Download presentation
Presentation is loading. Please wait.

1
Hasan Abdallah, MD Children’s Heart Institute
Dysautonomias Hasan Abdallah, MD Children’s Heart Institute

2
Dysautonomias Definition: altered autonomic function

3
History Galen(2nd Century): Nerves are hollow tubes distributing “animal spirits” to body parts enabling concerted action, or “sympathy” of the organs. Eustachius (1552): anatomy of the sympathetic nerves and the adrenal glands Abel and Takamine(1895): identified epinephrine as the active principle of the adrenal gland. Langley ( 1898) introduced the term autonomic nervous system to denote the portion of the nervous system largely responsible for involuntary, unconscious functions of internal organs. Cannon(1920): the sympathetic nerves and adrenal medulla is a functional unit—the “sympathico-adrenal” system.
: Nerves are hollow tubes distributing animal spirits to body parts enabling concerted action, or sympathy of the organs. Eustachius (1552): anatomy of the sympathetic nerves and the adrenal glands. Abel and Takamine(1895): identified epinephrine as the active principle of the adrenal gland. Langley ( 1898) introduced the term autonomic nervous system to denote the portion of the nervous system largely responsible for involuntary, unconscious functions of internal organs. Cannon(1920): the sympathetic nerves and adrenal medulla is a functional unit—the sympathico-adrenal system.")
4
Scope of the Problem Up to 1% of teenagers are debilitated with chronic fatigue. Autonomic dysfunction is identified in around 50% patients with CFS

5
Autonomic Nervous System ( ANS) ANATOMY AND PHYSIOLOGY
Sympathetic (thoracolumbar) Parasympathetic (craniosacral) Enteric The ANS is largely involuntary motor/ effector system. The CAN (Central Autonomic Network) Maintains integral relationships with visceral sensory neurons via afferent input from the vagus nerve and relays transmission through the nucleus tractus solitarius to the hypothalamus, amygdala, and forebrain. Autonomic Outflow Discharge: Occur independently, partially regulated and integrated by the central autonomic network (CAN)
 Parasympathetic (craniosacral) Enteric. The ANS is largely involuntary motor/ effector system. The CAN (Central Autonomic Network) Maintains integral relationships with visceral sensory neurons via afferent. input from the vagus nerve and relays transmission. through the nucleus tractus solitarius to the hypothalamus, amygdala, and forebrain. Autonomic Outflow Discharge: Occur independently, partially regulated and integrated by the central autonomic network (CAN)")
7
ANS Complex System: Pervasive and integrates multiple secondary functions so that symptoms can be widespread and confounding. Autonomic Dysfunction is often associated sensory perturbations, because the development of the Autnomic and sensory systems are closely linked

8
Embryologic Development
Development of the ANS is intimately related to the development of the sensory nervous system; both have their embryonic origins in the multipotential neural crest cells. These cells migrate and eventually evolve into sensory and autonomic ganglia as well as the adrenal chromaffin cells. Their differentiation and commitment to function in the mature nervous system is incumbent on exposure to growth factors released by structures along the migratory route and then within the target tissue.

10
Fuctional Oraganization of the Autonomic Nervous System
Inhibitory input from mechanoreceptors in the heart and aortic and carotid baroreceptors travels via afferent vagal fibers to the nucleus tractus solitarius (NTS). Sympathetic outflow is transmitted by efferent nerve fibers to the heart, blood vesselsa nd adrenal gland via the spinal cord. Cardiac parasympathetic tone originating from the vagal nuclei is modulated by the NTS in an integrated and reciprocal fashion, The resulting autonomic tone is determined by the balance between sympathetic and parasympathetic outf1ow
. Sympathetic outflow is transmitted by efferent nerve fibers to the heart, blood vesselsa nd adrenal gland via the spinal cord. Cardiac parasympathetic tone originating from the vagal nuclei is modulated by the NTS in an integrated and reciprocal fashion, The resulting autonomic tone is determined by the balance between sympathetic and parasympathetic outf1ow")
11
orthostatic intolerance
Humans absolutely require a functionally intact sympathetic nervous system to tolerate the “nonemergency” behavior of simply standing up. This explains why orthostatic intolerance constitutes a cardinal clinical manifestation of sympathetic neurocirculatory failure

