issues mentioned were that: Services need to be closer to home/closer to Wellington/Disruptive to travel That audiological services needed to be more frequent Comfy chair in audiology room would be helpful More soundproofing for audiology room")
39
The most mentioned suggestions relating to service coordination topics were on the costs of repairs, ear moulds, batteries, replacement parts and controllers (n=7) The other commonly mentioned area was appointments: The need for earlier notice That coordination of rehab evenings and audiology appointments would be useful That they valued the SCIP for its flexibility in giving appointments to recipients Other comments included: The importance of ensuring young adults are aware of what costs they will incur once they reach 21 Due to the extensive use of telephone for work requirements my controller button wears out each 12 months, I now have to buy a new controller each 12 months $1k. [I] Wish I did not have to pay for my CI batteries. I am a full time student, 19 yrs. I think it is strange that my hearing aid batteries are funded and not my CI where I only use one battery for my hearing aid lasting 4 day and my CI takes 3 batteries lasting about 3 days – CI Recipient

40
While parents and caregivers reported most services were useful for their family, responses from CI recipients were more mixed (see graph above) with only clinic services, email contact and written reports receiving more than 50% ‘very useful’ ratings Clinic services were again rated most highly, along with email contact and written reports. Interestingly, Nelson and Marlborough and Otago respondents did not value Skype or telephone services despite their distance from Christchurch Email contact was valued less by those in Canterbury and Christchurch and surrounding areas

42
Families of CI recipients were asked to rate individual service areas and then to provide an overall rating for that area e.g. assessment services The table above shows these top level ratings for service areas CI recipients rated audiology services the highest service top level ratings, while assessment services received the lowest overall ratings The final overall rating (at the bottom of the table) shows how CI recipients rated the programme overall. This rating was 1.48, indicating that there were likely to be other areas which contributed to satisfaction which were not listed within the survey (as only one area rating was lower than this one)
 shows how CI recipients rated the programme overall. This rating was 1.48, indicating that there were likely to be other areas which contributed to satisfaction which were not listed within the survey (as only one area rating was lower than this one).")
43
The three specific areas rated lowest by families are included in the table below:

44
The three specific areas rated highest by families are included in the table below The following slides contains details of specific ratings split by topic

45
Question Strongly Agree Strongly Disagree Average rating The way I or my child was referred for a cochlear implant 57%28%4%6%4%0% 1.72 How I was informed about the assessment process 45%34%9% 4%0% 1.94 Audiology services I or my child received as part of my assessment 62%17%11%9%0% 2%1.77 Habilitation/Rehabilitation services I or my child received as part of my assessment 64%23%4%9%0% 1.57 ENT/surgical services I or my child received as part of my assessment 64%19%9% 0% 1.62 Overall, with all of the Audiology, ENT, and Habilitation/Rehabilitation services I received as part of my or my child's assessment for a cochlear implant 58%22%13%4%2%0% 1.71

46
24 families responded to the question asking them to record what they liked or disliked about the assessment process 10 comments mentioned the valued support of staff, their expertise and the fact that they had no problems with the assessment part of the service. Other positive comments included the value in meeting another family, the benefits of such open communication and the fact that one family were very appreciative that their child was able to stay on the paediatric programme right through the initial habilitation even though she was technically now an adult Further information was also requested on the assessment process and what to expect (n=3) Other issues raised included: That one family felt pressured to get a CI, or as though there was no conscious choice for them (n=2) Stressful waiting for approval (n=1) Testing not age appropriate in tone (n=1) Need to be seen faster by SCIP once referred (n=1) That information about what was needed for assessment could be more proactive from SCIP – they had to enquire about the need for an MRI Lack of NZSL focus for children (from a CI Recipient answering questions about the paediatric programme) The testing for the rehabilitation was too babyish for me, found it off putting, kind of insulting for me. I think that the testing needs to be adjusted to the age of the client. I was 16 yrs. - CI Recipient
 Other issues raised included: That one family felt pressured to get a CI, or as though there was no conscious choice for them (n=2) Stressful waiting for approval (n=1) Testing not age appropriate in tone (n=1) Need to be seen faster by SCIP once referred (n=1) That information about what was needed for assessment could be more proactive from SCIP – they had to enquire about the need for an MRI Lack of NZSL focus for children (from a CI Recipient answering questions about the paediatric programme) The testing for the rehabilitation was too babyish for me, found it off putting, kind of insulting for me. I think that the testing needs to be adjusted to the age of the client. I was 16 yrs. - CI Recipient.")
47
A number of comments were also received relating to non-SCIP services: Poor experience with hospital audiologist (n=2) Poor information from AODC (1) Poor knowledge of doctor re CI (n=1) Late diagnosis of child/earlier referral needed (2) Actually we find SCIP to be fantastic. Our issue was with our Hospital Audiologist who clearly had very little experience in advising a family of a profound hearing loss. In fact we were give no information at all by her, nor would she clearly state that our daughter had a profound hearing loss. Her words were 'in my opinion I feel that her daughter has a hearing impairment'. It wasn't until I probed that she then said 'well she has no brain response to any sound what so ever'. We were also not given information on what a Deaf Advisor does. When I made the comment to her that 'I guess we will need to think about learning sign language', her response was 'why would you want to do that? You have options' but then did not go into what those options were. Not a great way to enter the world of hearing loss...

