Download presentation
Presentation is loading. Please wait.

1
Toronto I-II 12:45 pm Peer-based interventions in the prevention, engagement and treatment cascade: Opportunities and challenges Jane Simoni Professor of Psychology and clinical psychologist in the development and evaluation of health promotion interventions Discussion Panel: Mike Hamilton, Gareth Henry Haoua Inoua, Tara Jewal, Percy Lezard, Sean LeBlanc, Duncan MacLachlan, Moderator: Francisco Ibáñez-Carrasco

2
Opportunities and challenges for peer-based interventions in the HIV prevention, engagement and treatment cascade Jane M. Simoni, Ph.D. University of Washington Ontario HIV Treatment Network: 2013 Research Conference Toronto, Ontario November 18, 2013

3
Overview Research reviews of peer interventions Project PAL: What we tried and what we learned Benefits and challenges to implementing and sustaining peer-based interventions Notes from the field: Recommendations for implementation

4
PEER Support Global tradition of non-professional, community-based health care workers community-based health care workers –Practical knowledge of local needs and preferences preferences –Shared culture facilitates engagement and trust Diversity of roles reflected in diversity of titles –Community health worker, buddy, promotor, accompagnateur, advocate, lay worker, peer Policy statements promote use of peers to achieve public health goals, especially among marginalized or disadvantaged populations

5
What Defines a Peer? Essential Elements Peers share with the target group key personal characteristics, circumstances, or experiences (i.e., “peerness”) The contributions/benefits of peers’ work derive largely from their status as peers Peers lack professional training or accreditation/status in the scope of their work Peers function intentionally according to standard protocols, rather then operating solely as part of a naturally occurring social network Simoni et al., 2011
 The contributions/benefits of peers’ work derive largely from their status as peers Peers lack professional training or accreditation/status in the scope of their work Peers function intentionally according to standard protocols, rather then operating solely as part of a naturally occurring social network Simoni et al.,")
6
Literature Review: Is peer support beneficial?

7
Are peer interventions for HIV efficacious? A systematic review Simoni et al., 2011, AIDS and Behavior Methods –Searched PubMed and PsychInfo –Search terms: HIV, peer*, intervention(s) –Scanned references and consulted colleagues –Articles published before –Articles published before November 1, 2010 –Written in English Included articles that: – –Peers were the only or a main interventions –Addressed HIV-related health concern as main outcome –Used statistical methods of evaluation –Was a primary report of the results
 –Scanned references and consulted colleagues –Articles published before –Articles published before November 1, 2010 –Written in English Included articles that: – –Peers were the only or a main interventions –Addressed HIV-related health concern as main outcome –Used statistical methods of evaluation –Was a primary report of the results.")
8
studies were identified 518 studies were identified excluded during abstract review 71 excluded during data extraction process 330 excluded during abstract review 71 excluded during data extraction process 117 met criteria 28 were RCTs 54 quasi-experimental 35 cross-sectional Mostly in the US ( n =51) but newer studies represent developing world ( n =54)
 but newer studies represent developing world ( n =54)")
9
Targeted outcomes - n (%) Examples: – –unprotected anal intercourse and condom use – –perceived risk, perceived importance, beliefs, intention – –needle sharing, cleaning needles, methamphetamine use – –HIV tests, CD4 counts, tests for STIs, and viral load – –electronically monitored adherence, condom sales
 Examples: – –unprotected anal intercourse and condom use – –perceived risk, perceived importance, beliefs, intention – –needle sharing, cleaning needles, methamphetamine use – –HIV tests, CD4 counts, tests for STIs, and viral load – –electronically monitored adherence, condom sales")
10
Format of peer interventions 68 formal meetings or structured groups 40 outreach activities 24 formal one-on-one 15 popular opinion leader Populations – n (%)
")
11
Efficacy of peer interventions was assessed by summing the number of studies with a supportive result for at least one of the variables in the specified domain (a very liberal estimate). Peer interventions appear to be most successful with attitudinal and HIV knowledge outcomes, less so with substance use, risky sex, and biological outcomes. Overall interventions were efficacious, although the likelihood of a supportive result varied according to outcome domain: Peer interventions appear to be most successful with attitudinal and HIV knowledge outcomes, less so with substance use, risky sex, and biological outcomes. Outcomes that did not rely on self-report (biomarkers/other) were seldom used and much less likely to offer evidence of success
 were seldom used and much less likely to offer evidence of success.")
12
Is study design rigor a moderator of intervention efficacy? 5 out of 6 domains did not differ in efficacy by study design The exception was biological outcomes – –More rigorous designs were LESS likely to demonstrate support for the peer intervention under study

