Download presentation
Presentation is loading. Please wait.

1
ANGIOGRAPHY AND OTHER IMAGING TECHNIQUES Claudio Rabbia Claudio Rabbia Department of Vascular and Interventional Radiology Molinette Hospital Turin

2
ANGIOGRAPHY Mesenteric angiography is the most accurate modality for the diagnosis of acute lower gastrointestinal bleeding Mesenteric angiography is the most accurate modality for the diagnosis of acute lower gastrointestinal bleeding inferior mesenteric artery (IMA) The earliest description of angiographic demonstration of GI bleeding was in 1963. Since that time angiography has been used in evaluation of GI bleeding, though with varying frequency over time and with the advent of colonoscopy and scintigraphy

3
When and why to perform a diagnostic angiography? Massive LGI bleeding Inability to perform colonoscopy Failure of colonoscopy to reveal site of bleeding ( up to 52% of cases) Recurrent or persistent bleeding Subsequent endovascular therapy
 Recurrent or persistent bleeding Subsequent endovascular therapy.")
4
ANGIOGRAPHY bleeding rate of at least 0.5 ml/min accurate localization of bleeding source (27-86%) vasodilators, heparin or thrombolytic agents increase the sensitivity from 32 to 65%
 vasodilators, heparin or thrombolytic agents increase the sensitivity from 32 to 65%")
5
ANGIOGRAPHY Screen film arteriography Screen film arteriography DSA: higher sensitivity but artifacts DSA: higher sensitivity but artifacts by bowel motion by bowel motion Parasympathicolysis Suspended respiration

6
ANGIOGRAPHY occasionally specific diagnosis planning operative resection opportunity for nonsurgical therapy

7
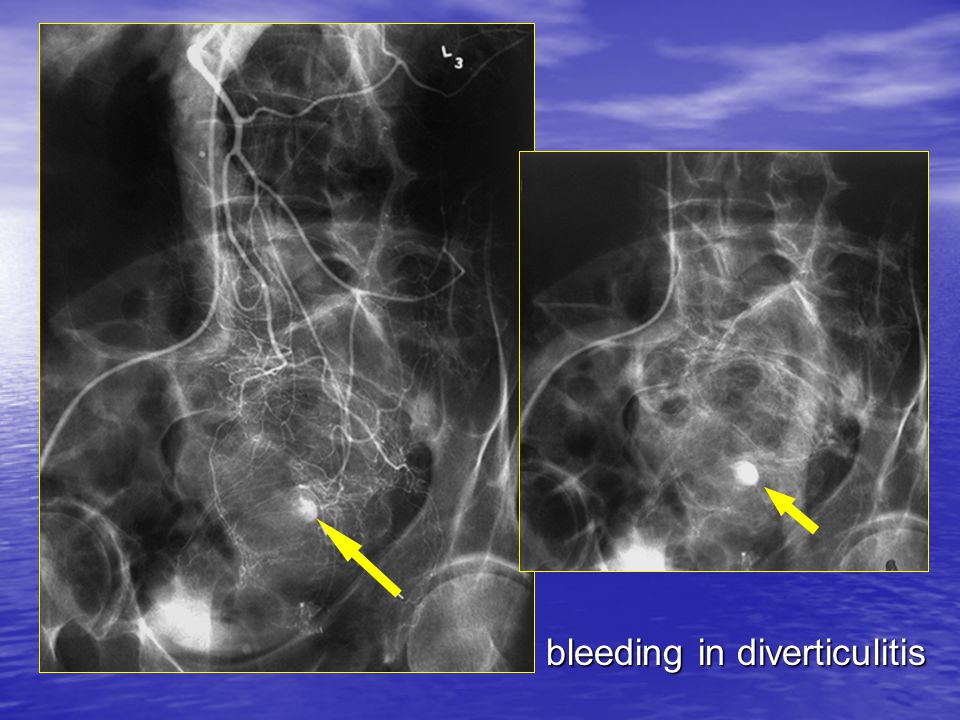
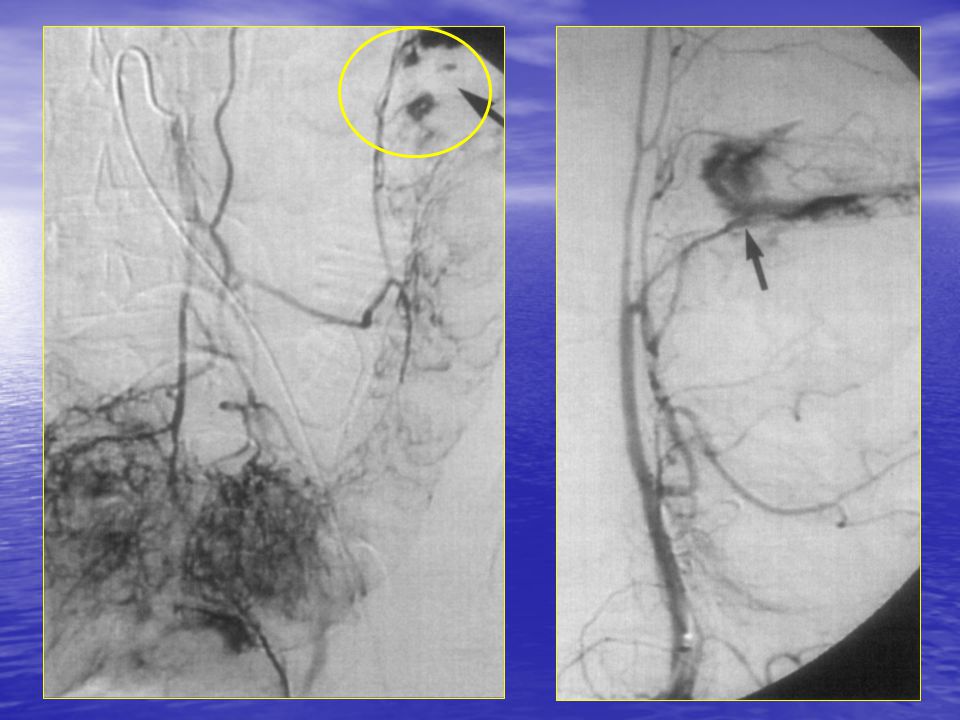
ANGIOGRAPHIC findings active extravasation of contrast material within the bowel lumen pseudoaneurysm pathologic circulation – increase of vascularization leiomyoma angiodysplasia

