Download presentation
Presentation is loading. Please wait.

1
Supporting Development of the Premature Infant after Discharge from the NICU
November 6, 2009 Susan M. Bickel, OTR/L Denise Doorlag, OTR/L Bronson Methodist Hospital Rehabilitation Department My experience as an OT 10 years at Bronson describe mentoring in the nicu preface that this Lecture is about Bronson's NICU

2
Objectives Able to state the progression of normal development of the preterm infant Able to identify the red flags of development and potential problems of the preterm infant Able to select appropriate developmental activities for the preterm infant

3
The Neonatal Intensive Care Unit at Bronson Methodist Hospital
Bronson is a Level III NICU 45 bed unit – all private rooms 33 beds are intensive care 12 beds are intermediate care

4
Our NICU Team Neonatologists Nursing Social Worker Case Managers
Dietitian Respiratory Therapists Developmental Specialist (OT) Pharmacist Chaplain Music Therapist Child Life Specialist Lactation Consultant Meet the NICU team...need to get to know all these people on the unit so you can communicate and work closely with them all
 Pharmacist. Chaplain. Music Therapist. Child Life Specialist. Lactation Consultant. Meet the NICU team...need to get to know all these people on the unit so you can communicate and work closely with them all.")
5
The Role of the OT in the NICU
Developmental assessment and treatment Feeding assessment and treatment Education to nursing and family

6
Definitions NICU – Neonatal intensive care unit
Neonate – newborn infant-typically from birth through day 28 of life Gestational Age – the length of time the infant was in utero Post Conceptual Age – the age the infant is in weeks from conception and as he ages Adjusted/Corrected Age or Conceptual age – same as post conceptual age Chronological Age – the age of the infant calculated from day of birth These are some terms specific to the NICU It's important to know how to correct for a babies age Ex: infant born at 28 wks is actually 12 wks or 3 months early so when infant is 6 mo old..actually acting like 3 months

7
Definitions Term – infant born 37 – 42 weeks
Post Term – infant born over 42 weeks Preterm – infant born 28 – less than 37 weeks Extremely Preterm – infant born under 28 weeks How to categorize a neonate

8
Definitions Appropriate for Gestational Age (AGA) – infant’s weight falls between a normal range of the 10th and 90th percentile for that gestational age Small for Gestational Age (SGS) – infant’s weight is less than the 10th percentile for that gestational age Large for Gestational Age (LGA) – infant’s weight is above the 90th percentile for that gestational age Intrauterine Growth Retardation (IUGR) – the infant’s weight and length are low for age
 – infant’s weight falls between a normal range of the 10th and 90th percentile for that gestational age. Small for Gestational Age (SGS) – infant’s weight is less than the 10th percentile for that gestational age. Large for Gestational Age (LGA) – infant’s weight is above the 90th percentile for that gestational age. Intrauterine Growth Retardation (IUGR) – the infant’s weight and length are low for age.")
9
21 weeks and six days on Oct. 24, Weighing less than ten ounces and measuring only 9.5 inches in length