13
Moderators of outcome domains Study location – –Studies in the U.S. were more effective at changing attitudes and cognitions than studies in developing countries Intervention modality – –Studies that used outreach were more effective at changing substance use than studies without outreach Population studied – –Studies intervening with non-PLWHA were more effective at changing sexual behavior than studies targeting PLWHA – –Studies intervening with non-MSM were more effective at changing attitudes/cognitions than studies targeting MSM

14
Conclusions from Simoni et al., 2011 “[F]indings suggest that we can have some confidence in peer interventions, yet more data are needed demonstrating an effect in the most rigorous study designs and with outcomes that are not potentially affected by respondent bias.”
![Conclusions from Simoni et al., 2011 [F]indings suggest that we can have some confidence in peer interventions, yet more data are needed demonstrating an effect in the most rigorous study designs and with outcomes that are not potentially affected by respondent bias.](http://images.slideplayer.com/13/3611389/slides/slide_14.jpg "Conclusions from Simoni et al., 2011 [F]indings suggest that we can have some confidence in peer interventions, yet more data are needed demonstrating an effect in the most rigorous study designs and with outcomes that are not potentially affected by respondent bias.")
15
Kerrigan et al. (2013). AIDS and Behavior. Female Sex Workers: A Systematic Review Kerrigan et al. (2013). AIDS and Behavior. Review & meta-analysis in low/middle income countries (1990– 2010) 6,664 citations, 10 met inclusion criteria HIV – – n =2 observational with protective combined effect (OR: 0.84, 95% CI: 0.71–0.99) STI infection – –n=1 longitudinal showed gonorrhoea/chlamydia (OR: 0.51, 95% CI: 0.26–0.99) – –Observational studies showed gonorrhoea (OR: 0.65, 95% CI: 0.47–0.90), but non-significant on chlamydia and syphilis Condom use – –n=1 RCT showed improvements with clients (ß: 0.3447, p = 0.002) – –n=1 longitudinal showed improvements with regular clients (OR: 1.9, 95% CI: 1.1– 3.3), but no change with new clients – –Observational studies showed improvements with new clients (OR: 3.04, 95 % CI: 1.29–7.17), regular clients (OR: 2.20, 95 % CI: 1.41–3.42), and all clients (OR: 5.87, 95 % CI: 2.88–11.94), but not regular non-paying partners Conclusion: “Overall, community empowerment-based HIV prevention was associated with significant improvements across HIV outcomes and settings.”
. AIDS and Behavior. Review & meta-analysis in low/middle income countries (1990– 2010) 6,664 citations, 10 met inclusion criteria HIV – – n =2 observational with protective combined effect (OR: 0.84, 95% CI: 0.71–0.99) STI infection – –n=1 longitudinal showed gonorrhoea/chlamydia (OR: 0.51, 95% CI: 0.26–0.99) – –Observational studies showed gonorrhoea (OR: 0.65, 95% CI: 0.47–0.90), but non-significant on chlamydia and syphilis Condom use – –n=1 RCT showed improvements with clients (ß: , p = 0.002) – –n=1 longitudinal showed improvements with regular clients (OR: 1.9, 95% CI: 1.1– 3.3), but no change with new clients – –Observational studies showed improvements with new clients (OR: 3.04, 95 % CI: 1.29–7.17), regular clients (OR: 2.20, 95 % CI: 1.41–3.42), and all clients (OR: 5.87, 95 % CI: 2.88–11.94), but not regular non-paying partners Conclusion: Overall, community empowerment-based HIV prevention was associated with significant improvements across HIV outcomes and settings. .")
16
Peer-led interventions to reduce HIV risk of youth: A review Maticka-Tyndale et al. (2009) Evaluation and program planning Review and synthesis n =24 peer-led programs in low/middle income countries HIV/AIDS risk reduction targeting youth in their communities
 Evaluation and program planning Review and synthesis n =24 peer-led programs in low/middle income countries HIV/AIDS risk reduction targeting youth in their communities.")
17
Peer-led interventions to reduce HIV risk of youth: A review Maticka-Tyndale et al. (2009) Evaluation and program planning Findings Majority show positive change in knowledge and condom use Effects on other sexual behaviors and STIs were equivocal
 Evaluation and program planning Findings Majority show positive change in knowledge and condom use Effects on other sexual behaviors and STIs were equivocal.")
18
Effectiveness of Peer Education Interventions for HIV Prevention in Developing Countries Medley et al. (2009) AIDS Education and Prevention Review and meta-analysis – – n =30 peer ed interventions in low/middle income countries – –January 1990 and November 2006 Significant Findings – – HIV knowledge (OR: 2.28; 95% CI: 1.88, 2.75) – – IDU equipment sharing (OR: 0.37; 95% CI: 0.20, 0.67) – – condom use (OR: 1.92; 95% CI: 1.59, 2.33) – –Non-significant on STIs (OR: 1.22; 95% CI:0.88, 1.71) Conclusion – –“Meta-analysis indicates that peer education programs in developing countries are moderately effective at improving behavioral outcomes but show no significant impact on biological outcomes. Further research is needed…”
 AIDS Education and Prevention Review and meta-analysis – – n =30 peer ed interventions in low/middle income countries – –January 1990 and November 2006 Significant Findings – – HIV knowledge (OR: 2.28; 95% CI: 1.88, 2.75) – – IDU equipment sharing (OR: 0.37; 95% CI: 0.20, 0.67) – – condom use (OR: 1.92; 95% CI: 1.59, 2.33) – –Non-significant on STIs (OR: 1.22; 95% CI:0.88, 1.71) Conclusion – – Meta-analysis indicates that peer education programs in developing countries are moderately effective at improving behavioral outcomes but show no significant impact on biological outcomes. Further research is needed… .")
19
Effectiveness of peer interventions for youth Tolli (2012). Health Education Research Systematic review – –Peer education interventions for youth in European Union – –n=17 publications, involving only 5 studies – –January 1999 and May 2010 Conclusion – –A few statistically significant and non-significant changes – –“[O]verall, compared to standard practice or no intervention, there is no clear evidence of the effectiveness of peer education concerning HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people in the member countries of the European Union. Further research is needed…”