12
Autonomic Dysfunction
Determine: Clinical Features Extent Severity Duration- Acute, Subacute, Chronic) Frequency- the symptoms occur (Daily, weekly, etc…) Diurnal variation Functional impact Secondary causes (e.g. Anemia, Dehydration, Deconditioning or Thyroid disorder) Possible underlying pathogenesis
 Frequency- the symptoms occur (Daily, weekly, etc…) Diurnal variation Functional impact Secondary causes (e.g. Anemia, Dehydration, Deconditioning or Thyroid disorder) Possible underlying pathogenesis")
13
RAR = rapidly adapting receptor;
SAR = slowly adapting receptor.

14
Orthostatic Intolerance
Symptoms occurring upon changing from the supine to the standing positions. May include: Dizziness, Lightheadedness, Blurred or Tunnel Vision Headache, Nausea Throbbing Headaches Diaphoresis Syncope

16
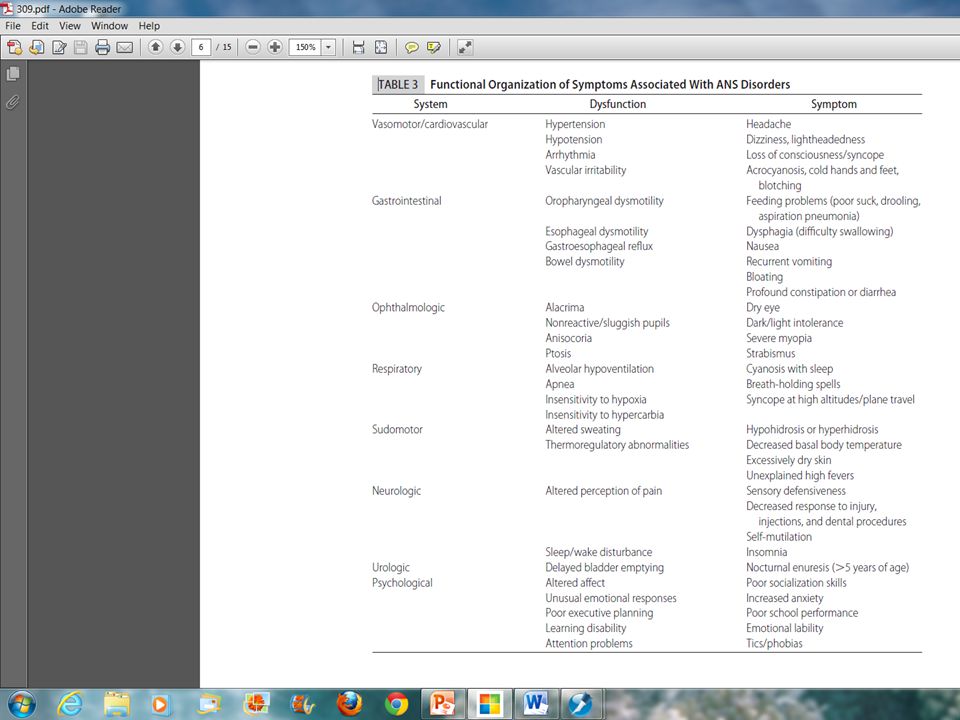
Symptoms Associated With ANS Disorders
System Dysfunction Symptom Ophthalmologic Alacrima Dry Eye Nonreactive/sluggish pupils Dark/light intolerance Ptosis Strabismus Anisocoria Severe myopia Sudomotor Altered sweating Hypohidrosis or hyperhidrosis Urologic) Delayed bladder emptying Nocturnal enuresis GI Dysmotility Gasto perisis
 Delayed bladder emptying. Nocturnal enuresis. GI. Dysmotility. Gasto perisis.")
17
Gastrointestinal Symptoms
Nausea Early satiety, Abdominal cramping after meals, Frequent diarrhea or constipation (or alternating bouts of both),
,")
18
Genitourinary Symptoms
May include Urinary incontinence Urinary frequency and urgency Urinary retention. Erectile dysfunction Decreased libido and inability to achieve orgasm Menstrual Disturanances