10
1 pound 6 ounces. 24 weeks

11
Medical Conditions Respiratory complications
Respiratory Distress Syndrome (RDS) – when tiny air sacs in the infant’s lungs do not stay open due to lack of surfactant Chronic Lung Disease – complications of the lungs that persist after 36 weeks of age requiring supplemental oxygen Bronchopulmonary Dysplasia (BPD) – abnormal growth of the infants airways and lungs due to high doses of oxygen and prolonged ventilator use typical resp diseases all related to being premature
 – when tiny air sacs in the infant’s lungs do not stay open due to lack of surfactant. Chronic Lung Disease – complications of the lungs that persist after 36 weeks of age requiring supplemental oxygen. Bronchopulmonary Dysplasia (BPD) – abnormal growth of the infants airways and lungs due to high doses of oxygen and prolonged ventilator use. typical resp diseases all related to being premature.")
12
Medical Conditions Cardiac Complications
Patent Ductus Arteriosus (PDA) – a small blood vessel that connects the pulmonary artery to the descending aorta that should close on its own after birth; if it does not close, it may require medical or surgical management Pulmonary Hypertension – increased pressure in the pulmonary blood flow Atrial Septal Defect – a heart defect where there is an opening in the atria Ventricular Septal Defect – a hole in the septum between the ventricles in the heart Infants with cardiac complications may be weaker and fatigue quicker with eating
 – a small blood vessel that connects the pulmonary artery to the descending aorta that should close on its own after birth; if it does not close, it may require medical or surgical management. Pulmonary Hypertension – increased pressure in the pulmonary blood flow. Atrial Septal Defect – a heart defect where there is an opening in the atria. Ventricular Septal Defect – a hole in the septum between the ventricles in the heart. Infants with cardiac complications may be weaker and fatigue quicker with eating.")
13
Medical Conditions Neurological Complications
Intraventricular Hemorrhage (IVH) – bleeding in the brain, often around the ventricles; very low birth weight infants are at high risk Hydrocephalus – an increase in cerebrospinal fluid in the brain Periventricular Leukomalacia (PVL) – decreased blood supply to the brain causing hollow spaces in the brain OT will often assess premies with any neurological insults to help assess tone and feeding skills ex: how a low tone infant may have difficulty feeding relationship between low tone and feeding
 – bleeding in the brain, often around the ventricles; very low birth weight infants are at high risk. Hydrocephalus – an increase in cerebrospinal fluid in the brain. Periventricular Leukomalacia (PVL) – decreased blood supply to the brain causing hollow spaces in the brain. OT will often assess premies with any neurological insults to help assess tone and feeding skills. ex: how a low tone infant may have difficulty feeding. relationship between low tone and feeding.")
14
Medical Conditions Neurological Complications
Hypoxic-ischemic Encephalopathy – injury to the brain due to decreased oxygen to the infant Myelomeningocele – a protruding portion of the spinal cord and membranes Infants with Myelom will often need ROM exercise for lower extremity Give parents a home exer program

15
Medical Conditions Nutritional and GI complications
Necrotizing Entercolitis (NEC) – inflammation of part of the intestine that may result in the death of that tissue; may allow bacteria to leak into the abdomen and cause infection Short – Gut Syndrome – infant is missing some intestine or too much has been removed Gastroesophageal Reflux Disease – contents in the stomach flow back up into the esophagus Many premies are prone to getting NEC..often can be medically managed...at times req surgery....then may have gut problems GERD- can be common in NICU and Peds...OT can help make feeding recs and suggest formula changes
 – inflammation of part of the intestine that may result in the death of that tissue; may allow bacteria to leak into the abdomen and cause infection. Short – Gut Syndrome – infant is missing some intestine or too much has been removed. Gastroesophageal Reflux Disease – contents in the stomach flow back up into the esophagus. Many premies are prone to getting NEC..often can be medically managed...at times req surgery....then may have gut problems. GERD- can be common in NICU and Peds...OT can help make feeding recs and suggest formula changes.")
16
Medical Conditions Nutritional and GI complications
Gastroschisis – a hole in the abdominal wall resulting in some of the intestines developing outside the body Hirschsprung’s Disease – an extremely dilated colon requiring surgical removal of the affected area; lack of ganglia needed for peristalsis Omphalocele – a congenital hernia of the umbilicus Gastroschisis will require surgery-most feed normally once fixed