20
Project PAL Promoting Adherence for Life

21
$ 1.8 million 5-year NIMH-funded R01 Full randomized clinical trial based on pilot in the Bronx (Project HAART) 2 X 2 factorial design, with randomization to: –Buddy –Pager –Buddy & Pager –Standard of Care
 2 X 2 factorial design, with randomization to: –Buddy –Pager –Buddy & Pager –Standard of Care")
22
Recruitment and Eligibility Recruitment (2003-06) –Madison HIV Primary Care Clinic Harborview Medical Center, Seattle –Nurse specialist –Provider referrals Eligibility –At least 18 y.o. –Starting or switching antiretroviral medications –English-speaking –No significant cognitive impairment or active psychosis

23
Nurse Recruiting

24
Computer-Assisted Self-Interviews Patients completed CASI interviews at the clinic

25
Interviewing & Reimbursement Schedule CASI interviews: $60 at baseline, $20 at 2 weeks, $35 at 3, 6, and 9 months Telephone interviews at 2 and 4 months ($0) $35 bonus for returning the EDM cap and completing all 5 interviews $15 for each buddy mtg Patients could earn up to $240
 $35 bonus for returning the EDM cap and completing all 5 interviews $15 for each buddy mtg Patients could earn up to $240")
26
Conceptual Framework Affirmational Emotional Informational Satisfaction with Social Support Received Adherence Depression Regimen Knowledge Self- Efficacy

27
Main Measures Perceived social support (both general and adherence-specific) Self-efficacy to adhere Depression (CES-D) Knowledge of HAART 7-day self-report of missed doses (100% vs less) Electronic drug monitoring (MEMS) HIV-1 RNA VL and CD4 Count
 Self-efficacy to adhere Depression (CES-D) Knowledge of HAART 7-day self-report of missed doses (100% vs less) Electronic drug monitoring (MEMS) HIV-1 RNA VL and CD4 Count")
28
3-Month Buddy Intervention Components Bi-monthly Buddy Meetings Discuss adherence Problem-solve around life issues related to adherence Adopt a harm reduction approach to substance use Weekly Phone calls More in-depth individualized support Chance to broach more sensitive issues Better suited for participants with confidentiality concerns

29
Who were our buddies? Other HIV+ patients from the clinic who were… Adherent to a HAART regimen Willing to participate in initial training and ongoing supervision Socially skilled Able to commit for 6 months Referred by staff or self

30
Buddy Training Content of training –Setting boundaries –Barriers to accepting help –Strategies for adhering –Referring for medical issues –Assessing and referring for psychological distress –Assessing and providing social support Ongoing bi-monthly group supervision

31
Pager Intervention 3-month intervention period Patients in the pager arm received daily individualized text pages reminding them which med & how many to take (i.e., “informational support”) Messages customized to protect patients’ confidentiality Educational and entertainment message also Based on prior data showing the efficacy of alarms in adherence and high prevalence of “forgetting” doses
 Messages customized to protect patients’ confidentiality Educational and entertainment message also Based on prior data showing the efficacy of alarms in adherence and high prevalence of forgetting doses")
32
Standard of Care: Standard of Care: HAART Protocol CLINICIAN – –Talk about starting medications COUNSELOR – –Talk about the meds & why it is important to take them regularly, possible side effects, drugs interactions NUTRITIONIST – –Talk about the meds and their food requirements and how to use food to help control any of the side effects. SOCIAL WORKER – –Talk about things that could impact how you take your meds, including housing, finances, etc. CLINICIAN – –Again, talk about your readiness to start meds and answer any remaining questions. If you are ready, prescriptions will be written. PHARMACIST – –Answer any questions about your medications and confirm your knowledge and acceptance. Pick up 2-week supply of meds.