19
POTS-Diagnostic Criteria
Development of orthostatic symptoms associated with a heart rate (HR) increment ≥30, usually to ≥120 bpm, within 10 minutes of standing and without orthostatic hypotension. Symptoms of orthostatic intolerance are those due to brain hypoperfusion and sympathetic overaction.
 increment ≥30, usually to ≥120 bpm, within 10 minutes of standing and without orthostatic. hypotension. Symptoms of orthostatic intolerance are those due to brain hypoperfusion and sympathetic overaction.")
20
POTS-Symptoms Due to Cerebral Hypoperfusion
Mechanism: Cerebral autoregulation fails in relation to the onset of dyspnea, hyperpnea, and hypocarbia. Cerebral vasoconstriction in POTS ensues in affected individuals and may be diagnosed as ‘‘hyperventilation syndrome’’ or ‘‘panic attack.’’ Interestingly, similar respiratory signs can be produced in control subjects given sufficient provocation. The underlying cause of orthostatic hyperpnea remains obscure, but postural stimulation appears to be necessary, and Abnoraml interactions between carotid baroreceptor and chemoreceptors are probably the root cause.

21
Acrocyanosis The distribution
of color change does not mimic the distribution of discoloration in Raynaud phenomenon, which is confined to the hand and foot. Rather, as shown in Figure 1, there is more widespread extension, especially in dependent extremities with a mottled appearance comprising islands of pink skin with normal cutaneous blood flow interspersed among prevailing cyanosis with decreased cutaneous blood flow.

22
Tachycardia of POTS could represent absolute
Blood Volume Tachycardia of POTS could represent absolute hypovolemia. This has been demonstrated in some patients with POTS41 and may relate to defective denervation of the kidneys and associated hyporeninemic hypoaldosteronism. 42,43 A reflex response to fluid shifts results in the circulatory insufficiency observed in patients.44 More recent data indicate that hypovolemia tends to be modest and may not by itself explain orthostatic intolerance in these patients.45 Nevertheless, decreased blood volume further impairs venous return and is at least a contributing factor: All compensatory mechanisms for orthostasis depend on circulatory volume adequacy and all will ultimately fail during sufficiently severe hypovolemia. Conversely, repletion of blood volume is often helpful in orthostatic intolerance of whatever cause because it invariably enhances postural venous return., although effects unrelated to blood volume may play a role. Although a primary disturbance in blood volume (or renal volume regulation) has been proposed for some cases of POTS,47-49 volume loading may improve patient well-being nonspecifically as well.
 has been proposed. for some cases of POTS,47-49 volume loading may improve. patient well-being nonspecifically as well.")
23
physical forces comprise a primary
Muscle Pump physical forces comprise a primary defense against lower extremity pooling in human beings in the form of the ‘‘skeletal muscle pump’’ in which contractions of leg and gluteal muscles increase interstitial pressure and propel sequestered venous blood back to the heart. Skeletal muscle may also be involved in neurogenic compensation through chemoreceptors and through local control mechanisms. Recent data indicate that while the muscle pump is normal in most patients with POTS, the muscle pump is defective in a subset of patients with POTS who also have decreased resting peripheral blood flow unrelated to exercise capability but exacerbated by bed rest.

24
Neurovascular Compensation
Neurovascular compensation limits dependent blood pooling. This includes rapid peripheral arterial vasoconstriction limiting flow to the extremities and splanchnic vascular bed while promoting passive venous emptying.53 Active venoconstriction occurs in the splanchnic circulation,54 but there is little evidence for venous beds other than splanchnic contributing to active orthostatic venoconstriction; rather, recent data suggest that other veins and venules contribute to venous return by passive elastic recoil during arterial vasoconstriction.55,56 A useful way to view vascular control systems is to view them as long distance or local control systems.