48
Questions Strongly Agree Strongly Disagree Average rating Services I received from my surgeon 80%7%0%5% 2%0%1.54 Services I received at St George's Hospital 68%16%5% 0% 5%1.74 Overall, services I received from my surgeon and St George's Hospital during my cochlear implant surgery 60%25%10%3%0%3%0%1.68 Most families who provided written comments on hospital and ENT services reported being happy or very happy with the services they received from their surgeon and the hospital Nine families reported that they did not receive their hospital and ENT services from either SCIP or from St George’s hospital Those families with suggestions for improvement s requested: ▪More toys and entertainment for children while recovering ▪Hospital staff with more experience with very young children ▪A single room – as this would have been good during what was an emotional time ▪More variety with food available for children and parents ▪A confirmed time to meet with the surgeon after the surgery ▪More training on stitching and scar minimisation for surgeons ▪Review of infection control processes, including a review of antibiotic usage

49
Strongly Agree Strongly Disagree Average rating Habilitation services my child receives (or received) from my therapist during the first 12 months after implantation 60%25%10%3%0%3%0%1.65 I am satisfied with the Habilitation services my child receives from my therapist beyond the first 12 months of implantation 55%21%12%9%0% 3%1.91 Overall I am satisfied with all of the Habilitation services my child receives from their therapist 67%19%9%2%0% 2%1.53 A number of families who provided written comments on habilitation services valued the friendly and helpful staff and were happy or satisfied with services ▪Good to have a therapist who uses sign ▪Short reports useful ▪Staff are easy to contact However, more families made suggestions regarding improvements which could be made to these services.
 from my therapist during the first 12 months after implantation 60%25%10%3%0%3%0%1.65 I am satisfied with the Habilitation services my child receives from my therapist beyond the first 12 months of implantation 55%21%12%9%0% 3%1.91 Overall I am satisfied with all of the Habilitation services my child receives from their therapist 67%19%9%2%0% 2%1.53 A number of families who provided written comments on habilitation services valued the friendly and helpful staff and were happy or satisfied with services ▪Good to have a therapist who uses sign ▪Short reports useful ▪Staff are easy to contact However, more families made suggestions regarding improvements which could be made to these services.")
50
While families mentioned seven times that they were happy with services, a number of issues were also raised. The most commonly mentioned issue was that they wanted to see more more frequent habilitation services – this was mentioned eleven times, almost half the items mentioned related to this issue Other issues included: (mentioned once each) That families shouldn’t have to suggest alternative service options, these should be offered to them The importance of more information for families as the child ages More clarity around the roles of AODCs and SCIP staff Needing more structure and direction for the family’s work with their child The need for explicit goals within the habilitation programme Children can be tired following travel on visits to Christchurch, limiting the value of visits Comments on other providers The need for AODCs to focus less on NZSL (n=1) The value of working with ITODs on the ground (n=1) “I think there was some confusion between us as to what the deaf advisor would be doing as compared to the habilitation service base out of SCIP. We have a different AODC now and this one seems to be better in terms of working with us. (The first one was LOVELY, but very focussed on sign language which is what we were told NOT to do in the first year or two, by SCIP)”
 That families shouldn’t have to suggest alternative service options, these should be offered to them The importance of more information for families as the child ages More clarity around the roles of AODCs and SCIP staff Needing more structure and direction for the family’s work with their child The need for explicit goals within the habilitation programme Children can be tired following travel on visits to Christchurch, limiting the value of visits Comments on other providers The need for AODCs to focus less on NZSL (n=1) The value of working with ITODs on the ground (n=1) I think there was some confusion between us as to what the deaf advisor would be doing as compared to the habilitation service base out of SCIP. We have a different AODC now and this one seems to be better in terms of working with us. (The first one was LOVELY, but very focussed on sign language which is what we were told NOT to do in the first year or two, by SCIP) .")
51
The most commonly mentioned suggestion was increasing the intensity of habilitation services, such as providing more appointments for children – these comments related to those who were newly implanted and those who had been in the service for longer (see next slide for further information) “The sessions so far at SCIP are very useful but I would like more direction as to what we are meant to do at home or some ideas written down. It would be good if there was a more structured programme that is followed for the habilitation side of things. I am not sure what we are meant to be expecting from our child or what goals should be reached at each stage post switch-on if any. I feel the habilitation post switch on needs to be more intensive and structured. Would be great if there were more AV trained therapists available through SCIP to provide the habilitation.” Parent or caregiver Other suggestions included: ▪More therapists needed ▪More information about what other services are available ▪Programme needs to be more proactive in offering new service options to families ▪Children are not always at their best when they have to travel to SCIP, so detailed follow up important Some suggestions did not relate to SCIP services: ▪Confusion regarding the roles of SCIP and AODC ▪Conflicting advice from SCIP and AODC, as AODC too focused on sign language ▪More contact from AODC needed