33
Flow of Participants Flow of Participants 223 enrolled SOC (n= 56)Buddy only (n= 58)Pager only (n= 56)Buddy & Pager (n= 53) 2 week (n= 52) 2 week (n=56) 2 week (n= 54) 2 week (n= 51) 2 month phone (n= 48) 2 month phone (n= 51) 2 month (n= 47) 2 month (n= 44) 3 month (n= 51) 3 month (n= 49) 3 month (n= 54) 3 month (n= 51) 4 month phone (n= 49) 4 month phone (n= 44) 4 month phone (n= 46) 4 month phone (n= 45) 6 month (n= 48; 2 pending) 6 month (n= 49; 1 pending) 6 month (n= 49; 1 pending) 6 month (n= 48; 0 pending) 9 month (n= 50; 3 pending) 9 month (n= 47; 5 pending) 9 month (n= 52; 3 pending) 9 month (n= 46; 5 pending)
Buddy only (n= 58)Pager only (n= 56)Buddy & Pager (n= 53) 2 week (n= 52) 2 week (n=56) 2 week (n= 54) 2 week (n= 51) 2 month phone (n= 48) 2 month phone (n= 51) 2 month (n= 47) 2 month (n= 44) 3 month (n= 51) 3 month (n= 49) 3 month (n= 54) 3 month (n= 51) 4 month phone (n= 49) 4 month phone (n= 44) 4 month phone (n= 46) 4 month phone (n= 45) 6 month (n= 48; 2 pending) 6 month (n= 49; 1 pending) 6 month (n= 49; 1 pending) 6 month (n= 48; 0 pending) 9 month (n= 50; 3 pending) 9 month (n= 47; 5 pending) 9 month (n= 52; 3 pending) 9 month (n= 46; 5 pending)")
34
Results

35
Baseline Socio-demographics Demographic Variable (N = 224) n (%) Gender Male Male Female Female Transgender Transgender 169 (75%) 53 (24%) 2 (1%) Race/ethnicity African-American African-American Hispanic Hispanic Caucasian Caucasian Other Other 67 (30%) 25 (11%) 105 (47%) 27 (12%) Education < High school degree < High school degree High school degree / GED High school degree / GED Some college / AA Some college / AA ≥ College graduate (BA/BS) ≥ College graduate (BA/BS) 47 (21%) 64 (29%) 93 (42%) 19 (9%) Employment Status Full or part-time Full or part-time Unemployed Unemployed 43 (19%) 180 (81%) Age (in years) Years since HIV diagnosis M (SD) 40.0 (8.2) 8.5 (6.7)
 n (%) Gender Male Male Female Female Transgender Transgender 169 (75%) 53 (24%) 2 (1%) Race/ethnicity African-American African-American Hispanic Hispanic Caucasian Caucasian Other Other 67 (30%) 25 (11%) 105 (47%) 27 (12%) Education < High school degree < High school degree High school degree / GED High school degree / GED Some college / AA Some college / AA ≥ College graduate (BA/BS) ≥ College graduate (BA/BS) 47 (21%) 64 (29%) 93 (42%) 19 (9%) Employment Status Full or part-time Full or part-time Unemployed Unemployed 43 (19%) 180 (81%) Age (in years) Years since HIV diagnosis M (SD) 40.0 (8.2) 8.5 (6.7)")
36
Overall Adherence 2 weeks 3 months 6 months 9 months BLPostF/UF/U Missed doses %% 074666260 1-2 1-218202121 3+ 3+8141719 How many doses of your HIV medication did you miss in the last 7 days?