25
‘‘Long Distance’’ Vascular Control

26
‘‘Local’’ Vascular Control
compensatory response to orthostasis arising from local vasoactive responses are often less well appreciated. These include endothelial vasoactive products (ie, NO, PGI-2, endothelin, EDHF)67,68 metabolites (adenosine, Ca21, CO2, H1 ions, lactate)69-71 autacoids (histamine, bradykinin, 5-HT, PAF, prostaglandins),72 local neurogenic mechanisms such as the axon reflex,73 and neurogenic inflammation (CGRP, substance P),74,75 especially within the cutaneous and enteric circulations. Local responses contribute to classic myogenic, metabolic, and venoarteriolar flow control, which may be important compensatory mechanisms during
67,68 metabolites (adenosine, Ca21, CO2, H1 ions, lactate)69-71 autacoids (histamine, bradykinin, 5-HT, PAF, prostaglandins),72 local neurogenic. mechanisms such as the axon reflex,73 and neurogenic. inflammation (CGRP, substance P),74,75 especially within. the cutaneous and enteric circulations. Local responses. contribute to classic myogenic, metabolic, and venoarteriolar. flow control, which may be important compensatory. mechanisms during.")
27
physiologic variants of POTS
distinguished on the basis of measurements of peripheral blood flow and peripheral arterial resistance in association with characteristic changes in regional circulations:

28
Classification Hyperadrenergic states Autonomic neuropathy involving antiganglionic antibodies Absolute hypovolemia Redistributive form of hypovolemia(central thoracic blood volume is reduced in the upright position, even though overall blood volume is normal)
")
29
Impedance Plethysmography (IPG)
")
31
Normal-flow POTS (Pool in splanchnic circulation due to increased splanchnic blood flow)
Redistributive form of hypovolemia- Splanchnic Blood flow is increased in the supine posture and during incremental tilt Normal peripheral resistance supine and enhanced peripheral resistance upright.. Intact graded reflex-mediated compensatory Intense peripheral vasoconstriction No generalized sympathetic failure. Severe degree of gravitational dependent acrocyanosis due to stagnant hypoxia Probable Mechanisms: Selective splanchnic denervation intact autonomic splanchnic activity confounded by local vasoactive substances e.g. Vasoactive intestinal polypeptide (VIP), substance P, or nitric oxide.
, substance P, or nitric oxide.")
32
Low-flow POTS (Uniform Hypovolemia & Reduced blood flow in multiple regional circulations )
intense peripheral vasoconstriction and low resting cardiac output while supine and decreased blood volume Pallor, extensive supine and upright acrocyanosis, cool skin and extremities, Tachycardia while supine and graded tilt. Defective skeletal muscle pump common Decreased blood flow most notable in the dependent parts of the body splanchnic blood flow does not change during tilt Abnormal Hyperemic blood flow indicating endothelial dysfunction and abnormal local blood flow regulation. Fluid Infusions usually helpful

33
High-flow POTS (Lower body vasodilation)
Increased cardiac index Increased peripheral blood flow, Decreased peripheral resistance in the lower extremities and pelvic segment, Unchanged peripheral blood flow during orthostatic stress May be related to a long tract neuropathy and high cardiac output is caused by inadequate peripheral vasoconstriction supine and upright. Patients typically are acy anotic, warm to touch with extensive filtration, resulting in dependent edema. patients are peripherally vasodilated and mildly tachycardic when supine and have relatively increased blood volume, reduced total peripheral resistance, and high resting cardiac output compared with healthy control subjects.1 Defective Peripheral vasoconstriction during orthostasis remains defective, leading to excess blood delivery to the lower limbs with enhanced microvascular filtration and edema formation.63 Acrocyanosis does not often occur. Persistent upright vasodilation responds to vasoconstrictor therapy with midodrine or similar agents. Often such patients have illness after a viral infection. A perip

34
POTS-ONSET, EPIDEMIOLOGY, AND NATURAL HISTORY
Onset often follows an infectious disease Patients often slowly improve after the initial infectious illness, only to become ill again spontaneously or during an intercurrent infection. 1 Approximately 75% to 80% of patients are women ranging in age from 14 to 50 years22 POTS is relatively uncommon in preadolescent children and may have a distinct pathophysiology in the very young. The illness may follow a remitting and relapsing clinical course, often enduring for years, but seems in many instances self-limited.