17
Medical Conditions Malformations
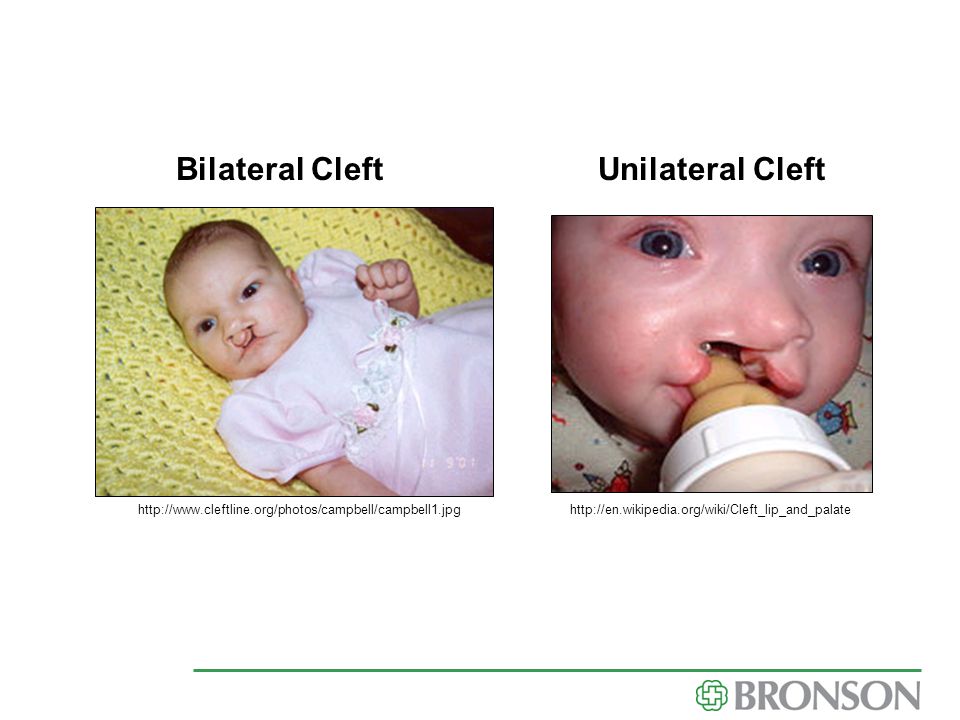
Club feet – where one or both feet turn into adduction and supination Cleft palate – a separation of the hard or soft palate Cleft lip – a separation of the upper lip and often the upper dental ridge OT works closely with all three of these malform splinting club feet with fragile skin give example teaching family feeding tech...cleft palate bottle

18
Bilateral Cleft Unilateral Cleft
19
Club Foot

20
Medical Conditions Blood Complications
Anemia – low hemoglobin in the blood Hyperbilirubemia – jaundice due to an excess of bilirubin in the blood Sepsis – infection in the blood Visual Complications Retinopathy of Prematurity (ROP) – an abnormal amount of blood vessels in the retina often caused by increased oxygen use in infants severe cases may result in retinal detachment and blindness Infant who is Jaundice will need bili lights or blanket
 – an abnormal amount of blood vessels in the retina. often caused by increased oxygen use in infants. severe cases may result in retinal detachment and blindness. Infant who is Jaundice will need bili lights or blanket.")
21
Medical Conditions Other Complications
Brachial Plexus Injury – damage to the brachial plexus during a difficult birth that may result in paralysis or weakness of the arm IDM – infant of a diabetic mother Down’s Syndrome/Trisomy 21 – most common syndrome characterized by one additional chromosome 21 OT goes in and teaches family handling tech and ROM exer for brachial plexus OT is often involved in therapy early on with Down's syndrome feeding and exer

22
Down’s Syndrome

23
A Typical Stay in the NICU
Nursing Care One nurse may have 3-4 babies to care for Infant is put on a 3 hour care schedule Diaper changed, meds given, clothes changed, blood pressure and temperature taken, heel stick/blood draw, suctioning, CPAP/vent changes and adjustments, feeding given through tube or by bottle, baths, feeding tube checked, position changed Infant is then able to have a calm/quiet sleep period until the next care time Often interrupted by other care such as physician, x-ray, therapy, respiratory care, eye exams, ECHOs, ultrasounds, and other medical care