37
Socio-demographic Correlates of Adherence Socio-demographic Correlates of Adherence At 3 months, employed participants were more likely to report 100% adherence than unemployed participants (85.4% vs. 70.6%), χ 2 (1) = 3.70, p =.05 At 3 months, African Americans were less likely than other participants to report 100% adherence (53.2% vs. 71.6%), χ2(1) = 6.39, p =.01 (Adherence not correlated with gender, income, education, relationship status.)
, χ 2 (1) = 3.70, p =.05 At 3 months, African Americans were less likely than other participants to report 100% adherence (53.2% vs. 71.6%), χ2(1) = 6.39, p =.01 (Adherence not correlated with gender, income, education, relationship status.).")
38
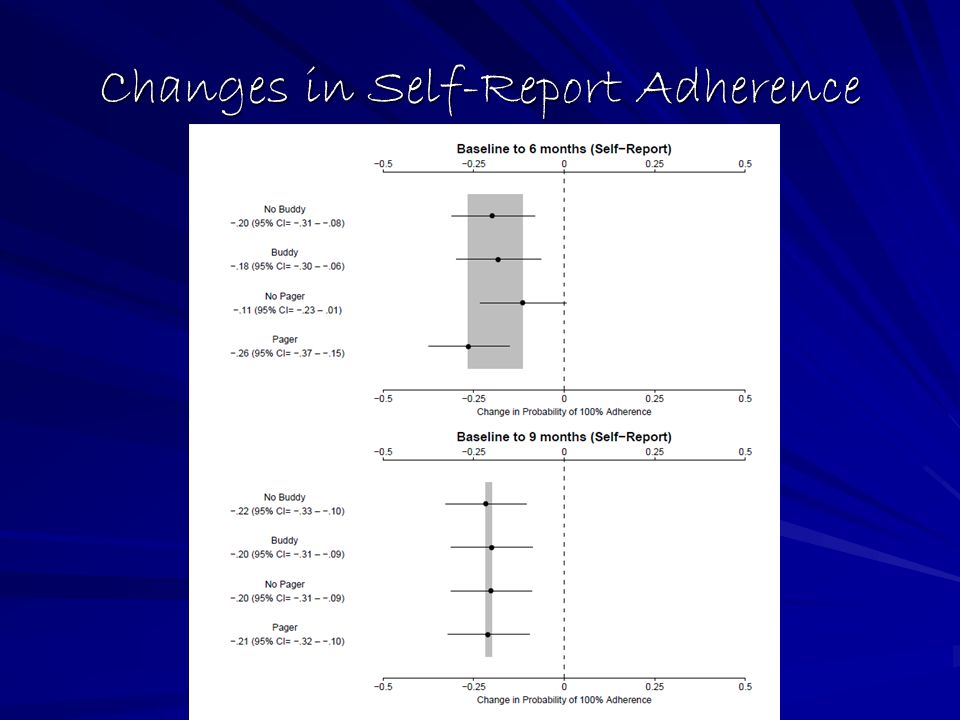
Does Intervention Improve Adherence? Self-Report Self-Report Those receiving buddy support were more likely to have not missed doses in the week prior to post-intervention assessment. Odds ratio = 2.1, p =.02 Those receiving buddy support were more likely to have not missed doses in the week prior to post-intervention assessment. Odds ratio = 2.1, p =.02 No effect for either buddy or pager intervention at 6 or 9- month follow-up No effect for either buddy or pager intervention at 6 or 9- month follow-up

39
Trends in Self-Report Adherence - Buddy - No Buddy - Pager - No Pager Shaded regions = 95% CI

40
Changes in Self-Report Adherence

42
Intervention Effects – EDM Adherence Intervention Effects – EDM Adherence Those receiving buddy support had a trend towards taking more doses in the week prior to post-intervention assessment. Estimate = 8.9%, p =.11

43
Trends in EDM Adherence - Buddy - No Buddy - Pager - No Pager Shaded regions = 95% CI

44
Changes in EDM Adherence

46
Biological Markers A priori findings A priori findings No significant effect of intervention on No significant effect of intervention on Change in CD4 count Change in CD4 count Achieving undetectable viral load Achieving undetectable viral load