35
Symptoms of orthostatic intolerance
Lightheadedness Headache Fatigue Neurocognitive/sleep disorders Exercise intolerance Weakness Hyperpnea/dyspnea Tremulousness Nausea/abdominal pain Sweating Anxiety/palpitations

36
Pathophysiologic Mechanisms (not mutually exclusive) include
Peripheral Autonomic Denervation Hypovolemia venous pooling, β-receptor supersensitivity Impairment of brain stem regulation. Secondary Prolonged deconditioning Psychological factors Poor Nutrition status

37
Physiological Changes upon Assuming the standing position
Abrupt gravitational shift in blood volume and consequent reduction venous return to the heart. Counteracted in the normal person by activation of the baroreceptors.

38
Is excessive postural tachycardia associated with deconditioning rather
than merely being an independent sign of autonomic dysfunction in patients with POTS? Conclusion: HR changes in POTS are not solely because of inactivity resulting in deconditioning Barbara E. U. Burkhardt, MD, Phil R. Fischer, MD, et al- (J Pediatr 2011;158:15-9)
")
39
Deconditioning Definition:
Peak VO2 less than 80% predicted with no evidence of ventilatory limitation to exercise. Ventilatory limitation: Ratio of maximum exercise ventilation to maximum voluntary ventilation of <1

40
POTS Vs. Non POTS Significantly higher resting HR
Delay in HR RECOVERY 5 minutes after exercise Significantly lower stroke volume with increasing exercise work load.

41
Medow and Stewart22 described
a pathophysiological model with 3 groups of patients with POTS—so-called ‘‘low-flow’’, ‘‘normal-flow’’, and ‘‘high-flow’’ POTS—admitting that this distinction may not be clinically relevant yet

42
HR recovery after exercise shows higher HR in
patients with POTS and deconditioned subjects.

43
rapid eye movement (REM)-behavioral sleep disturbances
Sleep Disorders Insomnia Fragmented Sleep rapid eye movement (REM)-behavioral sleep disturbances
-behavioral sleep disturbances.")
44
Dysautonomia Range from transient episodes in otherwise healthy people to progressive neurodegenerative diseases; from conditions in which altered autonomic function plays a primary pathophysiologic role to those in which it worsens an independent pathologic state

45
Orthostatic Hypotension
A decrease in systolic pressure of at least 20 mm Hg or a decrease in diastolic pressure of at least 10 mm Hg within 3 minutes of standing Results from: Intravascular Depletion Prolonged bedridden state and Deconditioning. Autonomic failure-sympathetic Neurocirculatory Failure

46
Chronic Autonomic Failure
Secondary (Most Common) : Diabetes, amyloidosis, or multiple myeloma), Toxic agents (e.g. Alcohol), Medications ( antidepressant, antipsychotic, antihypertensive, or antineoplastic). Primary: Pure Autonomic Failure (PAF) : Orthostatic Hypotension without symptoms or signs of central neurodegeneration. Multiple System Atrophy (MSA): Autonomic failure and progressive central neurodegeneration, Subtypes: Parkinsonian, Cerebellar, and Mixed forms.
 : Diabetes, amyloidosis, or multiple myeloma), Toxic agents (e.g. Alcohol), Medications ( antidepressant, antipsychotic, antihypertensive, or antineoplastic). Primary: Pure Autonomic Failure (PAF) : Orthostatic Hypotension without symptoms or signs of central neurodegeneration. Multiple System Atrophy (MSA): Autonomic failure and progressive central neurodegeneration, Subtypes: Parkinsonian, Cerebellar, and Mixed forms.")
47
Mechanisms of Herbal Remedies
Release Norepinephrine: Ma-Huang Yohimbe Bark

48
Peroneal Muscle Sympathetic Activity
In normal patients Peroneal Muscle Sympathetic Activity approximately doubles during orthostatic stress, with an approximate doubling of the plasma norepinephrine concentration