8
bleeding in diverticulitis

12
ANGIOGRAPHY clinical sensitivity Typical values are around 60% Attempts to identify predictors for positive angiographic findings have shown mixed results Attempts to identify predictors for positive angiographic findings have shown mixed results

13
Are there factors to predict which patients will benefit from angiography? a 12-year period review A positive bleeding scan did not increase the percentage of positive angiograms History of prior GI bleeding, transfusions, orthostatic hypotension or tachycardia were not predictors for a positive angiogram Pennoyer WP, Dis Colon Rectum 1997

14
Are there factors to predict which patients will benefit from angiography? Strong correlation with a systolic blood pressure <100 mmHg immediate arteriography rather than nuclear medicine in hemodynamically unstable patients immediate arteriography rather than nuclear medicine in hemodynamically unstable patients Nicholson ML, Gut 1998

15
COMPUTED TOMOGRAPHY At this time CT is not commonly performed for diagnosis of acute GI bleeding BUT “Acute Massive Gastrointestinal Bleeding: Detection and Localization with Arterial Phase Multi–Detector Row Helical CT” Yoon W et al Radiology 2006

16
Arterial phase contrast enhanced MDCT - advantages Rapid: very short acquisition time Non invasive Accurate in detection and localizing sites of acute GI bleeding (arterial phase images)
")
17
Technical aspects 120-140 mL of contrast medium (350 mg/mL of iodine) Time of acquisition: 20-25 sec Nominal section thickness: 1.5 mm No three-dimensional reconstruction Delayed (portal phase) scans usually not performed
 Time of acquisition: sec Nominal section thickness: 1.5 mm No three-dimensional reconstruction Delayed (portal phase) scans usually not performed")
18
MDCT (multi detector computed tomography) Compared to angiography as the reference standard Sensitivity: 90% Specificity: 99% Accuracy: 100% for localization Yoon W, Radiology in press for detection }
 Compared to angiography as the reference standard Sensitivity: 90% Specificity: 99% Accuracy: 100% for localization Yoon W, Radiology in press for detection }")
19
MDCT findings Collection of contrast material within the bowel lumen or extravasated contrast material (greater than 90 HU) Focal dilatation of fluid filled bowel segment In addition ability to demonstrate morphologic changes in the GI tract (tumors, polyps)
 Focal dilatation of fluid filled bowel segment In addition ability to demonstrate morphologic changes in the GI tract (tumors, polyps)")
20
MDCT findings morphologic changes Preliminary unenhanced CT scan to detect preexisting hyperattenuating material Preliminary unenhanced CT scan to detect preexisting hyperattenuating material Suture material

21
MDCT findings morphologic changes Polipoid lesion in the sigmoid colon

22
colon adenocarcinoma in the sigmoid colon MDCT findings morphologic changes

23
MDCT findings morphologic changes

24
MDCT findings active extravasation MDCT during arterial phase to identify active extravasation of contrast material within the bowel lumen MDCT during arterial phase to identify active extravasation of contrast material within the bowel lumen

25
MDCT findings

26
ANGIOGRAPHY AND MDCT which better? The major drawback is that their rate of detection is influenced by several factors, including the rate of bleeding at the time of imaging and the timing of imaging. Sites of bleeding cannot be demonstrated even in patients with massive GI bleeding because of its intermittent nature. There is no “gold standard” method as reference

27
MDCT advantages and limits Advantages Noninvasiveness and rapidity High accuracy of arterial phase MDCT MDCT may guide further endovascular intervention Delayed selective injection during angiographyLimits Impaired renal function Artifacts may obscure extravasation Lack of therapeutic capability (angiography, endoscopy, surgery)
")
29
time 0 5’ later

30
limitations of combining MDCT and angiography include large amount of contrast medium and costs

31
MAGNETIC RESONANCE MRI has a limited role in the evaluation of acute LGIB from arterial sources. In the setting of aneurysms and pseudoaneurysm, magnetic resonance angiography (MRA) may be helpful in depicting small vascular abnormalities.
 may be helpful in depicting small vascular abnormalities..")
32
Comparison of three dimensional magnetic resonance imaging in conjunction with a blood pool contrast agent and nuclear scintigraphy for the detection of experimentally induced gastrointestinal bleeding 100% sensitivity and specificity of 3D MR with intravascular contrast agent Strong difference in diagnostic performance in ROC analysis in favour of MR imaging Hilfiker PR Gut 1999

33
MAGNETIC RESONANCE limitations Lower spatial resolution ( compared with MDCT) Longer acquisition time Limited availability of equipments for GI emergency
 Longer acquisition time Limited availability of equipments for GI emergency")
34
conclusions With new CT technology, probably MDCT will represent first imaging technique in LGI bleeding Further angiography is mandatory if endovascular treatment is needed Currently there is no indication for MR imaging

Similar presentations





>")







 Sensitive indicator of perfusion Diagnosis and prognosis of.>")