47
Were participants engaged in the interventions? Pager support Pager support Range: 0 to 96.5% Range: 0 to 96.5% Mean: 41.1% (SD= 31.1%) Mean: 41.1% (SD= 31.1%) Buddy support Buddy support Range: 0 to 6 meetings attended Range: 0 to 6 meetings attended Mean: 2.8 meetings (SD= 2.2) Mean: 2.8 meetings (SD= 2.2)
 Mean: 41.1% (SD= 31.1%) Buddy support Buddy support Range: 0 to 6 meetings attended Range: 0 to 6 meetings attended Mean: 2.8 meetings (SD= 2.2) Mean: 2.8 meetings (SD= 2.2).")
48
Biological Markers – Post hoc Among pager participantshigher pager response rate was associated with: Among pager participants, higher pager response rate was associated with: Greater CD4 count at 3, 6, 9 months. Greater CD4 count at 3, 6, 9 months. ↑10% pager response → ↑12-23 CD4 (p’s <.05) ↑10% pager response → ↑12-23 CD4 (p’s <.05) Lower viral load 3 and 9 months Lower viral load 3 and 9 months ↑10% pager response → ↓0.1 Log 10 VL (p’s <.05) ↑10% pager response → ↓0.1 Log 10 VL (p’s <.05)
 ↑10% pager response → ↑12-23 CD4 (p’s <.05) Lower viral load 3 and 9 months Lower viral load 3 and 9 months ↑10% pager response → ↓0.1 Log 10 VL (p’s <.05) ↑10% pager response → ↓0.1 Log 10 VL (p’s <.05).")
49
Biological Markers – Post hoc Among buddy participants, greater attendance of peer support meetings was associated with… Among buddy participants, greater attendance of peer support meetings was associated with… A trend towards lower Viral Load at 3 and 6 months. A trend towards lower Viral Load at 3 and 6 months. ↑1 meeting → ↓0.1 – 0.2 log 10 VL (p’s <.10) ↑1 meeting → ↓0.1 – 0.2 log 10 VL (p’s <.10) Significantly lower Viral Load at 9 months Significantly lower Viral Load at 9 months ↑1 meeting →↓log 10 VL (p <.01) ↑1 meeting → ↓0.2 log 10 VL (p <.01)
 ↑1 meeting → ↓0.1 – 0.2 log 10 VL (p’s <.10) Significantly lower Viral Load at 9 months Significantly lower Viral Load at 9 months ↑1 meeting →↓log 10 VL (p <.01) ↑1 meeting → ↓0.2 log 10 VL (p <.01).")
50
Conclusions 1. Medication adherence starts off high and erodes over time for most patients. 2. An RCT testing buddy & pager adherence promotion strategies demonstrated some success during the first 3 months. –Specifically, those receiving buddy support (vs. those who did not) had greater likelihood of reporting 100% adherence in the 7 days prior to the 3-month post-intervention interview. –Electronic drug monitoring revealed a trend towards improved adherence for those receiving vs. not receiving buddy support.
 had greater likelihood of reporting 100% adherence in the 7 days prior to the 3-month post-intervention interview. –Electronic drug monitoring revealed a trend towards improved adherence for those receiving vs. not receiving buddy support..")
51
CDC Recognition Both Peer Support and Pager Support classified as interventions with “Good Evidence” by CDC and will be available online for distance learning implementations Two of the few evidence-based HIV medication adherence interventions identified in CDC’s systematic review of the literature from 1996 to 2009

52
Peer Support to Promote Medication Adherence Among People Living with HIV/AIDS: The Benefits to Peers Patricia Marino, PhD Jane M. Simoni, PhD Louise Bordeaux Silverstein, PhD Social Work in Health Care, Vol. 45(1) 2007
")
53
As part of the pilot Project HAART in the Bronx, NY, we conducted qualitative interviews with nine HIV-positive peers who had participated in an intervention designed to provide support to other HIV- positive individuals as one means of promoting antiretroviral therapy adherence. Analyses of the peers’ common dialogue about their involvement in the study revealed four main themes...

54
I. Social Acceptance Being with those who are going through the same thing (89%) I heard everyone was going through what I was going through and people felt the same way I did Feeling accepted within an otherwise isolating disease (56%) I know for sure I am not alone now Feeling safe in the program (67%) Whatever you said in that room stayed in that room
 I heard everyone was going through what I was going through and people felt the same way I did Feeling accepted within an otherwise isolating disease (56%) I know for sure I am not alone now Feeling safe in the program (67%) Whatever you said in that room stayed in that room.")
55
II. Reciprocal Support Support from peers (78%) You found something here they could not find no place else Receiving support on many levels (89%) Verbally we were able to talk about things they could not tell other people be it their husbands, moms, pops or children By helping other people I got something in return (100%) I found that they were there to listen to me. We helped each other Helping other people through example (89%) I was doing something for other people
 You found something here they could not find no place else Receiving support on many levels (89%) Verbally we were able to talk about things they could not tell other people be it their husbands, moms, pops or children By helping other people I got something in return (100%) I found that they were there to listen to me. We helped each other Helping other people through example (89%) I was doing something for other people.")
56
III. Personal Growth and Empowerment Feeling entitled enough to talk about disease (67%) Most people do not ask questions. I do not know whether we feel intimidated or we feel we are not going to know what they are talking about. The program made me feel like that is not true. Being part of project HARRT gave me strength (67%) It gave me confidence to look into more things because of the positive experience Change in outlook (78%) I am a totally different person now
 Most people do not ask questions. I do not know whether we feel intimidated or we feel we are not going to know what they are talking about. The program made me feel like that is not true. Being part of project HARRT gave me strength (67%) It gave me confidence to look into more things because of the positive experience Change in outlook (78%) I am a totally different person now.")
57
IV. Resistance and Other Challenges Obstacles to accepting support (100%) Certain people were just in denial and nothing you can say is going to change that Certain people you cannot help (56%) There was times when you could help certain people and certain people you cannot help No control over loss (56%) It knocked me for a loop because it did not enter my mind that I would lose somebody
 Certain people were just in denial and nothing you can say is going to change that Certain people you cannot help (56%) There was times when you could help certain people and certain people you cannot help No control over loss (56%) It knocked me for a loop because it did not enter my mind that I would lose somebody.")
58
Conclusions: Benefits and Challenges of Peer Support