49
Deficiency of Membrane Norepinephrine Transporter

50
Hyper Noradrenergic Essential Hypertension
Increased cardiac and renal spillover of norepinephrine increased rates of efferent sympathetic nerve firing in the outflow to the skeletal muscle vasculature The sympathetic Mechanism: Activation originates within the CNS and mediated via noradrenergic projections from the brainstem to the forebrain Chronic sympathetic cardiac stimulation and peripheral vasoconstriction; Increased renin secretion and tubular reabsorption of sodium Present in about 40% of young patients with untreated essential hypertension

51
Increased sympathetic and Adrenomedullary Outflows
Panic Disorder Increased sympathetic and Adrenomedullary Outflows Wilkinson DJ, et al. Sympathetic activity in patients with panic disorder at rest,under laboratory mental stress, and during panic attacks. Arch Gen Psychiatry.1998;55:

52
Congestive Heart Failure

53
CHRONIC FATIGUE SYNDROME (CFS)
New, unexplained fatigue that lasts for at least 6 months, is not relieved by rest, and has no clear cause. Associated with 4 or more new symptoms: Memory or concentration problems, Sore Throat Tender Lymphadenopathy, Myalgia, Arthralgia Headache Unrefreshing sleep, Postexertional malaise

54
CFS Women are affected about 3 times more than men Prevelance:10 to
200 to 250/ persons in US

55
CFS Loss of heart rate variability consistent with vagal withdrawal,
increased blood pressure variability consistent with enhanced modulation of sympathetic tone, and impaired baroreflex. Stewart JM, Gewitz MH, Weldon A. Orthostatic intolerancein adolescent chronic fatigue syndrome. Pediatrics. 1999;103:

56
In a recent placebo-controlled
clinical trial of this therapeutic approach (86), 100 patients with CFS who had positive results on tilt-table testing took escalating doses of placebo or fludrocortisone for 9 weeks. Symptoms improved in 10% of the placebo recipients and in 14% of patients receiving fludrocortisone—a statistically nonsignificant difference. The ability to tolerate tilt also did not improve, and there was no correlation between the tilt-table test measures and any of the self-rating categories. Rowe PC, Calkins H, DeBusk K, McKenzie R, Anand R, Sharma G, et al. Fludrocortisone acetate to treat neurally mediated hypotension in chronic fatigue syndrome: a randomized controlled trial. JAMA. 2001;285:52-9. [PMID: ] TREATMENT One of the most important aspects of treatment of patients with dysautonomia is careful education of patients
, 100 patients. with CFS who had positive results on tilt-table testing took. escalating doses of placebo or fludrocortisone for 9 weeks. Symptoms improved in 10% of the placebo recipients and. in 14% of patients receiving fludrocortisone—a statistically. nonsignificant difference. The ability to tolerate tilt also. did not improve, and there was no correlation between the. tilt-table test measures and any of the self-rating categories. Rowe PC, Calkins H, DeBusk K, McKenzie R, Anand R, Sharma G, et al. Fludrocortisone acetate to treat neurally mediated hypotension in chronic fatigue. syndrome: a randomized controlled trial. JAMA. 2001;285:52-9. [PMID: ] TREATMENT. One of the most important aspects of treatment of. patients with dysautonomia is careful education of patients.")
57
TREATMENT 1.Education of patients and caregivers 2. Identify situations that may precipitate or worsen symptoms 3.