52
Strongly Agree Strongly Disagree Average rating Audiology services I or my child received from my Audiologist in the first 12 months after getting an implant 68%25%3%5%0% 1.45 Audiology services I or my child receive from my Audiologist having had my implant for more than 12 months 56%29%3%12%0% 1.71 Overall, Audiology services I or my child receives from SCIP 65%30%5%0% 1.40

53
Of comments provided, 11 suggestions related to improvements for paediatric audiology services, while nine were positive and related to staff and their responsiveness, services overall and the move to Merivale*. The need for local audiology services in Wellington or Palmerston North was the most frequently mentioned suggestion (n=5), other comments included More frequent (twice yearly) audiology services (n=2) The need for further explanation of what is happening in appointments (n=2) Request for reports after audiology appointments (n=1) “[It] would be good to have a little more explanation (for us parents as lay people) as to what is going on during the audiology appointments.” *the move from VADEC to Merivale following the Feb 2011 earthquakes
, other comments included More frequent (twice yearly) audiology services (n=2) The need for further explanation of what is happening in appointments (n=2) Request for reports after audiology appointments (n=1) [It] would be good to have a little more explanation (for us parents as lay people) as to what is going on during the audiology appointments. *the move from VADEC to Merivale following the Feb 2011 earthquakes.")
55
11 comments mentioned positive qualities of the staff at SCIP, including that they were accommodating, approachable, professional and friendly and that SCIP provided a good service. Other positive comments included: Good management of spare and loan parts, including to a family overseas (n=5) Replacement parts received quickly (n=2) New location good (n=1) Urgent needs accommodated (n=1) Issues included: Longer lead time for appointments would be good to allow plans and arrangements (n=3) Need for more flexibility to book airfares for other family members in advance (when they are on sale) (n=2) Problems with travel plans and communication re this/need to request changes (n=2) Letters not always accurate and reports sent to wrong RTD (n=2) Cost of batteries (for children when they move to the adult programme), slow responses to emails, lack of flexibility and short notice for appointments, slowness of repairs were also mentioned Generally good service - but would like more understanding for families coming from out of town and trying to co- ordinate other family members - whether they be wanting to travel down too or making arrangements for their care while we are away. There needs to be flexibility on SCIP's part to allow us to book (cheap) airfares for other family members in advance when they are on sale. – Parent/caregiver The only frustration is how long we have to wait for an appointment if we have to reschedule. Our 12 month appointment didn't happen until 15 months. With that said, in an urgent situation recently we were fitted in very quickly and that was greatly appreciated.. – Parent/caregiver
 Replacement parts received quickly (n=2) New location good (n=1) Urgent needs accommodated (n=1) Issues included: Longer lead time for appointments would be good to allow plans and arrangements (n=3) Need for more flexibility to book airfares for other family members in advance (when they are on sale) (n=2) Problems with travel plans and communication re this/need to request changes (n=2) Letters not always accurate and reports sent to wrong RTD (n=2) Cost of batteries (for children when they move to the adult programme), slow responses to s, lack of flexibility and short notice for appointments, slowness of repairs were also mentioned Generally good service - but would like more understanding for families coming from out of town and trying to co- ordinate other family members - whether they be wanting to travel down too or making arrangements for their care while we are away. There needs to be flexibility on SCIP s part to allow us to book (cheap) airfares for other family members in advance when they are on sale. – Parent/caregiver The only frustration is how long we have to wait for an appointment if we have to reschedule. Our 12 month appointment didn t happen until 15 months. With that said, in an urgent situation recently we were fitted in very quickly and that was greatly appreciated.. – Parent/caregiver.")
56
Most respondents found most services to be useful for their family, although responses were more mixed for internet and telephone services Clinic services were rated most highly by those living in all areas, along with written reports, while Skype and phone services were rated ‘very useful’ by respondents in some areas (e.g. Nelson Marlborough and Taranaki) and ‘Not useful’ by others (e.g. Southland, Otago). Skype and phone services were understandably rated less useful for those families living in Christchurch Email contact was rated ‘very useful’ by most respondents.
 and ‘Not useful’ by others (e.g. Southland, Otago). Skype and phone services were understandably rated less useful for those families living in Christchurch contact was rated ‘very useful’ by most respondents..")
58
A number of issues were identified which were outside SCIP control, these include: Poor knowledge of CI’s among hospital audiologists, ENT specialists and GPs Poor hospital audiology services, particularly with regard to young children Poor communication of diagnoses from audiologists Late identification of hearing losses in DHBs Inadequate services from AODCs and RTDs Conflicting advice from AODCs re sign language cf SCIP Inadequate information about CIs from AODCs Dislike of DHB travel reimbursement process Actually we find SCIP to be fantastic. Our issue was with our Hospital Audiologist who clearly had very little experience in advising a family of a profound hearing loss. In fact we were give no information at all by her, nor would she clearly state that our daughter had a profound hearing loss. Her words were 'in my opinion I feel that her daughter has a hearing impairment'. It wasn't until I probed that she then said 'well she has no brain response to any sound what so ever'. We were also not given information on what Deaf Advisor does. When I made the comment to her that 'I guess we will need to think about learning sign language', her response was 'why would you want to do that? You have options' but then did not go into what those options were. Not a great way to enter the world of hearing loss...