59
Benefits of Peer Support To clients: –Can provide a specific type of support –Can target “hard-to-reach” populations –Good for those who fear stigma –Can take a harm reduction approach –Some beneficial effects on HIV outcomes demonstrated To peers themselves: –Peers can benefit (helper-therapy principle) –Empowerment –Training and possible employment –Sustained health outcomes
 –Empowerment –Training and possible employment –Sustained health outcomes")
60
Negatives of Peer Support To clients: –Peers overstepping – dispensing medical advice –Harm to clients through peers’ inexperience or lack of skills –Boundary violations (peers vs. friends/lovers) –Breaches of confidentiality –Legal liability To peers themselves: –Peers experience personal failure/loss when clients do not progress –Peers’ own health challenges –Risk for relapse
 –Breaches of confidentiality –Legal liability To peers themselves: –Peers experience personal failure/loss when clients do not progress –Peers’ own health challenges –Risk for relapse.")
61
Recommendations Broaden opportunities for peers Strengthen training Conduct process evaluations Examine systematically peer activities Rigorously evaluate program outcomes Disseminate and sustain successful programs

62
Future Notes from the Field: What might be useful for clinical practice?

63
Peer Selection Key Criteria –Social and communication skills –Compassion, empathy, non-judgmental attitude towards others’ lifestyles –Acceptable to and respected by target group –Willingness to commit to training and a minimal length of participation –Experience with ART (not necessarily successful – struggles can lead to empathy and solutions) –Stable recovery from substance dependency
 –Stable recovery from substance dependency")
64
Training of Peers - 1 Methods –Skills-based training –Adult learning principles –Mix presentation of information, practice of skills, constructive feedback on skills –Trusting environment for disclosing and reflecting on experiences relevant to peer work –Refreshers, updates, advanced workshops

65
Training of Peers - 2 Topics –Communication skills Active listening Conflict resolution –Peer roles on multidisciplinary teams –Disclosure –Defining and enforcing boundaries –Transference/countertransference –Self-care –Back-to-work issues

66
HIV Peer Training Resources HRSA-funded HIV Peer Educator Training Sites (California, Missouri, New York) – curricula and information available at http://www.hdwg.org/peer_center/ http://www.hdwg.org/peer_center/ Family Health International/YouthNet Youth Peer Education Toolkit Training of Trainers Manual
 – curricula and information available at Family Health International/YouthNet Youth Peer Education Toolkit Training of Trainers Manual")
67
Recruitment Strategies Elicit recommendations from –Target client population Announce search for peer candidates at Community Advisory Boards (CABs) and other patient organizations Ask community leaders and activists to suggest candidates –Experienced peers Peers can identify former clients, fellow patients, fellow members of AA, NA, or support groups –Medical and other providers Ask a member of the client population to confirm providers’ recommendations of patients and clients Advertise for self-referrals –CAB and other patient organizations –Central community gathering places –Explain desired characteristics and requirements
 and other patient organizations Ask community leaders and activists to suggest candidates –Experienced peers Peers can identify former clients, fellow patients, fellow members of AA, NA, or support groups –Medical and other providers Ask a member of the client population to confirm providers’ recommendations of patients and clients Advertise for self-referrals –CAB and other patient organizations –Central community gathering places –Explain desired characteristics and requirements")
68
Key Elements of Peer Support in Adherence Interventions – 1 Trusting relationships –Emotional support: help clients process emotional reactions to HIV status, illness, medication, disclosure –Social support: cultivate social networks and norms supportive of adherence and related behavior changes –Model adherence, healthy behaviors, good communication with providers Education and mentoring –Personalize education with examples from peers’ own history –Provide practical advice for integrating adherence into daily life –Recognize and celebrate progress towards adherence

69
Key Elements of Peer Support in Adherence Interventions – 2 Patient Navigation and Advocacy –Identify health and social service needs, facilitate referrals –Accompany client to medical and other appointments –Identify resources for resolving issues important to clients, e.g. insurance, benefits, immigration status