58
Non pharmacological Management
Orthostatic intolerance Increase salt and fluid intake Head of bed elevated 4-5 inches Lower body resistance isometric training exercises Smaller low fat, low carb, high protein frequent meals Plan Excersice activities to occur later in the day Avoid morning Hot bath or showers Secretomotor symptoms Artificial tears Over-the-counter oral mucous membrane moisturizers Punctal plugging or cauterization Sudomotor symptoms External cooling devices Avoidance of warm/hot environments if heat intolerance Use of antiperspirants (Drysol) for excessive sweating
 for excessive sweating.")
59
Adequate Fluid intake Fluid intake > 3L/day
Sodium Intake ,000 mg/Day Avoid Caffeine intake Fluid intake log Elevate head of the bed frame to 4 inches above horizontal, by placing cinder blocks under bed frame and not by using pillows. 24-hour urinary sodium excretion should be greater than 150 mEq per 24 hrs. Total Urinary output > 2.5 L/24 hrs

60
Exercise & Reconditioning
Maximize lower body and abdominal tone to improve venous return Start with recumbent exercises Encourage: Repetitively standing on tiptoes Frequently Contract calf muscles and perform knee bends. Formal rehabilitation and Exercise program

61
POTS-Pharmacological Treatment
Midodrine 2.5–15 mg TID Pyridostigmine.15–60 mg TID or SR 180 mg daily Beta Blockers ( Acetabutalol, Betaxalol metoprolol, nadolol, propranolol) Fludrocortisone 0.1–0.2 mg daily or every other day Selective serotonin reuptake inhibitors (SSRIs) Erythropoietin 2000–10,000 units subcutaneously, weekly, titrated to hematocrit of 55%
 Fludrocortisone 0.1–0.2 mg daily or every other day. Selective serotonin reuptake inhibitors (SSRIs) Erythropoietin 2000–10,000 units subcutaneously, weekly, titrated to hematocrit of 55%")
62
Midodrin Peripherally acting a-adrenergic receptor agonist , only
Duration of action: Up to 4 hours . It is typically used at . Side effects: scalp tingling and ‘‘goose bumps’’ due to piloerection at the skin surface, supine hypertension, and urinary retention. Generally, patients may have some control of their doses so that on days when they are more symptomatic and their orthostatic blood pressure drop is more severe, they may take a higher dose of the medication.

63
Pyridostigmine (Mestinon)
Acetylcholinesterase inhibitor: Potentiales acetylcholine neurotransmission at peripheral autonomic ganglia, thereby increasing peripheral vasoconstriction via sympathetic nerve fiber transmission. Increases vagal cardiac input. The most common side effects: increased salivation, sweating, and increased gastrointestinal motility. Rarely patients may experience muscle fasciculations.

64
Autoimmune Autonomic Neuropathy
Plasmapheresis Infusion of intravenous immunoglobulin (IVIg) Oral immunosuppressive medications for long-term therapy
 Oral immunosuppressive medications for long-term therapy")
65
Acute idiopathic Anhidrosis or Hypohidrosis:,
May be a form of limited autonomic neuropathy, skin biopsy: Lymphocytic infiltration around sweat glands and ducts. RX: Short course oral prednisone or IV Methylprednisolone Chronic Anhidrosis:

66
Localized: subcutaneous injections of botulinum
Hyperhidrosis-RX Localized: subcutaneous injections of botulinum toxin to denervate sweat glands.1 Generalized Hyperhidrosis: medications with strong anticholinergic side effect, such as amitriptyline or glycopyrrolate. Topical treatments for excessive sweating include aluminum chloride (the active ingredient in antiperspirants) and topical compounded cream formulations of glycopyrrolate.
 and topical compounded. cream formulations of glycopyrrolate.")
67
Secretomotor Abnormalities-RX
Xerophthalmia: Chronic, severe dry eye has a risk of development of corneal abnormalities and should be treated aggressively. Punctal plugging Artificial tears and cyclosporine eye drops locally, fish oil oral supplements. Xerostomia: over-the-counter agents to control symptoms of dry mouth; pyridostigmine in refractory cases.