25
A Typical Stay in the NICU
Family Visitation Families are allowed to visit whenever they want to be there Family is limited to mom/dad, grandma/grandpa and siblings Mom and dad can bring other visitors with them Families are not allowed to sleep at the bedside Barriers to family visits Families that live far away often have transportation problems Families that need to work Families have other children at home

26
A Typical Stay in the NICU
Ups and Downs of Medical Status Extremely premature infants have multiple system problems Each day early on in life can bring a new problem The need for emergent surgery may arise An infant may go through several surgeries throughout their stay Changes in respiratory status happen daily Even infants who are doing well, can unexpectedly take a turn for the worse

27
Shows CPAP, feeding tube, monitor leads
Shows CPAP, feeding tube, monitor leads

28
Development of the Premature Infant
The infant at 31 weeks and under: Behavior Primarily in a sleep state Brief periods of alertness when closer to 31 weeks Able to consistently respond positively and negatively to stimulation Easily startled and agitated Motor The extreme premature infants are generally hypotonic until about 29 weeks Oral Motor The sucking reflex is beginning but is weak and not very coordinated

29
Development of the Premature Infant
The infant at 32 – 36 weeks: Behavior Able to demonstrate brief alert periods Beginning to open eyes in response to stimulation Attempts to calm self (hands to mouth) Motor At 32 weeks developing more consistent hip flexion Towards 36 weeks, demonstrating more consistent upper extremity flexion Oral Motor Demonstrating the rooting reflex and beginning to work on oral feedings
 Motor. At 32 weeks developing more consistent hip flexion. Towards 36 weeks, demonstrating more consistent upper extremity flexion. Oral Motor. Demonstrating the rooting reflex and beginning to work on oral feedings.")
30
Development of the Premature Infant
The infant at 37 – 40 weeks: Behavior Infant awakens on his own Tolerates longer alert periods with greater tolerance to stimulation Beginning to track and focus with eyes Motor Flexor tone dominates throughout all four extremities More spontaneous and controlled movements Oral Motor Consistent rooting reflex Organized suck, swallow, breathe coordination

31
How to Correct for Gestational Age
It is recommended that a child’s age is corrected up to 2 years of age. Subtract the number of weeks or months that the infant was early from the current age of the infant Example: if the infant was born at 28 weeks gestation, he was born 3 months early. When he is 6 months old, his corrected age is 3 months. He then should be expected to do 3 month old skills. The infant’s head, weight, and length measurements should be based on his corrected age. Remind parents how to correct for their infant’s age and also have the parent remind the doctor what the infant’s corrected age is.

32
Premature Infant vs. Term Infant
Flexor tone of the preterm infant at term age is not as great as the infant born at term The preterm infant at term age will have less head control than the infant born at term The preterm infant at term age will have less predictable sleep-wake cycles and feeding patterns than the infant born at term Breastfeeding skills are not as mature in the preterm infant at term age The preterm infant at term age has decreased ability to tolerate multiple types of stimulation

33
Why Does the Premature Infant Develop Differently?
Lack of the uterine environment Inability to develop physiological flexion Decreased exposure to movement and joint compression Early exposure to sound, light and other stimuli Poor positioning Prolonged positioning in the supine position resulting in poor head shape and weakened flexor muscles

34
Why Does the Premature Infant Develop Differently?
Respiratory complications and medical instability Abnormal tightness in muscles Delay of initiation of feeding Increase in noxious stimulus associated with care Early fatigue and decreased endurance with all activity Infants being sedated or on prolonged ventilation may develop extending postures making it difficult to move normally and to self-organize (article: “Enhancing Occupational Performance in Infants in the NICU”)
")
36
Why Does the Premature Infant Develop Differently?
Increased noxious stimuli and decreased pleasing interactions “Research shows that highly stimulating physical environments such as the NICU are stressful to infants and may affect their self-regulation and ability to engage in activities.” (article: “Enhancing Occupational performance in Infants in the NICU”) Due to high amounts of unpleasing stimuli in the NICU, infants have a hard time exploring the caregiver’s face and visually following the caregiver in poor social play (article: “Enhancing Occupational performance in Infants in the NICU”)
 Due to high amounts of unpleasing stimuli in the NICU, infants have a hard time exploring the caregiver’s face and visually following the caregiver in poor social play (article: Enhancing Occupational performance in Infants in the NICU )")
37
common CPAP...cont post airway pressure...keeping lungs open to help baby breathe better