70
Formats for Peer Support One-on-one support –Frequent (weekly) contact, in person, phone, or e-mail facilitates the development of trusting relationships –With support from supervisor, may take place off-site in location where a client feels safe –Discussion of adherence may come after peer-client relationship is established over several weeks Group support –Support groups led by trained peers help normalize HIV status, overcome isolation, foster norms supportive of adherence, present peer as role model –Educational sessions present information tailored to clients in culturally appropriate styles Multidisciplinary teams –Peers complement professionals’ services –Clarify and reinforce information from providers –Bring unique insights and information to team
 contact, in person, phone, or facilitates the development of trusting relationships –With support from supervisor, may take place off-site in location where a client feels safe –Discussion of adherence may come after peer-client relationship is established over several weeks Group support –Support groups led by trained peers help normalize HIV status, overcome isolation, foster norms supportive of adherence, present peer as role model –Educational sessions present information tailored to clients in culturally appropriate styles Multidisciplinary teams –Peers complement professionals’ services –Clarify and reinforce information from providers –Bring unique insights and information to team")
71
Supervising Peers Collaborate with peers to develop specific job skills, responsibilities, and expectations that correspond to their unique qualifications Use ‘teach back’ techniques to ensure that peers fully understand their role Customize recording forms to document all aspects of peer activities and for ease of use Provide individual or group ‘supportive supervision’ to reflect on peer’s emotional reactions to client interactions and develop skills and expertise Encourage peers to develop their own support network through support groups for peers, ongoing workshops, or opportunities to socialize with fellow peers

72
Resources for Peer Supervisors ‘Peer Support for HIV Treatment Adherence: A Manual for Program Managers and Supervisors of Peer Workers.’ Mannheimer et al, 2003. Available at www.peerNYC.org www.peerNYC.org Coping with Hope: HIV Treatment Decisions/Adherence. A multidisciplinary Mental Health Services Curriculum,’ USDHHS Center for Mental Health Services et al, 2000. Available at www.aidsetc.org www.aidsetc.org Training in multidisciplinary team development, including peers, through Cicatelli Associates, Inc., www.cicatelli.org www.cicatelli.org ‘Integrating Peers into Multidisciplinary Teams: A Toolkit for Peer Advocates’ and ‘Supervisors’ Guide’. Cicatelli Associates Inc., 2007

73
Compensation Recommended if programs are to be sustainable –Free time to the project means less earning time Compensatory options At minimum provide meals and expenses Monetary or non-salary incentives –T-shirts, bicycles, access to loans, free medical care, and/or the status of being a peer educator. Opportunities for recognition Increased responsibilities and decision-making authority Opportunities for personal and professional growth –Compensation must be relative to avoid creating social distance between the peer and the intended audience Compensation is needed to improve job satisfaction, retention rates, and program sustainability

74
Retention Strategies Skills assessment and staff development plan –Conduct periodic individual and group support sessions with peer educators to address stress, burnout, and other psychological aspects as well as to share successes and ideas Provide peer volunteers with ongoing educational sessions and opportunities to "socialize" with other volunteers Involve peer educators in decision-making and giving them broader responsibilities related to program design, implementation, and evaluation

75
Acknowledgements Co-investigators –Thomas (Mac) Hooten, Marc Gourevitch, Bu Huang, Cynthia Pearson, Pamela Frick Schwartz, Karina Walters Consultants –Laurie Bauman, Seth Kalichman, Gary Marks, Research assistants at Yeshiva University –Mary Alm, Oshra Cohen, Nina Cooperman, Patricia Marino, Sara Mott, Michelle L. Monaco, E. Cathrine Strugstad Research assistants at UW –Alison Wilhelm, Mary Plummer, David Pantalone, Heidi Montoya, Dellanira Valencia-Garica, David Huh, Keren Lehavot, Sam Yard, Kim Nelson, Bryan Kutner Staff and undergraduate students Particpants!!

76
UW LAB

77
Ontario HIV Treatment Network Thank you and I wish you well in your work!

78
Thank you

79
End of presentation Jane Simoni jsimoni@uw.edu For copies of this presentation or to join the adherence listserv

80
What’s next? 10:15a.m.Break/Networking/Poster Sessions (Foyer) 10:15a.m.Visual Story Galleries (Foyer, Richmond, University, Adelaide)
 10:15a.m.Visual Story Galleries (Foyer, Richmond, University, Adelaide).")
Similar presentations















 Richard Wolitski, Cynthia Gomez, Jeffrey Parsons, and the SUMIT Study Group Prevention Interventions.>")