68
Multiple system Atrophy (Shy-Drager syndrome)
")
69
Norepinephrine Transporter Protein Deficiency
Another recent autonomic condition producing a complex form of POTS is the. Reported in only a single family. Specific genetic defect in norepinephrine transporter protein deficiency64 exerting both central and peripheral effects on vascular regulation.65 Despite its rarity, the illness has furnished an ideal monogenetic model for autonomic illness, and appropriate animal knock-out models have been constructed and investigated.66

70
Noradrenergic projections
Broadly distributed throughout the CNS and PNS Play important modulatory roles in attention, pain perception, learning, memory, and autonomic function originate from a small population of brainstem nuclei, the noradrenergic cell groups The largest of these groups is the locus coeruleus (LC), which projects widely to the cortex, amygdala, olfactory bulb, hippocampus, septum, hypothalamus, brainstem nuclei, and spinal cord
, which projects widely to the cortex, amygdala, olfactory bulb, hippocampus, septum, hypothalamus, brainstem nuclei, and spinal cord.")
71
(NE) transporter Regulate the duration of NE neurotransmission by removal of the NE from the extracellular space. 80–90% of released NE may be recaptured and re released, NETs are important targets of antidepressants such as desipramine and reboxetine and for drugs of abuse including cocaine and amphetamine (Ritz et al., 1990; Pacholczyk et al., 1991; Chen and Reith, 1994; Wall et al., 1995; Tatsumi et al., 1997). Loss of NETs or NE clearance has been associated with depression (Klimek et al., 1997) and with several heart and vascular system diseases including orthostatic intolerance (Jacob et al., 1999).
. Loss of NETs or NE clearance. has been associated with depression (Klimek et al., 1997) and with several heart and vascular system diseases including. orthostatic intolerance (Jacob et al., 1999).")
72
Hereditary Sensory and Autonomic Neuropathies (HSANs)
Genetic Errors affecting a specific aspect of small fiber neurodevelopment Variable phenotypic expression (HSAN type I), AD, presenting in the second decade of life, (HSAN type III)=Familial Dysautonomia &III) AR, present at birth. (HSAN type IV) congenital insensitivity to pain with anhidrosis (CIPA)
, AD, presenting in the second decade of life, (HSAN type III)=Familial Dysautonomia &III) AR, present at birth. (HSAN type IV) congenital insensitivity to pain with anhidrosis (CIPA)")
73
RX: Clonidine to control vomiting and the dysautonomic crisis,
FD Affected gene IKBKAP that aids in expression of various neurotransmitters . Inadequate development, and limited survival, of sensory and autonomic neurons. the sympathetic neurons are more exetnsively affected than the parasympathetic Hypoactive Corneal and tendon reflexes, Diminished taste appreciation due to absence of lingual fungiform papillae Vibratory sensory loss and impaired coordination with age Absence of tears(alacrima) with emotional crying Poor oral coordination and hypotonia are and frequent GER and aspiration Protracted episodes of nausea and vomiting triggered by emotional or physicalstress Frequent erythematous skin blotching and hyperhidrosis Extreme hypertension and sever postural hypotension without compensatory tachycardia Relative insensitivity to hypoxemia RX: Clonidine to control vomiting and the dysautonomic crisis, Fludrocortisone and midodrine to mange Hypotension.
 with emotional crying. Poor oral coordination and hypotonia are and frequent GER and aspiration. Protracted episodes of nausea and vomiting triggered by emotional or physicalstress. Frequent erythematous skin blotching and hyperhidrosis. Extreme hypertension and sever postural hypotension without compensatory tachycardia. Relative insensitivity to hypoxemia. RX: Clonidine to control vomiting and the dysautonomic crisis, Fludrocortisone and midodrine to mange Hypotension.")
74
probably secondary to impaired thoracolumbar sympathetic outflow.
CIPA/HSAN type IV Anhidrosis causes episodic fevers and extreme hyperpyrexia that is usually the earliest probably secondary to impaired thoracolumbar sympathetic outflow. thick and calloused appearance of the skin with lichenification of palms, dystrophic nails, and areas of hypotrichosis on the scalp.38 Miosis due parasympathetic dysfunction, mild postural hypotension. The insensitivity to pain is profound and can result in self-mutilation, autoamputation, and corneal scarring

Similar presentations







>")

 ~5% of total.>")
 AUTONOMIC NERVOUS SYSTEM PHARMACOLOGY.>")





 regardless of changes externally. Communication.>")
 Cardiovascular system (fast) (a) cardiac output increase c.o., increase pressure (b) peripheral.>")