62
Framing: “We are interested in you or your child’s experiences of SCIP services in the last year…”(The 2012 survey provides good historic information about services received, future surveys can now focus on current services.) The rating scale used should have descriptions at each point e.g. Very well, well, neither well nor poorly, poorly, very poorly. Very poorly in this case being the worst rating, as opposed to the 2012 rating of ‘not very well’. Type of respondent question should be made more specific (is the aim to split adult and paediatric programme?) Part One: Are you completing this survey as 1) a person who has received services from the SCIP or 2) for a child or young person in your family who has received services from SCIP? Part Two: Have you or your child received services from 1) SCIP’s Paediatric Programme, or 2) SCIP’s Adult programme? or 3) Both SCIP’s Paediatric Programme and SCIP’s Adult programme? (These would be directed to different parts of the survey Change referral question to make this more specific – it would seem that people don’t understand what this means How did you first find out about SCIP – should be answer one only, same with referral question Add a catch all question at the end of the questionnaire to allow respondents to express anything which they haven’t previously
 Part One: Are you completing this survey as 1) a person who has received services from the SCIP or 2) for a child or young person in your family who has received services from SCIP. Part Two: Have you or your child received services from 1) SCIP’s Paediatric Programme, or 2) SCIP’s Adult programme. or 3) Both SCIP’s Paediatric Programme and SCIP’s Adult programme. (These would be directed to different parts of the survey Change referral question to make this more specific – it would seem that people don’t understand what this means How did you first find out about SCIP – should be answer one only, same with referral question Add a catch all question at the end of the questionnaire to allow respondents to express anything which they haven’t previously.")
64
The Southern Cochlear Implant Programme is doing well in the eyes of most CI recipients and their families Families seem to be slightly less satisfied than adults Improvements can be made in a number of areas, particularly with regard to communications and easier access to services for those living outside Christchurch It may also be useful to ensure SCIP clients and their families are clear about which services are provided by SCIP and which services are outside SCIP control and to educate medical professionals about CI Improvements can also be made to ensure future surveys are easier to complete, reduce the risk of survey fatigue among respondents and provide evermore useful information on which to base future improvements to the services offered SCIP should focus on telling recipients and their families about what the programme has learnt from the feedback received, and what they intend to do as a result To maximise benefit further, SCIP should tell recipients and their families about changes while and after these have been made

Similar presentations














 Information Report>")



>")











 is intended to help students with disabilities interact with the same content.>")