38
Potential Problems of the Premature Infant
Muscle tightness Muscle weakness Poor endurance Visual problems Feeding problems Behavioral and Sensory problems

39
Red Flags of Preterm Development
Muscle tightness Infant prefers to turn head to one side Flat spots on back/side of head Arching Difficulty bringing hands to the middle Standing on toes Delayed rolling Difficulty changing diaper/changing clothes

40
How We Can Help Frequent position changes Tummy time
Range of motion exercises/stretching Eliminate walkers, exersaucers, and jumpers Helmet use for severe plagiocephaly Possible referral to physician for medication Referral to physical therapy and occupational therapy Educating parents on proper progression of developmental milestones Teach parents appropriate play activities to work on midline, rolling, and tracking

41
Red Flags of Preterm Development
Muscle weakness Poor head control Floppy baby Delayed sitting Delayed rolling Delayed crawling Decreased active arm and leg movements Tires easily with activity An OT in acute care needs to have a plan for the day - but yet needs to be flexible because things are always changing

42
How We Can Help Practice supported upright sit
Range of motion exercises Tummy time to help strengthen trunk muscles Keep newborn swaddled when sleeping Use mobiles, play gyms, and wrist rattles to encourage movement Pull to sit activities Help facilitate muscle tone Eliminate walkers, exersaucers and jumpers Position infant so he can easily get hands to mouth Possible referral to PT/OT, if developmental milestones are not being met

44
Red Flags of Preterm Development
Poor endurance Sleepy baby Unable to take whole feeding Tires easily with activity

45
How We Can Help Help parents create a schedule for baby
Allow infant to have full, restful sleep in crib, away from disturbances Help parents understand why baby is fatiguing

46
Red Flags of Preterm Development
Visual Problems Infant does not make eye contact with caregiver Infant does not track toy or face Infant’s eyes are averted to the left or right Infant prefers to look to the right or the left only demonstrate program on doll

47
How We Can Help Provide a variety of toys that offer visual stimulation Educating parents on appropriate amount of visual stimulation Education on retinopathy of prematurity and how it may affect the baby Facilitating infant to look to the direction he favors the least Identify whether there is tightness in the neck, in which case, range of motion will be needed Infants respond best to visual stimulation that has depth such as parent’s face

48
Red Flags of Preterm Development
Feeding Problems Infant is not gaining weight Infant falls asleep during feeding Infant is irritable during feeding Gagging or difficulty progressing to solids Infant chokes or coughs during feeding Infant changes color during feeding Infant has increase in vomiting/spitting up

49
How We Can Help If infant is not gaining weight, refer to the physician Help parents create a feeding schedule Help parents understand how much food the infant should be eating Educate parents on why infant fatigues when eating Consider need to try a different flow rate/nipple Educate parents on symptoms and recommendations of reflux Educate on signs of aspiration Consider referral to OT or speech for feeding therapy Support the breastfeeding mom by referring to a lactation specialist, if needed

50
Red Flags of Preterm Development
Behavioral and Sensory Problems Increased crying or irritability Difficulty tolerating movement/position changes Sleeping an unusual amount or difficulty waking Delayed smiling or laughing Inconsolable Frequent and abrupt state changes Infant not able to stay in a nice alert state for long Not tolerating bath time Frantic movements when unswaddled Aversive to certain foods or stimulation around mouth

51
How We Can Help Never, Never, Never Shake A Baby! Keep infant swaddled
Provide slow, gentle movement Help parents create a schedule Teach consoling techniques Teach how to give proprioceptive input Decrease or modify stimulation to a tolerable level Support alert state with calm, positive interactions Offer age appropriate social play Never, Never, Never Shake A Baby!

52
Assessing Behavior 1 = Deep sleep –infant is very still and difficult to wake up 2 = Light sleep – infant moves arms and legs to change position but usually goes back to sleep 3 = Drowsy – infant is just starting to wake up; eyes may be half closed; infant looks very tired 4 = Quiet Alert – infant’s eyes are wide open and bright; infant is quiet but looks very interested; good attention 5 = Active Alert – infant is awake but is becoming more active and may become fussy 6 = Crying – may mean infant is hungry, tired, wet, or needs help to calm down This tool is used to describe the infants behavior throughout your assessment. Helps determine readiness to feed

53
Why We Need YOU! Some developmental problems may not be detected until after discharged home Parents need frequent reeducation on development Sometimes parents need to be taught how to PLAY Young parents need more support Pediatricians are not always able to offer the time to discuss developmental problems Developmental delays may get missed at well child visits Due to an increased survival of very low birth weight infants, there is an increase in prevalence of lifelong motor, cognitive and behavioral dysfunction.(article: “Positive Screening for Autism in Ex-preterm Infants: prevalence and Risk Factors”).
.")
54
References Limberopoulos C, et al. Positive Screening for Autism in Ex-preterm Infants: Prevalence and Risk Factors. Pediatrics.2008;121(4): Maddalena P, Gibbons S. Cerebellar Hemorrhage in Extremely Low Birth Weight Infants: Incidence, Risk Factors, and Impact on Long-Term Outcomes, Neonatal Network. 2008; 27(6): Vergara E. Enhancing Occupational Performance in Infants in the NICU. OT Practice ; July 8: Van Haastert IC, etal. Early Gross Motor Development of Preterm Infants According to the Alberta Infant Motor Scale. The Journal of Pediatrics. 2006; Nov; Wilson-Costello D, et al. Improved Neurodevelopmental Outcomes for Extremely Low Birth Weight Infants in Pediatrics. 2007; 119(1):
: Maddalena P, Gibbons S. Cerebellar Hemorrhage in Extremely Low Birth Weight Infants: Incidence, Risk Factors, and Impact on Long-Term Outcomes, Neonatal Network. 2008; 27(6): Vergara E. Enhancing Occupational Performance in Infants in the NICU. OT Practice. 2002; July 8: Van Haastert IC, etal. Early Gross Motor Development of Preterm Infants According to the Alberta Infant Motor Scale. The Journal of Pediatrics. 2006; Nov; Wilson-Costello D, et al. Improved Neurodevelopmental Outcomes for Extremely Low Birth Weight Infants in Pediatrics. 2007; 119(1):")
55
References Da Costa SP, et al. Sucking and Swallowing in Infants and Diagnostic Tools. Journal of Perinatology. 2008; 28: Limperopoulos C, et al. Does Cerebellar Injury in Premature Infants Contribute to the High Prevalence of Long-term Cognitive, Learning, and Behavioral Disability in Survivors. Pediatrics. 2007; 120(3): Vandenberg K. Assessing Behavior Organization in Infants. Physical Assessment of the Newborn: A Comprehensive Approach to the Art of the Physical Vergara E, Bigsby R. Developmental & Therapeutic Interventions in the NICU Paul H Brookes Publishing Co. Staff of The Children’s Hospital Denver, Colorado, Cregar P (editor). Developmental Interventions for Preterm and High-Risk Infants Therapy Skill Builders.
: Vandenberg K. Assessing Behavior Organization in Infants. Physical Assessment of the Newborn: A Comprehensive Approach to the Art of the Physical Vergara E, Bigsby R. Developmental & Therapeutic Interventions in the NICU Paul H Brookes Publishing Co. Staff of The Children’s Hospital Denver, Colorado, Cregar P (editor). Developmental Interventions for Preterm and High-Risk Infants Therapy Skill Builders.")
Similar presentations